All published articles of this journal are available on ScienceDirect.

Effect of Contamination, Damage and Barriers on the Light Output of Light-Curing Units
Abstract
Background:
Light-curing is a crucial step during the application of composite resin restorations. The clinical success of composite depends on the Light-Curing Units (LCU) to deliver adequate light energy to polymerize the resin. However, light-curing usually does not receive the proper awareness it deserves.
Objective:
This study aims to evaluate the effect of contamination and debris of the LCU’s tip on its light output. Determine the effect of damage to the LCU’s tip such as chipping, dents and scratches. Additionally, it evaluates the effect of plastic barrier sleeves.
Methods:
Sixty LED LCUs were tested using MARC™ Resin Calibrator (BlueLight Analytic Inc., Halifax, Canada) to measure their irradiance and energy before and after cleaning their tips. They were also tested with and without a clear plastic barrier. Additionally, four damaged LCUs received new tips and were tested again. Kruskal-Wallis H and One-Way ANOVA tests were used for statistical analysis.
Results:
Cleaning the LCUs’ tips showed significant improvement, an average increase of 8.2%. However, some units increased by up to 47% in irradiance and energy values. Replacing the damaged tip with a new one significantly improved the output of the LCUs, increasing light energy by up to 73%. The barrier used in this study caused 7% reduction in the energy delivered by the LCUs. The statistical analysis showed that cleaning the LCUs and replacing their damaged tips resulted in a significant increase in energy (p<0.05).
Conclusion:
Unclean or damaged LCUs’ tips can drastically reduce the light output of the LCUs, reducing the quality of the composite restorations. Clinicians are strongly recommended to regularly monitor, clean and maintain their curing lights.
1. INTRODUCTION
Light-curing is an important step in the restorative dentistry during the application of light-cured Resin-Based Composites (RBC), and the clinical success of those restorations depends on the light-curing units to deliver adequate light energy to polymerize the resin. However, light-curing usually does not receive the proper awareness it deserves and is often taken for granted, which can lead to incomplete polymerization and higher failure rate of RBCs [1-5]. With the increased demand and use of RBCs, light-activated cements and adhesives, as well as the extensive use of light-curing units (LCU) in other dental procedures like orthodontics and bleaching. LCUs have become an essential and heavily used equipment in daily dental practice [6, 7]. Therefore, some issues like damage, contamination and debris on the LCU’s light guide tip raise the question on the significance of the effect of those issues and to what degree they can decrease the LCU’s efficiency to deliver the required energy to adequately cure the RBCs [8-11].
Although several articles have suggested maintaining the LCUs and keeping them clean and free of contaminants [2, 8, 11], it has been shown that the majority of LCUs in dental practices are affected by the adherence of composites and bonding material on its tip [12-14], which can lead to the reduction of the light output [9]. Furthermore, it was stated that infection control methods like the use of protective plastic barriers to cover the LCU can reduce its light output. The light exposure time needs to be increased to compensate for this reduction [11, 14,15]. Therefore, this point of interest needs to be confirmed, because the barrier sleeve is mandatory for infection control, specially that autoclaving the light guide tip is generally not used as an infection control method because it has been shown to decrease the light irradiance significantly over time [15, 16]. The barrier should be snugly fit the light cure and it should not impede the light cure output [17]. Many studies have found that some infection control methods might reduce light intensity of LCU by up to 40%. A clear thin barrier is considered the best option as it causes light energy reduction less than the other options [9, 14, 18-21].
Moreover, a damage to the LCU might occur through use such as scratches, dents or chipping of its tip. Although it is logical to get a damaged dental equipment replaced, some dental practices might ignore the issue and continue to use the damaged LCU [4, 8, 14]. Also, it has been shown that the LCU’s power can decrease with long-term or extensive use, and that dentists are often using LCUs that deliver inadequate light energy [22, 23]. However, usually it is because they were unaware that their LCUs were not able to adequately cure their restorations [24]. All these factors will affect the efficiency of the LCU units to properly cure composite resin.
