All published articles of this journal are available on ScienceDirect.

Effects of Different Application Techniques on Nanohybrid Composite Restorations Clinical Success
Abstract
Introduction:
Dental composites have been used as a restorative material for a long time. However, they have their limitations.
Aims:
This study evaluated the effects of placement techniques on the clinical performance of class I composite resin restorations.
Methods:
A total of 40 patients with split-mouth design participated in this study. Each patient had two fillings according to the placement technique (either bulk or incremental packing) of the composite resin restorations. Group (A): was packed by Tetric EvoCeram bulk-fill composite resin and Group (B): was incrementally packed with Tetric EvoCeram composite resin. Restorations of the teeth were evaluated on the same day, at one week, 3 months and 6 months to determine any signs of failure according to the modified United States Public Health Service (USPHS) criteria.
Results:
At different follow-up periods, the results showed no significant differences for retention, marginal integrity, surface stain, gingival bleeding, and secondary caries; however, there were significant differences in color match, surface texture, and postoperative sensitivity.
Conclusion:
This study concluded that the nanohybrid resin composites demonstrated excellent clinical performance for 6 months follow up period.
1. INTRODUCTION
Dental composites are used as a restorative material since early 1960. The demand for posterior resin composite restorations has dramatically increased in recent years, because of their ability to match the tooth color, absence of mercury, biocompatibility and bond with the tooth structure [1]. However, like all dental materials, composites have their limitations, such as the gap formation caused by polymerization contraction during setting, leading to marginal discoloration and leakage [2]. In this decade, bulk-fill composites are becoming increasingly popular due to the clinical appeal of reducing the time necessary to insert the composite into the cavity [3]. The particularity of the new material category is stated to be the option to place it in 4 mm thick bulks instead of the current incremental placement technique, without negatively affecting polymerization shrinkage or cavity adaptation. Thus, problems related to polymerization shrinkages like gap formation causing secondary caries due to bacterial colonization, pulp irritation, and post-operative sensitivity could be minimized [4], continuous occlusal loading produces stresses on restorations, thereby increasing crack initiation and encouraging loss of these restorations. Thus, the selection of restorative materials represents a critical factor for successful restoration [5].
2. MATERIALS AND METHODS
This study evaluated the effects of placement techniques (Bulk, Incremental packing) on clinical performance of class I composite resin restorations.
In Table 1, a detailed description of the materials utilized in the study is presented, along with their composition and manufacturers. These include the different types of Tetric dental materials examined in the study.
| Material | Description | Composition | Manufacturer |
|---|---|---|---|
| Tetric Evo Ceram | Visible light cured nanohybrid Resin composite | The monmer matrix is composed of dimethacrylates (17-18%weight). The fillers contain barium glass, ytterbium trifluride, mixed oxide and prepolymer (82-83%weight), additives, catalysts, stabilizers and pigments (1% weight). | Ivoclar Vivadent |
| Tetric Evo Ceram Bulk Fill | Visible light cured nanohybrid Resin composite | Containing a highly reactive light initiator Ivocerin | |
| Tetric N-Etch | Etchant | Phosphoric acid (37 wt% in water) | |
| Tetric N-Bond Total-Etch | Single-component, Total-etching, light curing, nano-filled adhesive ystem | Phosphonic acid acrylate, HEMA*, Bis GMA**, urethane dimethacrylate, ethanol, nanofillers, catalysts and stabilizers. |
2.1. Clinical Procedures
A total of 40 patients were selected following a selection criterion; patients’ age range was 20-40 years, maintaining good oral hygiene measures (Brushing their teeth at least twice /day, using floss daily, no plaque or calculus deposition), two detected caries lesions on both posterior quadrants (right and left molars). Caries was detected by clinical inspection; following the ICDAS score of 3 or 4, as well as x-ray examinationfor lesion passing the DEJ spreading in the outer surface of dentin less than half-way to the pulp R3.
Ethical approval was obtained from the Imam Abdulrahman Bin Faisal University (IRB-2019- 234-Dent).
