All published articles of this journal are available on ScienceDirect.

Retained Primary Molars and Related Reasons in Umm Al-Qura University, Makkah: A Retrospective Study
Abstract
Background:
Retention of primary molars beyond the expected time of exfoliation is uncommon; this condition is known as persistence. A retained primary tooth, with the crown in good condition, roots, and supporting alveolar bone can serve adults for many years.
Objective:
To determine the prevalence of retained primary molars and investigate the reasons for their persistence in Umm Al-Qura University.
Methods:
Overall, 500 extra-oral panoramic radiographs were assessed to investigate whether primary molars persisted beyond the expected exfoliation period. Dental records were also reviewed to investigate the possible reasons for persistence. The collected data were tabulated and statistically analyzed, with P < .05 considered significant.
Results:
Seventy-six retained primary molars were identified (39 in females and 37 in males) in 500 panoramic radiographs (from 260 females and 240 males). Agenesis of the permanent successor tooth was the most frequently encountered reason for the retention of primary molars (19%). The second most frequent reason was ectopic deviation of the path of eruption of the successor (11%). The third most common reason was impaction of the successor (10%).
Conclusion:
The incidence of retained primary molars in the investigated population was 15.2%. The most common reason for the persistence of primary molars was agenesis of the permanent successor, followed by ectopic eruption and impaction of the successor teeth. These data highlight the need for education and awareness of dentists and patients to preserve the primary tooth when there is no permanent successor present and support an appropriate treatment plan for each case.
1. INTRODUCTION
The retention of primary molars beyond their expected time of exfoliation is an uncommon condition, known as persistence or retention. Only a limited number of reports have investigated the persistence of primary teeth [1-3]. When the crown, roots, and alveolar bone are sound, such a retained tooth can serve an individual for many years through adolescence and adulthood [4]. However, retained primary teeth can also lead to clinical problems [5], including periodontal bone loss of the neighboring permanent teeth [6], dental caries, and loss of proper arch integrity when mesial tipping or distal drifting occurs. This complicates the condition of the retained primary tooth, which assumes an infra-occlusal position [7] owing to the continued eruption and movement of adjacent teeth [4]. Retention of primary teeth can result in several complications, which require orthodontic treatment or surgical intervention. Ankylosis of the primary molars leave the primary teeth submerged or in a significantly infra-occlusion position. With such loss of arch integrity, tipping of the adjacent permanent teeth usually occurs and complicates proper alignment of the dentition. Furthermore, super-eruption of the opposing teeth often arises as a significant consequence of neglected or improperly managed conditions. Ankylosis of the primary teeth could occur in addition to ectopic eruption or after impaction of permanent premolars. This leads to a localized or generalized loss of the required arch length and would eventually result in malocclusion and crowding of the dentition [8].
Few studies have investigated factors underlying the retention of primary teeth. The most common reason was the developmental absence of a permanent successor tooth or congenitally missing permanent premolars [9]. Mandibular second premolars appear to be the most frequent congenitally missing successors [10]. Teeth agenesis is more common in females, with a female: male ratio of 1.37:1 [9]. The etiology of tooth agenesis is mostly idiopathic; however, there may also be a familial cause, with an autosomal dominant pattern of inheritance. Tooth agenesis is a dental malformation that is one of the most common congenital malformations in humans [11]. Agenesis of permanent premolars developing tooth germ is a condition found to be the most common cause for primary molars retention [12]. Certain syndromes, such as ectodermal dysplasia, are associated with a large number of missing teeth [9]. Tooth agenesis could also arise due to environmental factors, such as trauma, infection, or irradiation [10]. Children with agenesis of multiple permanent successor tooth germs are expected to develop persistence of primary teeth more frequently than those without agenesis of the permanent premolars [13].
However, even when the permanent tooth is present, it may fail to erupt, leading to retention of the primary tooth. Furthermore, dental crowding, ankylosis of the primary tooth, lack of eruptive force of the developing successor, ectopic eruption of the permanent successor, deviation in the eruptive path of the permanent successor, or the presence of supernumeraries or other obstructions could also lead to retention of the primary teeth [10]. It has been also reported that the intra-bony migration and impaction of the successor tooth germ could promote persistence of the primary predecessor [14].