Clinicians must understand the principles of light-curing because improper curing of composites can dramatically affect its physical and chemical properties leading to complications such as reduced hardness, reduced bond strength to tooth structure, microleakage, post-operative sensitivity, recurrent caries, color instability, increased wear and fracture, and making the composite less biocompatible because unbound monomers are cytotoxic [25, 26].
Knowledge of the LCU’s irradiance and the energy requirement of RBCs is essential for successful polymerization. However, it has been shown that a majority of dentists are not familiar with this information which might lead to under-polymerized restorations [3, 4]. Clinicians need to understand radiometric terms such as the term radiant flux or power, which is used to describe the power output of the LCU and expressed in units of Watt (mW). The irradiance (usually used by the manufacturers and called light intensity) is the radiant power delivered by the LCU to a surface and expressed in units of Watt/area (mW/cm2). The radiant energy, which is irradiance over time expressed in units of Joule/Area (J/cm2) [1, 26-28]. It is important to know the required amount of energy to properly cure composite resins. This value can vary depending on the composite. Clinicians should always check the manufacturer’s instructions [25, 29]. However, it has been shown that an energy dose of 16-24 J/cm2 is needed to properly cure a 2 mm thickness layer of composite [30-33]. Also, studies showed that an LCU with light irradiance of at least 300-400 mW/cm2 is required to appropriately cure a composite increment of 1-2 mm thickness. Therefore, it is not recommended to use LCUs with irradiance less than 400mW/cm2 [25]. And in such case this LCU should be used for 40 seconds on each composite layer to achieve the required energy (16 J/cm2).
Studies have shown that most dentists do not know the power of the LCUs they use, or the amount of energy different resin-based composites need to receive for sufficient curing and adequate polymerization. Using a dental radiometer, dentists can measure their LCU’s irradiance, but these devices was shown to be inaccurate. Therefore, clinicians might have difficulty knowing the irradiance and radiant energy that they are delivering to their restorations [6, 34]. In a recent study in Germany, it was found that only 41% of LCUs used in dental offices had intact undamaged light tips [35]. Also, most dentists are lacking attention to cleaning and maintaining their LCUs regularly [8, 35-37]. All of this can lead to RBCs that are not properly polymerized which in turn can increase the failure rate of these RBCs [1-5].
The aim of this study is to evaluate the effects of contamination and debris of the LCU’s tip on its light output, to evaluates the effect of damage to the LCU’s tip and to evaluate the effect of barrier sleeves. The first hypothesis was that cleaning the tips of the LCUs will increase their light energy delivered to composite restorations. The second hypothesis was that the use of barriers as infection control method can reduce the energy delivered by the LCUs. The third hypothesis was that damaged tips reduce light energy and replacing them with new tips will increase the LCU’s light output. This study will show the significance of care and maintenance of the LCUs to raise awareness among dental care professionals for optimal use of light-curing units.
2. MATERIALS AND METHODS
This study used the MARC™ Resin Calibrator (RC) (BlueLight Analytics Inc., Halifax, Nova Scotia, Canada), which utilizes a laboratory grade spectrometer (Model USB4000, Ocean Optics Inc, Dunedin, FL, USA) to accurately record the irradiance and energy delivered to the sensors that is 3.9 mm in diameter and resembled the top surface of composite. The sensor is connected to the spectrometer with a bifurcated fibre optic cable. This device was used to measure the irradiance of the LCUs and the total energy that they can deliver to the top surface of the composite at zero distance. A pre-configured laptop computer with a custom software (MARC™ Light Collector) that incorporates data collecting, storing and exporting. The data reported includes measurements like the actual optical curing time, the mean and max irradiance, the mean and max power, the calculated energy and the wavelength spectrum of the LCU. The MARC™-RC is fixed on bench MARC™, a special bench consists of specially designed modifiable accessory arms that allows the LCU to be fixed accurately into the desired position over the sensors and moved using the knobs that can move the LCU precisely in horizontal and vertical directions. This enables accurate adjustment of the LCUs over the sensors, so it can be assured that LCUs are positioned the same every time an LCU is tested. One LCU (Demi™ Ultra, Kerr, USA) was used for the calibration of the device prior to the study, it was also used between tests to assure that the device is giving accurate measurements. This was done by one examiner only and an intra-examiner agreement test was done, and the results were consistent. The mean irradiance of the calibration LCU was 1600 ± 4 mW/cm2. All the LCUs were fully charged before testing, to ensure that they are working on their full power.