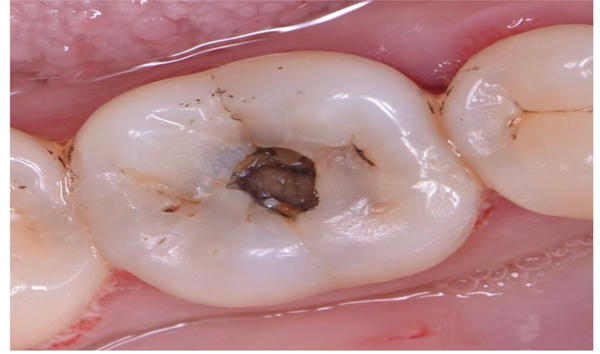
Each patient received two fillings according to the placement technique (either bulk or incremental packing) of the composite resin restorations. The patients signed an informed consent form before participating in the research. After shade selection, all operative procedures were performed under local anesthesia i.e. 2% Lidocaine Hydrochloride (Xylocaine 2%, Dentsply Sirona, York, Pennsylvania, United States). Conventional class I cavities were prepared. The average facio-lingual width of each preparation was equal to one-third of the distance between cusp tips; the width was measured using a graded periodontal prob. All the preparations were of simple class I cavities and the cavo-surface angles without any intentional bevel [6]. Only shallow and mid-sized cavity preparations were included in this study. (≤ 4mm). Deep cavity preparations were excluded due to the need for cavity liners for pulp protection [7]. A rubber dam (Dentsply Sirona, York, Pennsylvania, United States) was placed throughout the whole cavity preparation and restoration. Split-mouth design was used, in which Tetric EvoCeram Bulk Fill composite resin (Ivocalr Vivadent, Schaan, Liechtenstein) was placed in the left quadrant (Group A). It was placed in bulk following the manufacturer’s instructions. The composite was then light cured for 30 seconds using Bluephase Style LED light (Ivocalr Vivadent, Schaan, Liechtenstein). Tetric EvoCeram was placed in the right quadrant (group B) with incremental packing using a plastic instrument in two increments (1 mm thick each). The thickness of the increment was checked using a periodontal probe. Each increment was cured for 20 seconds using the same light cure. After polymerization of the restorations, the rubber dam was removed, and occlusal adjustment was performed in maximum intercuspation and eccentric movements, with the patient seated, so that the occlusal plane is parallel to the ground. The restoration was finished and polished using OptraPol finishing burs provided by the manufacturer (Ivocalr Vivadent, Schaan, Liechtenstein) under water cooling, (Figs. 1-3). Restorations were evaluated at the same day, at one week, 3 months and 6 months to determine any signs of failure according to the modified USPHS criteria (the United States Public Health Service criteria) [8] (Table 2).
| Criteria | Test Procedure | USPHS Score | – |
|---|---|---|---|
| Retention | Visual inspection with a mirror at 18 inches | Complete retention of the restoration Mobilization of the restoration, still present Loss of the restoration |
Alpha (A) Bravo (B) Charlie (C) |
| Colour match | Visual inspection with mirror at 18 inches |
Restoration is perfectly matched for color shade Restoration is not correctly matched for color shade Restoration is unacceptable for color shade |
Alpha (A) Bravo (B) Charlie (C) |
| Marginal integrity | Visual inspection with explorer and mirror, if needed |
Absence of discrepancy at probing Presence of discrepancy at probing, without dentin exposure Probe penetrates in the discrepancy at probing, with dentin exposure |
Alpha (A) Bravo (B) Charlie (C) |
| Marginal discoloration | Visual inspection with mirror at 18 inches |
Absence of marginal discoloration Presence of marginal discoloration limited and not extended Evident marginal discoloration penetrated towards the pulp chamber |
Alpha (A) Bravo (B) Charlie (C) |
| Surface texture | Visual inspection with explorer and mirror, if needed |
The surface is not rough Surface is slightly rough Surface is highly rough | Alpha (A) Bravo (B) Charlie (C) |
| Surface staining | Visual inspection with explorer and mirror, if needed |
The surface is not staining Surface is slightly staining Surface is highly staining | Alpha (A) Bravo (B) Charlie (C) |
| Postoperative sensitivity | Ask patients | Absence of the dentinal hypersensitivity Presence of mild and transient hypersensitivity Presence of strong and intolerable hypersensitivity |
Alpha (A) Bravo (B) Charlie (C) |
| Gingival bleeding | Visual inspection with explorer and mirror, if needed |
Gingival tissues are perfect Gingival tissues are slightly hyperaemic Gingival tissues are inflammatory |
Alpha (A) Bravo (B) Charlie (C) |
| Secondary caries | Visual inspection with explorer and mirror, if needed |
No evidence of caries Evidence of caries along the margin of the restoration |
Alpha (A) Bravo (B) |


2.2. Statistical Analysis
Restoration characteristics were described by descriptive statistics using frequency distributions of the scores. The Statistical Package for Social Sciences, version 21.0 (IBM SPSS Software, Chicago, Ill., USA) was used to process the data. 95% confidence interval was used and the level of significance was set at p<0.05.