A cross-sectional study found that the most commonly retained predecessor was the mandibular second primary molar, followed by the maxillary deciduous canine [10]. In a study conducted by Aktan et al. in 2011, primary teeth were more frequently retained in the mandible than in the maxilla, and the right side was less affected than the left side [4]. However, previous studies have not clearly explained the reasons for the retention of primary teeth.
Little is known about the prevalence of retained primary molars in Saudi Arabia, or about their association with periodontal problems, dental caries, formation of pathological cyst or tumors, and concomitant ankylosis of the offending tooth. Accordingly, the aim of the present study was to determine the prevalence of retained primary molars and investigate the reasons underlying their persistence among individuals attending Umm Al-Qura University Dental Teaching hospital, Makkah, Saudi Arabia.
2. MATERIALS AND METHODS
2.1. Study Design and Subjects
A total of 500 panoramic radiographic images were obtained from the files of patients attending the Dental Teaching Hospital, Faculty of Dentistry, Umm Al-Qura University. All high-quality radiographic images were evaluated individually by a single 6th-year dental student. The subjects' age and sex were also recorded for further comparison.
2.2. Sample Selection
The following inclusion criteria were used: Patients older than 6 years and younger than 25 years; with no history of previous intervention, and no previous tooth extraction.
Extra-oral panoramic radiographs of the included patients were examined. A primary tooth was considered to be persistent if the last permanent successor tooth had erupted more than 1 year previously, and if the primary tooth had not been exfoliated [4].
In the radiographic examination, the reasons for the persistence of the primary teeth as well as the characteristics of the retained primary teeth were evaluated. These factors included the tooth type, number, location, crown-root morphology, such as invaginations, short and slender root forms, root resorption level, apical status, and periodontal support. In addition, we determined whether the teeth showed evidence of having pathological conditions, such as periodontal problems, ankylosis, infra-occlusion, cystic lesion, and tipping of the adjacent permanent teeth.
Tooth agenesis was determined from panoramic radiographs by screening for the absence of permanent tooth germ. Ankylosis of a primary molar was determined when complete cohesion was noticed between the roots and the invested bony structure. An ectopic path of eruption of the permanent successor was observed on the panoramic radiograph when the long axis of the erupting tooth formed an angle other than 90° with its overlying predecessor. According to Shalish and colleagues [15], the presence of infra-occlusion of a deciduous molar can be detected when vertical discrepancy exceeding 3 mm, as measured from the mesial marginal ridge of the permanent first molar, was evident on pretreatment panoramic radiographs. Using these definitions, the proportions (in percentage) of cases demonstrating these features were determined.
2.3. Statistical Analysis
All the collected data were recorded, tabulated, and statistically analyzed using Statistical Package for the Social Sciences (Version 15, SPSS, Inc., Chicago, IL, USA). P <.05 was considered statistically significant. The Chi-square test was used to compare the frequency of retained primary molars among the sexes.
3. RESULTS
The sample included 500 extra-oral panoramic radiographs of regular dental patients, 260 females and 240 males, with an age range older than 6 but younger than 25 years (mean age: 21.25 years). Seventy-six cases showed retained primary second molars (15.2%). Retained mandibular second primary molars (15%) were significantly predominant, as compared to the maxillary arch (0.2%). Only 0.6% of cases showed bilateral retained primary molars, while, in the remaining cases, a single primary molar persisted. There was no significant difference between the sexes (Table 1).
