All published articles of this journal are available on ScienceDirect.

Prevalence of Carotid Artery Calcification Detected on Panoramic Radiographs of Patients with a History of Hypertension or Myocardial Infarction
Authors Info & Affiliations
Abstract
Background:
Atherosclerosis is characterized by the deposition of lipids on the internal walls of blood vessels, damaging various tissues of the body by complete or partial occlusion of the vessels. Sometimes the calcified plaques in the carotid artery can be detected on panoramic radiographs, helping the practitioners decrease the risk of Cerebrovascular Accident (CAV).
Objective:
This study aimed to assess the frequency of Carotid Artery Calcification (CAC) detected in panoramic radiographs of patients with hypertension or myocardial infarction.
Methods:
A total of 400 panoramic radiographs of patients >40 years of age were evaluated. The images belonged to patients with a history of hypertension or myocardial infarction and healthy individuals referred from the AL Zahra Cardiology Department to Isfahan School of Dentistry and a private oral and maxillofacial imaging center. All the images were evaluated for the presence of CAC. Data were analyzed with SPSS 19, using the Chi-squared test, Fisher's exact test, t-test and ANOVA (α=0.05).
Results:
The prevalence rate of CAC was 4%. According to the results, there was a significant relationship between CAC and hypertension (P=0.003), with no significant relationship between the prevalence of these lesions, stage of hypertension and myocardial infarction.
Conclusion:
According to the results, the prevalence of CAC on panoramic radiographs was significant; therefore, it seems that the detection of CAC on panoramic radiographs of patients must be considered by dentists.
1. INTRODUCTION
Atherosclerosis is a chronic inflammatory disease characterized by the formation of fatty fibrous plaque on the internal walls of blood vessels, which progress and occlude various blood vessels in the body. Formation of atheroma in carotid and coronary arteries causes severe complications such as limb paralysis and slurred speech and in severe cases might be fatal [1, 2].
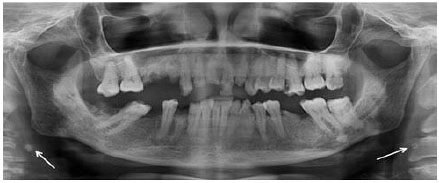
Panoramic radiography is an extraoral radiographic technique commonly used as a diagnostic tool in dentistry. Except for routine applications such as the evaluation of teeth, the remaining roots, jaw fractures, etc., panoramic radiographs can be applicable for the detection of calcified athermanous lesions but due to the presence of various anatomical structures which might be superimposed on the lesion, such as hyoid bone, thyroid cartilage, styloid process, epiglottis cartilage, posterior aspect of the tongue, soft palate, ear lobe, calcified acne, etc., diagnosis is difficult and requires adequate experience and knowledge. The Carotid Artery Calcification (CAC) usually appears as a radiopaque nodular mass, which is present in the intervertebral space between the 3rd and 4th cervical vertebrae (Fig. 1) [3].
In 2014, Moshfeghi et al. [4] evaluated the relation between CAC, hypertension and myocardial infarction; 200 female patients were selected, who were >40 years of age. The panoramic radiographs of the patients were evaluated and their medical history was also collected. Finally, of 200 subjects, 22 exhibited CAC (11%), 11 had a history of hypertension and three had a history of myocardial infarction.
In 2008, Mehdizade and Naghavi [5] evaluated the prevalence of CAC in patients >50 years of age in Isfahan, Iran; 400 individuals were selected and assessed for the presence of CAC, a history of diabetes mellitus, hypertension and myocardial infarction. The results showed a significant relationship between the prevalence of CAC and gender (more in females) and diabetes mellitus.
In 2009, Khosroanah et al. [6] assessed panoramic radiographs and color Doppler of 90 patients for the presence of CAC in Namazi Hospital and compared them together during the period of 11 months. The results showed significant accuracy of panoramic radiographs in the detection of CAC (66.6%).