3. RESULTS
The composite resin restorations were evaluated for retention, color match, marginal integrity, surface stain, surface texture, postoperative sensitivity, gingival bleeding, and secondary caries. The difference between the restorative material Tetric EvoCeram (bulk fill packing and incremental packing) at the end of 6 months was not statistically significant and demonstrated acceptable clinical performance. Meanwhile, there were some statistically different issues regarding the evaluation criteria between the follow-up periods:
3.1. Retention
The score was predominantly scored (A) at different follow-up periods for both the groups with a minor record for score (C) after 6 months follow up, as shown in Table 3. The difference between both the groups was non-significant (p= 0.0917>0.05). Similarly, the difference between different follow up periods was also non-significant (p=0.0561>0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 39 | 0 | 0 | 40 | 0 | 0 |
| One week | 39 | 0 | 0 | 40 | 0 | 0 |
| Three months | 36 | 0 | 0 | 38 | 0 | 0 |
| Six months | 37 | 0 | 2 | 37 | 0 | 1 |
3.2. Colour Match
As presented in Table 4, the score was predominantly recorded (A) at different follow-up periods for both the groups with a minor record for score (B) at different follow-up periods. The difference between both the groups was non-significant (p=0.391>0.05), whereas the difference between different follow-up periods was significant (p=0.006>0.05).
| Composite | Group A: Bulkfill Packing | Group B: Incremental Packing | ||||
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 40 | 0 | 0 | 40 | 0 | 0 |
| Three months | 38 | 0 | 0 | 38 | 0 | 0 |
| Six months | 37 | 0 | 0 | 37 | 0 | 0 |
3.3. Marginal Integrity
The score was predominantly recorded (A) at different follow-up periods for both the groups with a minor record for score (Ba) and no record for score (C) at different follow-up periods. In Table 5, it was observed that the difference between both the groups was non-significant (p=1>0.05). Similarly, the difference between different follow up periods was also non-significant (p=0.091>0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 40 | 0 | 0 | 40 | 0 | 0 |
| Three months | 38 | 0 | 0 | 38 | 0 | 0 |
| Six months | 37 | 0 | 0 | 37 | 0 | 0 |
3.4. Surface Stain
The score was predominantly recorded (A) at different follow-up periods for both the groups with no record for score (B) or (C) at different follow-up periods, as shown in Table 6. The difference between both the groups was non-significant (p=0.2917>0.05). Similarly, the difference between different follow up periods was also non-significant (p=0.4950>0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 35 | 1 | 0 | 38 | 2 | 0 |
| Three months | 37 | 1 | 0 | 38 | 0 | 0 |
| Six months | 35 | 2 | 0 | 37 | 0 | 0 |
3.5. Surface Texture
The score was predominantly recorded (A) at different follow-up periods for both the groups with a minor record for score (B) and no record for score (C) at different follow-up periods as presented in Table 7. The difference between both the groups was non-significant (p=0.391>0.05), whereas the difference between different follow-up periods was significant (p=0.0109<0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 40 | 0 | 0 | 40 | 2 | 0 |
| Three months | 37 | 0 | 0 | 38 | 0 | 0 |
| Six months | 36 | 1 | 0 | 37 | 0 | 0 |
3.6. Post-operative Sensitivity
The score was predominantly recorded (A) at different follow-up periods for both the groups with a minor record for score (Ba) and no record for score (C) at different follow-up periods. As shown in Table 8, the difference between both the groups was non-significant (p=0.1817>0.05), whereas the difference between different follow-up periods was significant (p=0.006<0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 39 | 1 | 0 | 38 | 2 | 0 |
| Three months | 37 | 1 | 0 | 36 | 2 | 0 |
| Six months | 36 | 0 | 0 | 36 | 1 | 0 |
3.7. Gingival Bleeding
Table 9 shows that the score was predominantly recorded (A) at different follow-up periods for both the groups with no record for score (B) or (C) at different follow-up periods. The difference between both the groups was non-significant (p= 1>0.05). Similarly, the difference between different follow up periods was also non-significant (p=0.091>0.05).