Sixty LED LCUs were collected from the clinics in the College of Dentistry at Ajman University. Each LCU was assigned a number, then the details of the LCUs were marked down including the assigned number, its model, serial number, date of manufacturing and which clinic/lab it belongs to, so they can be retrieved whenever they are needed. (Table 1) shows the details about all the types of LCUs used in the study.
After MARC™-RC was calibrated, the LCUs were tested. Each LCU was fixed on the resin calibrator with its tip perpendicular to the sensor surface at a zero-millimeter distance. All information was inserted in the software, which includes the brand name, model name, curing mode, curing time, the tip diameter which was pre-measured using a caliper and the distance between the tip and the sensors. Other parameters had to be checked that include the integration time which was fixed at 60 ms for all LCUs and the sensor trigger at 50mW as recommended by BlueLight Analytics. Also, the energy required which was also fixed for all units at 16 j/cm2 which was already set by the software and as recommended by Phillip’s text book [30]. The parameters on the software were confirmed and the test was started by pressing the curing button on the LCU which automatically starts the recording on the software, and it shows live data on the screen including a graph. It automatically stops recording when the LCU stops curing. The curing time was set to 20 seconds for all LCUs except Acteon mini LED and 3M Ortholux Luminous as shown in (Table 1). The curing mode used was the standard curing mode for all the LCUs.
Each LCU was tested in 4 conditions. Initially, the LCU was tested as it is without cleaning and without a barrier (Group 1). Then, the LCU was tested as it is but with a plastic sleeve barrier (Dochem plastic syringe sleeves model number 1A6511, England United Kingdom) that is utilised as an infection control method to protect the LCU from contaminations while using it in patient’s mouth. The barrier was snuggly fit to the LCU and the tip of the LCU was not facing the seam of the barrier (Group 2). All light guides were cleaned following the manufacturer’s recommendations and based on the literature [8, 11], making sure the tip is as clear as possible of all debris and contaminants. It was done using a soft cloth and 40% Isopropyl alcohol solution (Green Cross, Philippines). It was recommended by the manufacturers to remove the light guide from the unit and clean it separately which made it possible to clean the inside of the light guide that goes inside the LCU, then the light guide was dried with a second soft cloth and was checked again to ensure that it is clear from any debris, then it was tested without using a barrier (Group 3). Finally, the cleaned LCU was tested with the barrier (Group 4).
From the sixty LCUs, a total of 240 reports were collected and saved. However, for two LCUs (Ortholux Luminous and Seker L-460) the data was excluded because of very small sample size (one for each of them) as shown in (Table 1). Data was then exported for statistical analysis. The 232 reports were divided into four groups (58 each). Group 1; as received, Group 2; as received with barrier, Group 3; cleaned, Group 4; cleaned with barrier. Data distribution was found non-normal using Shapiro-Wilk normality test. Thus, data were analyzed using Kruskal-Wallis H nonparametric test. Furthermore, for a more controlled testing and to exclude all other features of the LCUs that may interfere with the effect of contamination, the data for 30 Acteon Mini LED (all of them having same power, features and age) were separated and analyzed using One-Way ANOVA.
Additionally, some of the LCUs were noted for having a damaged light guide tip, ranging from small scratches to dents to a broken tip. Therefore, their reports were isolated. Then their damaged tips were replaced with new tips and they were tested again. Four LCUs shown in (Table 4) were tested for damage effect using MARC™-RC. A total of 8 reports were collected and exported separately for statistical analysis and were divided into 2 groups damaged tips (n=4) and new tips (n=4).