In 2003, Ohba et al. selected 659 individuals >80 years of age in Japan for assessing the prevalence of CAC on panoramic radiographs. Of 659 subjects, 33 were CAC-positive [7].
In 2006, Damrongsri and Tanakon evaluated panoramic radiographs of 1370 patients selected from the Oral and Maxillofacial Radiology Department in Mahidol University; 34 subjects exhibited CAC, 16 and 17 of whom were male and female, respectively [8].
Due to the increasing risk of Cerebrovascular Accident (CAV) in populations, this study aimed to use panoramic radiographs in the detection of CAC in individuals suffering from hypertension and myocardial infarction, which are two most important etiologic factors of atherosclerosis. The results of this study might help dental practitioners lower the risk of CAV by early detection and referral of affected patients to a specialist.
2. MATERIALS AND METHODS
In this study, 400 panoramic radiographs were selected and evaluated for the presence of CAC. All the images were taken for treatment purposes and none of them were taken for CAC detection. Knowledge and full consent of patients were essential and their participation was free of any cost. All the radiographs were taken by a digital system under the same terms and conditions with high diagnostic value (without overexposure and underexposure).
The subjects were individuals >40 years of age, with a history of hypertension or myocardial infarction and healthy individuals in equal numbers. The history of hypertension and myocardial infarction of patients was assessed and approved by a cardiologist and sent to the Department of Oral and Maxillofacial Radiology for imaging. The images of healthy individuals were collected from the archives of a private oral and maxillofacial radiology center.
The CAC usually appears as a radiopaque nodular mass, which is present in the intervertebral space between the 3rd and 4th cervical vertebrae.
The presence of CAC was confirmed by an oral and maxillofacial radiologist. Data were analyzed by SPSS 19, using the Chi-squared test, Fisher's exact test, t-test and ANOVA [9, 10].
3. RESULTS
The samples included 240 males (60%) with a mean age of 61 years and 160 females with a mean age of 60 years (40%). The T-test showed no significant differences between the mean ages and gender between the subjects (P=0.349).
Distribution of CAC in terms of myocardial infarction, hypertension and gender and the stage of hypertension in both genders is available in Tables 1 and 2. According to the obtained results, more CACs were detected on the left side, indicating that the left carotid artery seems to be affected at a higher rate (4%). According to Fisher's exact test, there was no significant relation between CAC and a history of myocardial infarction (P=0.010). The Chi-squared test showed there was a significant relationship between the prevalence of CAC and a history of hypertension (P=0.003) and there was no significant relationship between CAC and gender (P=0.061). Based on the t-test, there was no significant relationship between the mean of age and the presence of CAC (P=0.913), between mean age and a history of myocardial infarction (P=0.161), and there was a significant relationship between hypertension and mean age (P=0.028). The Chi-squared test showed there was a significant relationship between hypertension and gender (P=0.018) and between a history of myocardial infarction and gender (P=0.001). According to the Chi-squared test, there was no significant relationship between hypertension and gender (P=0.160). Due to the Fisher's exact test, there was a significant relationship location between CAC and gender (P=0.046). According to ANOVA, there was no significant relationship between the mean age and location of CAC (P=0.236) and between the stage of hypertension and mean age (P=0.164).