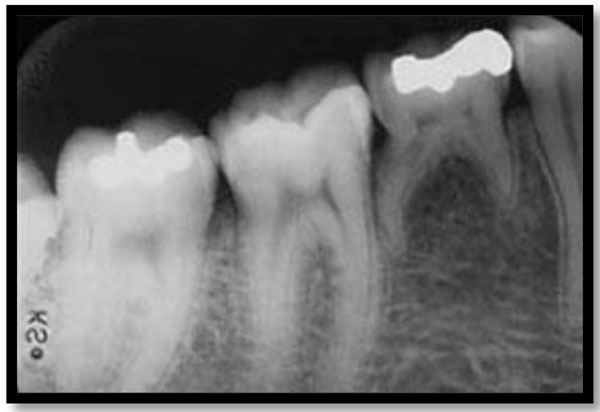
There was also no statistically significant difference between the causes of primary molar persistence (P = 0.29). The reasons for the persistence of primary molars are shown in Table 2. Agenesis of the permanent successor was the most frequently encountered reason for retained primary molars (3.8%) representing 19 cases in the total sample. An example is shown in Figs. (1 & 2). This was followed by ectopic eruption of the developing permanent tooth, at 2.2%, accounting for 11 cases in the total sample (Fig. 3). Another 10 cases (2%) had an impaction of the permanent tooth, and 9 cases (1.8%) demonstrated ankylosis of the primary molar.
| Groups | Retained Primary Molars | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Male | 37 (7%) | 203 (41%) | 240 (48%) |
| Female | 39 (8%) | 221 (44%) | 260 (52%) |
| Total | 76 (15%) | 424 (85%) | 500 (100%) |
| χ2 = 2.48, P = 0.9 | |||
| Groups | Prevalence Rate | F | P | Sig. | |
|---|---|---|---|---|---|
| Agenesis | 19% | 1.26 | 0.29 | NS | |
| Ectopic eruption | 11% | ||||
| Impaction | 10% | ||||
| Ankylosis | 9% | ||||


There was also no statistically significant difference in terms of the most common complications associated with retention of primary molar teeth (P = 0.38). The most common problems associated with retained primary teeth were tipping of the adjacent permanent teeth (2.6%; n = 13), followed by resorption of the primary molar (2%; n = 10), carious primary molars and existence of pathology (1.4%; n = 7), and finally filling in the primary molar (0.6%; n = 3) as illustrated in Table 3.
4. DISCUSSION
The present study, based on retrospective radiograph analysis of a patient population from Makkah, explored the persistence of primary molars with a view to understanding the prevalence and possible causes of their retention, and further investigated the problems associated with their retention, as little is known about the retention of primary molars and the underlying reasons for the retention of primary molars [4].
We included subjects aged > 6 years to explore the incidence of agenesis of the permanent successors, which is classified from the age of 10 years. Participants selected also had to be younger than 25 years to exclude dental complications associated with age advancement such as periodontal disease and the development of dental caries.
In this study, agenesis of the permanent second premolars was found to be the most common reason for the retention of the primary molar, followed by ectopic eruption of the permanent successor and impaction of the permanent successor. Our findings agreed with the results of Aktan and colleagues [4], who stated that retention of the primary mandibular second molars is most often due to agenesis of the permanent mandibular second premolars, which are their successors, followed by ectopic eruption of the permanent mandibular second premolars, and impaction of the permanent mandibular second premolars.
When the level of occlusion of the retained primary molars is located apically and the inter-occlusal space is increased, “infra-occlusion” is said to have occurred. Infra-occlusion is mainly due to ankylosis of the primary molars. In this study, 13 subjects with the tipping of the permanent adjacent tooth and 9 subjects with ankylosed primary molars had a retained tooth in an infra-occlusion position or a submerged primary molar. Submerged primary molars represent a serious negative effect in terms of arch length integrity, which is particularly manifested in terms of tipping of the neighboring teeth and encroachment of the space overlying the tooth in an infra-occlusion position.