| Composite | Group A: Bulk Fill Packing | Group B: Incremental Packing | ||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 40 | 0 | 0 | 40 | 0 | 0 |
| Three months | 38 | 0 | 0 | 38 | 0 | 0 |
| Six months | 37 | 0 | 0 | 37 | 0 | 0 |
3.8. Secondary Caries
The score was predominantly recorded (A) at different follow-up periods for both the groups with no record for score (B) and score (C) at different follow-up periods. The difference between both the groups was non-significant (p=0.391>0.05) as presented in Table 10 below, whereas the difference between different follow-up periods was significant (p=0. 005<0.05).
| Composite | Group A: Bulk fill Packing | Group B: Incremental Packing |
||||
|---|---|---|---|---|---|---|
| Time score | A | B | C | A | B | C |
| Baseline | 40 | 0 | 0 | 40 | 0 | 0 |
| One week | 40 | 0 | 0 | 40 | 0 | 0 |
| Three months | 38 | 0 | 0 | 38 | 0 | 0 |
| Six months | 36 | 0 | 0 | 37 | 0 | 0 |
4. DISCUSSION
Despite the fact that a 6-month period is considered to be a short period of time to reflect restoration, clinical performance and failure, it does give an indication for the future performance of the restoration. Results revealed insignificant differences between Tetric EvoCeram (bulk fill) and incremental packing regarding all USPHS criteria. This finding agrees with the findings by Alkurdi and Abboud (2016) [9] who compared the clinical performance of the two resin composite restorations (bulk fill and incremental packing) in class II cavities and showed acceptable clinical results over a 12 months period. Also, Frankenberger et al., (2012) [10] compared the clinical behavior of two different resin composite restorations (bulk fill and incremental packing) and found that both the materials performed satisfactorily over a 6 months observation period. The bulk fill resin composite performed at least equal to the conventionally layered resin composite during the first six months of the clinical trial.In addition, El-Eraky et al., (2014) [11] found no significant difference between the two bulk fill composite resin class II restorations one week after placement as a baseline, and at 6, 12 and 18 months postoperatively using the same criteria. Similar results were also obtained by Celik et al., (2010) [12] when two nanohybrid posterior composites were compared for class I cavities. Moreover, the findings of the study by Shimada et al., (2007) [13] were also the same, who demonstrated that the evaluation of composites during short periods depicted minor changes as compared to the baseline. Similarly, Dijken and Pallesen (2015) [14], also compared the clinical durability of bulk fill resins in class I posterior resin restorations and stated that bulk-fill technique showed acceptable clinical results and was similar to the conventional layering technique during the evaluation period. Good surface characteristics, marginal adaptation, and color stability, as well as the low frequency of secondary caries, were observed. The materials exhibited satisfactory performance throughout the observation periods (1 week, 3 months and 6 months). A possible explanation for this satisfaction in clinical performance is the fact that all restorations were done in conservative class I cavities, which probably contributed to a more effective sealing, reducing marginal leakage. Besides, all the patients were instructed to follow oral hygiene measures, and the restorations were done after a suitable disease control [15]. In this study, the difference between the follow-up periods was insignificant for retention, marginal integrity, surface stain, gingival bleeding, and secondary caries. The percentage for the Alpha score for retention was 95% (n=38) for Tetric EvoCeram (bulk fill packing) and (incremental packing) at 6 months follow up period. It was reported that the insignificant difference in retention could be related to the bonding material or the technique used {Yip et al., (2003) [16] and Dresch et al., (2006)} [17]. The inclusion criteria in this study might also affect the outcome as the conservative class I cavity preparations exhibited a high C factor (5/1) which might explain the limited loss of adaptation at the cavity margins [18]. Class I cavities represent an ideal use of adhesive materials, the margins were all in the enamel. If the margins were extended to involve dentin (class II or V) or cementum (root caries), the results would have been different [19, 