All analyses were conducted at a 5% significance level using (SPSS Inc., version 20.0; Chicago, IL, USA).
| LCU Model | N |
Power (as claimed by the manufacturer) |
Curing Time | Energy (calculated in the curing timed used) | Tip Ø* | Wavelength Spectrum** |
|---|---|---|---|---|---|---|
| Mini LED (Acteon, France) | 31 | 1250 mW/cm2 | 10s | 12.5 J/cm2 | 7.5mm | 410-490 (448) |
| Litex 696 (Dentamerica, USA) | 12 | 1200 mW/cm2 | 20s | 24 J/cm2 | 8.5mm | 420-510 (458) |
| LED B (Woodpecker, China) | 11 | 1000 mW/cm2 | 20s | 20 J/cm2 | 8mm | 424-510 (459) |
| BluePhase N (Ivoclar, Germany) | 4 | 1200 mW/cm2 | 20s | 24 J/cm2 | 9mm | 390-510 (455) |
| Ortholux Luminous (3M, USA) | 1 | 1600 mW/cm2 | 15s | 24 J/cm2 | 8mm | 420-509 (456) |
| L-460 (Seker, China) | 1 | 1200 mW/cm2 | 20s | 24 J/cm2 | 7.5mm | 425-510 (458) |
3. RESULTS
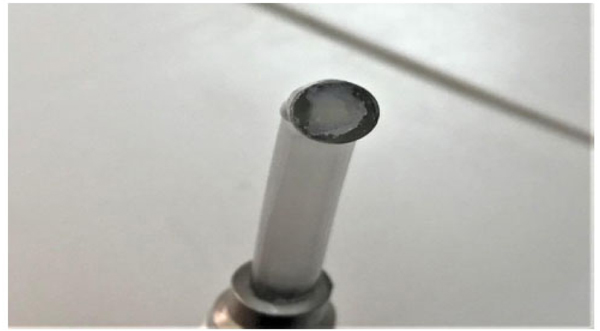
Group 1 showed an average energy of 16.99 J/cm2. Group 2 had the lowest energy values with an average of 15.78 J/cm2. Group 3 achieved the highest energy values an average of 18.53 J/cm2. Group 4 showed an average of 17.18 J/cm2. (Table 2) shows the mean energy, standard deviation, minimum and maximum energy for each group. The statistical analysis using Kruskal-Wallis H test showed that cleaning the tip of the LCU resulted in a significant effect (P<0.05), increasing the amount of energy delivered by all the LCUs. There was an average of 8.2% improvement in energy when comparing group 1 to group 3 and when comparing group 2 to group 4. Fig. (1) shows a contaminated LCU’s tip, a layer of composite residue covers most of the tip, reducing the amount of light energy delivered by the LCU to the restoration. The analysis also showed that using a barrier can cause a slightly significant reduction the energy values (P<0.05). There was an average of 1.27 J/cm2 (7.28%) reduction in energy when comparing the barrier groups (2 and 4) to the no barrier groups (1 and 3).
Furthermore, the analysis of the smaller group of 30 Mini LED curing lights further confirmed the results. Showing an average of 7.5% improvement in energy values after cleaning the LCUs. One-Way ANOVA also showed that there was a significant difference between the two groups (P<0.05). (Table 3) shows the mean energy, standard deviation, minimum and maximum energy for the two groups.