| Groups | Prevalence Rate | F | P | Sig. | |||
|---|---|---|---|---|---|---|---|
| Tipping of the adjacent permanent teeth | 13% | 1.15 | 0.38 | NS | |||
| Resorption of the primary molar | 10% | ||||||
| Carious primary molar | 7% | ||||||
| Existence of pathology | 7% | ||||||
| Filling in the primary molar | 3% | ||||||
When no root resorption occurs, and the primary tooth’s coronal structure is good and at the same occlusal level as the adjacent permanent teeth, the tooth is esthetically and functionally acceptable and there is no reason for extraction of the primary molars. It is not possible to predict the probability of survival of a primary molar at an early age; however, the overall probability of primary molar retention can be estimated to be more than 90% [5]. Where no root resorption has occurred and the coronal structure appears to be good, but the primary molar is located inferiorly to the adjacent permanent teeth, the primary molars may be retained and reshaped with direct composite or indirect restorations, such as gold or ceramic inlays or onlays. Where the primary tooth presents root resorption, caries, periodontal diseases and has a poor prognosis, extraction and prosthetic replacement, such as immediate or delayed implant supported crown, conventional fixed partial denture, removable partial denture, or resin bonded prosthodontics, may be necessary [4].
The rate of resorption of the roots of the primary molars has been observed to diminish with age. Early recognition and early thorough diagnosis are the most important factors for successful treatment [7].
In cases with agenesis of permanent mandibular second premolars, preservation of the primary molars helps to maintain the bone volume and reduce bone resorption, which will later facilitate placement of an immediate implant in patients around the age of 16 years.
Limited super-eruption of the opposing permanent tooth, as well as tipping of the adjacent permanent teeth, represents a common problem in proper assessment and consideration of the conditions frequently accompanying retained teeth at infra-occlusion positions [16]. In order to achieve an accurate diagnosis, radiographic examination is equally as important as clinical investigations. It represents an integral part of preserving efficient patient pre-procedural records and achieving an effective diagnosis, without which clinically significant data could be overlooked.
Retained primary molars must be carefully assessed so that all possible treatment options can be considered. If the permanent premolars were missing, preserving primary molars with or without modification is the most desirable option. The radiographic image must be carefully examined in such cases to detect submerged primary molars i.e. ankylosis or other associated problems, such as caries in the primary molars, resorption of the primary molars, periodontal problems and bone resorption, mesial tipping of the distal or mesial permanent tooth, and super-eruption of the opposing permanent tooth. Various treatment approaches have been proposed, which are dependent on the age of the patient, developmental stage of the root, the position of the primary molar, number of affected teeth, severity of tipping of the adjacent permanent teeth, and the presence or absence of the permanent mandibular second premolars [7].
Although several treatment options can be adopted according to the available circumstances, the exact starting point of intervention is difficult to decide. The dentist must keep the primary molars under observation and the patient should be recalled regularly for a follow-up to decide the optimal approach and timing for treatment intervention (Parisay et al., 2013). Dentists and patients should be educated to preserve persistent primary teeth as much as possible in cases with absence of permanent successor teeth, and appropriate treatment should be devised for each case. In cases with impaction of the permanent successor, the primary tooth should be extracted to allow spontaneous eruption of the permanent successor [17, 18]. Alternatively, combined orthodontic-surgical treatment might be indicated in certain conditions where eruptive force is lacking, to guide the permanent successor into its proper position by correcting its eruptive path in order to maintain functional and stable occlusion by correcting its eruptive path [19].
5. LIMITATIONS
The relatively smaller sample size and involvement of only a single center are limitations of this study, however, we took all the population that fits our inclusion criteria. The study findings should be validated in a larger sample size involving multiple centers from different regions of Saudi Arabia.
CONCLUSION
We found that primary molars were retained in 15.2% of the study population. The most frequent causes of primary molar retention were agenesis of the permanent successor, followed by ectopic eruption and impaction of the successor teeth. The most common problems associated with retained primary teeth were tipping of the adjacent permanent teeth, resorption of the primary molar, primary molar caries and pathology, and fillings required in the primary molar.
FUNDING
None.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
STROBE guidelines and methodology were followed.
CONFLICT OF INTEREST
The author declares no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
I would like to acknowledge Mr. Reda Khalil, Radiographic Technician at Umm Al-Qura University for his assistance in accessing the panoramic radiographs records for assessment and evaluation.