| CAC | Myocardial Infarction | Hypertension | Gender | |||
|---|---|---|---|---|---|---|
| Yes | No | Yes | No | Female | Male | |
| Present | 4 (3.6%) | 12 (4.1%) | 5 (1.9%) | 11 (8.1%) | 6 (2.5%) | 10 (6.3%) |
| Absent | 106 (96.4%) | 278 (95.9%) | 260 (98.1%) | 124 (91.9%) | 234 (97.5%) | 150 (93.8%) |
| Total | 110 (100%) | 290 (100%) | 265 (100%) | 135 (100%) | 240 (100%) | 160 (100%) |
| Stage of hypertension | Female | Male |
|---|---|---|
| Stage 1 | 31 (19.4%) | 36 (15%) |
| Stage 2 | 26 (16.3%) | 26 (10.8%) |
4. DISCUSSION
Intervertebral spaces in all the panoramic radiographs were checked for the presence of CAC. CAC is usually detected in the 3rd and 4th intervertebral space; thus, all the obvious radiopaque nodular masses in this space are considered as suspected views of CAC. The calcified structures above or below the above-mentioned space were not considered as CAC in our study. The medical history of all the patients and their effect on hypertension and myocardial infarction were checked and approved by a cardiologist.
Previous studies have reported a prevalence of 5%, 6.2% and 11% for CAC on panoramic radiographs [3-5]. The relationships between CAC incidence and its risk factors in all ages in both genders have also been evaluated.
Moshfeghi et al. evaluated 200 panoramic radiographs and medical histories of CAC-positive cases and reported a significant relationship between CAC and hypertension and myocardial infarction [4], which were in agreement with our results. The prevalence of CAC on panoramic radiographs was 11%, which is higher than that in our study; the reason might be attributed to differences in ethnicity, quality of radiographs, exposure conditions and experience in detecting these lesions on panoramic radiographs. Moshfeghi et al. reported a relationship between CAC and myocardial infarction [4], which is different from the results of the present study.
Mehdizadeh and Aghavi assessed 400 panoramic radiographs and, in contrast to our study, reported a significant relationship between CAC and gender; in addition, there was a strong relationship between diabetes and CAC [5], which is not evaluated in the present study. However, the relationship between CAC and hypertension was confirmed in both studies.
According to Damrongsri and Bayer’s studies, a significant relationship was found between CAC and gender (more in females), unlike the current study [8]. The reason for the discrepancy might be the small sample size.
Based on a study by Ohba et al., unlike our research, there was no significant relationship between CAC and a history of hypertension [7], which can be attributed to differences in ethnicity, quality of radiographs, exposure conditions and experience in the detection of these lesions on panoramic radiographs.
Other items evaluated in our study were the stage of hypertension and the location of CAC in the samples, which have not been assessed in any other study yet. The stage of hypertension was checked by a cardiologist and the location of CAC in panoramic radiographs was confirmed by an oral and maxillofacial radiologist.
Khosropanah et al., in 2009, studied 90 panoramic radiographs and color Doppler of the same individuals for the detection of CAC [6]. After extracting data and comparing them together, they reported that the accuracy of panoramic radiographs in the detection of CAC was significant and recommended their use as a primary diagnostic tool for the same purpose. However, according to the study of Almog et al., the risk of wrong detection is high in inexperienced clinicians [11], which can result in unnecessary and costly procedures for the patients; therefore, the detection of CAC on panoramic radiographs is quite difficult and requires adequate experience and knowledge due to the superimposition of anatomical structures.
The limitation of the present study was the dissatisfaction of patients and the small sample size. Due to differences in the prevalence of CAC on panoramic radiographs in different populations and races, we suggest further studies with larger sample sizes. Due to the importance of the subject in decreasing the incidence of CVA by dental practitioners, we suggest further studies in the diagnosis of calcified carotid artery plaque on panoramic radiographs for dental students.
CONCLUSION
According to the results of the present study, the prevalence of carotid artery calcification on panoramic radiographs was significant; therefore, it seems that the detection of CAC on panoramic radiographs of dental patients must be considered by dentists.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of the Isfahan University of Medical Science, Iran (Code 395698).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The participants provided written informed consent to be involved in this study.
AVAILABILITY OF DATA & MATERIAL
The data sets analyzed during the current study are available from the corresponding author on request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors thank the participants for being involved in this study.
REFERENCES
Availble on: /j/hmbci.2017.31.issue-3/hmbci-2017-0019/hmbci-2017 -0019.xml