| Factor | n | Mean ± SD Energy (J/cm2) | Range (J/cm2) |
|---|---|---|---|
| Group 1 (As received) | 58 | 16.99 ± 4.60 | 3.98 - 28.77 |
| Group 2 (As received with barrier) | 58 | 15.78 ±4.28 | 3.77 - 26.29 |
| Group 3 (Cleaned) | 58 | 18.53 ± 4.98 | 4.15 - 33.65 |
| Group 4 (Cleaned with barrier) | 58 | 17.18 ± 4.66 | 4.03 - 31.68 |
| Factor | n | Mean ± SD Energy (J/cm2) | Range (J/cm2) |
|---|---|---|---|
| Acteon Mini LED (As received) | 30 | 16.87 ± 0.885 | 15.24 - 18.87 |
| Acteon Mini LED (Cleaned) | 30 | 18.24 ± 0.667 | 17.19 – 19.88 |
| LCU | Condition | Actual Curing Time | Mean Irradiance (mW/cm2) | Total Energy (J/cm2) | Irradiance Difference (mW/cm2) | Energy Difference (J/cm2) | Difference % |
|---|---|---|---|---|---|---|---|
| Mini LED | Damaged | 9.96s | 1025 | 10.21 | 753 | 7.61 | 73.4 |
| New | 10.02s | 1778 | 17.82 | ||||
| LED.B #1 | Damaged | 20.15s | 962 | 19.38 | 91 | 1.9 | 9.4 |
| New | 20.21s | 1053 | 21.28 | ||||
| LED.B #2 | Damaged | 24.59s | 455 | 11.18 | 140 | 3.5 | 30.7 |
| New | 24.66s | 595 | 14.68 | ||||
| Bluephase N | Damaged | 20.09s | 1054 | 21.17 | 408 | 8.2 | 38.7 |
| New | 20.09s | 1462 | 29.37 |
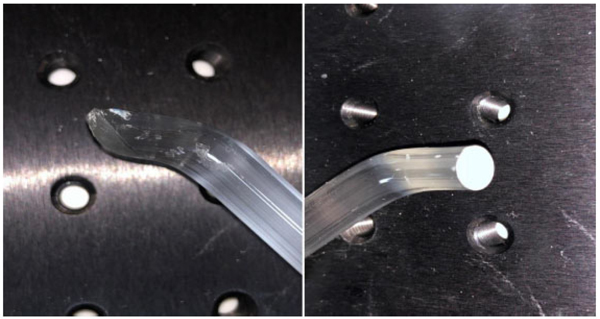
(Table 4) shows the effect of changing the damaged tip to a new one on the irradiance and energy delivered by the LCUs. The four damaged LCUs improved by 9.46%, 30.77%, 38.71% and 73.46% after changing their tips. The analysis showed that changing the damaged tip with a new one had a significant effect (P<0.05). Fig. (2) shows the damaged tip and the new tip that was used to replace it for Acteon mini LED. This caused a 73.46% improvement in the irradiance and light energy delivered.
Additionally, the LCUs were divided into groups according the type (model) and compared. However, two models were excluded (3M Ortholux Luminous and Seker L-469) because sample size was only one for each. Also, one Acteon mini LED was excluded because it was a much older version of the LCU compared to the other 30 units. This comparison used the irradiance not the energy because each LCU had a different curing time. It was found that there was a significant difference between all the groups (p<0.05) except when comparing the Woodpecker LED B to Dentamerica Litex 696 there was no significance difference in irradiance (p=0.786). Only 2 LCUs (Woodpecker LED B) did not reach the minimum recommended irradiance of 400 mW/cm2. (Table 5) shows the mean irradiance, standard deviation, minimum and maximum irradiance for each type of LCUs.
| LCU | N | Mean ± SD Irradiance (mW/cm2) | Range (mW/cm2) |
|---|---|---|---|
| Acteon Mini LED | 30 | 1819.9 ± 65.5 | 1707 – 1986 |
| Woodpecker LED B | 11 | 897.8 ± 406.3 | 183 - 1549 |
| Dentamerica Litex696 | 12 | 819.5 ± 114.3 | 609 - 985 |
| Ivoclar BluePhase N | 4 | 1528.2 ± 262.2 | 1462 – 1674 |
4. DISCUSSION
This study found that contamination and damage of curing light tips reduce their irradiance and energy delivered to composite restorations which might lead to under polymerized resin and increased failure rate of those restoration.
When the LCUs were collected, it was noticed that most of the units had debris and contamination present on the light guide tips ranging from a layer of adhesive to big chunks of composites. It was clear from the reports that cleaning the tips of the LCUs had significant effect on the light output and amount of energy delivered by these LCUs. However, since the increase in energy was dependent on the amount of tip contamination and debris that was removed, which was not consistent as some LCUs were well maintained and had almost no contaminants on the tip and other LCUs were poorly maintained and had large amount of residue adhered to the tip. The improvement in energy ranged from 0.58% to 47.43%. Even though the LCUs should not get contaminated in the first place (by covering them with a barrier). However, in case the tip was contaminated, the LCU must not be used in that condition, specially that cleaning and disinfecting the LCU does not require any special or complicated equipment and takes few minutes only but it can make dramatic effect by increasing the energy delivered by the LCU. Thus, reducing the chance of under-curing composite restorations and increasing their success rate. Other studies have also showed that cleaning and disinfecting LCUs is highly recommended to maintain its light output power. However only approved cleaning solutions should be used, as some sterilization fluid can damage the LCU’s tip or the lens that is covering the LED [2, 8, 10, 26].