20]. On the other hand, results were not consistent with the study by Moura et al., (2011) [21] who compared different composite restorations and reported a high failure of retention of the restorations. This could be related to the difference in the adhesive used. One single adhesive system was used in this study to minimize the variables. It is important to highlight that the ethanol-based adhesive was used in this study as compared to Moura's study who used the acetone-based adhesive system, which demonstrated lower bond strength than ethanol or water-based adhesive systems, exhibiting questionable clinical performance. It is safe to say that the use of deferent adhesive system can have an effect on the end results, therefore, further investigation in this matter is indicated [22, 23]. The marginal seal is an important parameter to be considered in clinical evaluation. The results showed no significant difference between different follow-up periods for marginal seal. At 6 months, only 1 Tetric EvoCeram restoration (bulk fill packing) (2.5%) and 1 Tetric EvoCeram restoration (incremental packing) (2.5%) were rated Charlie score. During the follow-up periods, fractures in restorations were not observed, indicated good marginal adaptation [15]. The marginal adaptation is directly linked to the marginal integrity for any restorative material and is associated with several factors such as contraction of polymerization [19]. Marginal adaptation is directly influenced by the type of composite resin used. On the other hand, Moura et al., (2011) [19] reported inadequate marginal seal when they evaluated the restorations clinically for 3 years which could be attributed to the long evaluation period compared to six months of evaluation in this study. The composite's polymerization shrinkage and the long-term degradation of the adhesive system should also be considered. Also, the results showed an insignificant difference between different follow-up periods for surface stains. 36 Tetric EvoCeram restorations (bulk fill packing) (90%) were rated Alpha score, and 2 restorations (5%) were rated Bravo. For Tetric Evo Ceram (incremental packing), 37 restorations (92.5%) were rated Alpha score, and 1 restoration (2.5%) was rated Bravo. Surface stains may be the first sign of incubating debris that contains cariogenic bacteria with the potential to initiate an active carious wall lesion at the interface.
In most cases, this stain accumulation is associated with a margin defect, creating a gap between the cut tooth and the restorative material [11].
According to Lopes et al.,(2003) [24] the surface stains might be due to the patient’s habits, their oral hygiene, and the extent to which they are influenced by external factors such as drinks, food, cigarettes and other things that possess stain elements. Gingival bleeding was not observed because the simple class I cavities had no proximal contact and contour [25]. All Tetric EvoCeram restorations (bulk fill packing) and (incremental packing) were rated Alpha score at 6 months follow-up period. Development of secondary caries could be due to the material used, clinical environment, caries experience of patients, criteria for replacements and different handling characteristics which affect their clinical behavior [26]. Results of this study revealed the insignificant difference in the follow-up periods for secondary caries and all restorations of Tetric EvoCeram (bulk fill packing) and (incremental packing) were rated Alpha score at baseline, 1 week, 3 months and 6 months. This result was in accordance with the results obtained by Junior et al., (2008) [15] who found no statistically significant difference in secondary caries when they compared composite resin restorations in class I cavities. Prdal and Hegde (2008) also obtained similar results [27] when they compared two composite resin materials in class I and class II cavities, and none of the restorations had any evidence of caries along the margin of the restorations. Thus all were rated Alfa at six months evaluation period. The clinical success obtained by the absence of secondary caries was probably a result of the adequate restorative technique, short evaluation period and good oral hygiene of the patients. It must be reported that all restorations were placed in the university clinic and the patients were selected with good oral hygiene, low caries risk and without severe malocclusion or bruxism.
On the other hand, Celik et al., (2010) [12] demonstrated secondary caries in class I cavities restored with nanohybrid composites although they evaluated the restorations at short periods and they claimed that secondary caries was 3.5 times higher in composite restorations than an amalgam restoration. The results showed a significant difference between different follow-up periods for color match, surface texture, and post-operative sensitivity. This could be attributed to the problems associated with the use of composite resin restorations. According to Lopes et al., (2002) [28] the use of composite resins for the restoration of posterior teeth presented other problems such as microleakage, postoperative sensitivity, and technical difficulties. Regarding the color match, 31 Tetric EvoCeram (bulk fill packing) restorations (77.5%) were rated Alpha score, 2 restorations (5%) were rated Bravo score and 5 restorations (21.5%) were rated Charlie score and for Tetric EvoCeram (incremental packing) 32 restorations (80%) were rated Alpha, 2 restorations (5%) were rated Bravo and 4 restorations (10%) were rated Charlie at 6 months follow up periods. The color match was thought to be involved with the organic matrix of resin composites and the alterations in surface texture could be attributed to many variables related to the inorganic filler of resin composites like size, hardness and amount of inorganic loading [15]. As for surface texture, 33 Tetric EvoCeram (bulk fill packing) restorations (82.5%) were rated Alpha, 3 restorations (7.5%) were rated Bravo and 2 restorations (5%) were rated Charlie and for Tetric EvoCeram (incremental packing) 34 restorations (85%) were rated Alpha, 2 restorations (5%) were rated Bravo, and 2 restorations (5%) were rated Charlie at 6 months follow up periods. It was reported that nanohybrid composite recorded higher surface roughness after finishing and polishing. This might be due to exfoliation of the large glass filler particles from the matrix during the polishing procedures [11]. Another finding stated that the rate alpha was given to a surface as enamel, knowing that no material replaces all the qualities of the enamel and this especially applies for its smooth, polished surface [29].
Moreover, the changes in surface texture and color stability of resin composite restorations could increase after one year [30]. To put this issue in better perspective, it is essential to remember that all restorations were acceptable in terms of color match, and especially when compared with an amalgam restoration [27]. Postoperative sensitivity seemed to be a problem related to resin composite restorations. The results showed a significant difference in different follow-up periods for Tetric EvoCeram (bulk fill packing): 37 restorations (92.5%) were rated Alpha, and 1 restoration (2.5%) was rated Bravo. For Tetric EvoCeram (incremental packing) 34 restorations (85%) were rated Alpha, and 4 restorations (10%) were rated Bravo score. Many studies have indicated that up to 30% of the studied populations had reported post-operative sensitivity following the placement of a posterior resin restoration [12]. The increase in dentin permeability provoked by acid-etching technique could be one of the explanations for this post-operative sensitivity. Unfortunately, it is not possible to prevent trauma from operative and restorative procedures completely.
Furthermore, sensitivity is influenced by the patient, the dentist, the choice of the material and the type of the tooth [31]. On the other hand, these results were not consistent with the findings obtained by Chermont et al., (2010) [32] who evaluated the postoperative sensitivity clinically in class I cavities and stated that dentin adhesive did not result in any significant difference in postoperative sensitivity and the clinical technique might be more relevant to the development of sensitivity rather than the type of adhesive itself. This difference could be related to the adhesive systems as they used adhesives containing glutaraldehyde or it could be related to the difference in the evaluation period as they evaluated the restorations at 48 hours and after 7 days as compared to this study which evaluated the restorations at 1 week, 3 months and 6 months.
CONCLUSION
Clinical results varied with the placement technique of the resin composite restoration and incremental packing showed better results when compared to bulk fill packing.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Imam Abdulrahman Bin Faisal University (IRB-2019- 234-Dent).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All the research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013. (http://ethics.iit. edu/ecodes/node/3931)
CONSENT FOR PUBLICATION
The patients signed an informed consent form before participating in the research.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Hospital of Dentistry, College of Dentistry at https://www.iau.edu.sa/en/colleges/college-of-dentistry, reference number (IRB-2019- 234-Dent).
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