The plastic barrier decreased the energy delivered by the LCUs by 7.2%. While it might not by a huge reduction, it should be always considered that curing time might need to be increased to compensate this reduction. Only one type of barriers was tested in this study. However, because different types of barriers exist and because different manufacturers might make barriers with different materials, thickness and texture, the effect of these barriers will certainly vary. Therefore, additional investigations are needed. Nonetheless, barriers are still the best option and it is recommended by other studies over other infection control methods for the LCUs [2, 8, 11, 15, 26].
After replacing the damaged tip with a new one the energy increased for all 4 LCUs. However, the energy improvement ranged from 9.46% to 73.46%. Meaning that the type and extent of tip damage will determine how much it can affect the LCU’s light output, but no doubt a damaged tip can cause a significant drop in energy delivered by the LCU, because light will be scattered instead of being directed directly to the restoration. Therefore, dentists must not use LCUs with damaged tip and should replace it with a new tip if possible. A study performed in 2011 has showed how damage to the LCU’s tip can significantly reduce its light output [14].
It was noted that the Woodpecker LED B budget LCUs had some issues. For example, different LCUs of this model delivered irradiance values that ranged from 183 mW/cm2 to 1549 mW/cm2, which means they are not consistent and cannot always be trusted to deliver the light output claimed by the manufacturer. Also, it was found that two LCUs of the same model failed to even deliver the minimum required irradiance of 400 mW/cm2 (363 mW/cm2 and 183 mW/cm2) even after cleaning their tips. Many studies have showed that the light energy delivered by many dental practice curing lights are inadequate and are not capable of properly polymerizing the resin in the selected time [24, 26]. Therefore, it is always advised to keep the curing light monitored using radiometers and keeping a record to show that the light output was checked. Even though some radiometers might not give accurate irradiance numbers or may not show a number at all (using light to indicate the LCU’s power), they can be used to determine whether light output has changed over time [2, 8, 11, 26]. If the output was reduced it will be necessary to increase the exposure time. If the irradiance was reduced to less than the minimum 400 mW/cm2, it is then recommended to get the LCU either fixed or replaced to a new one to ensure that the composite resin restorations are being adequately polymerized.
CONCLUSION
Contaminants and debris on the LCU’s tip can significantly reduce its light output. Cleaning the tip with proper disinfection methods will improve the energy delivered by the LCU to the composite restoration. The amount of debris present on the tip before cleaning will determine to what extent the LCU’s output will improve. Damage to the LCU’s tip can cause significant reduction in the energy delivered by the LCU to the restoration. LCUs with broken tips should never be used as the light might not be delivered adequately to the restoration. The use of barriers reduces the light output of the LCU as it scatters the light and this reduction should always be taken into consideration by adjusting the curing time to compensate this reduction. Budget LCUs’ power might be much less than the power claimed by the manufacturer and it might even fluctuate for the same model. This must be considered by the dentist when using such LCUs.
Clinicians are strongly recommended to monitor their LCUs periodically by testing their irradiance and energy and keeping a log book for the records. Also, it is highly recommended that clinicians must maintain their LCUs regularly by disinfecting the tip and keeping it clean and by replacing the damaged tips to ensure adequate polymerization of their RBCs. They should adjust the curing time to compensate any reduction in the LCU’s irradiance. Also, they should fix or discard any LCUs that do not reach the minimum recommended irradiance.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIAL
The data sets analyzed during the current study are available from the corresponding author on request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank Mrs. Hanine Bou Antoun for her valuable input in statistics.

