All published articles of this journal are available on ScienceDirect.

Ultrasonography as a Diagnostic Aid in Evaluating Cystic Lesions, Benign Tumors and Malignancies of Maxillofacial Region: A Clinical Study
Abstract
Aim:
To evaluate the accuracy of Ultrasonography as a diagnostic aid in cysts, benign tumors and malignancies of maxillofacial region.
Objectives:
This study was conducted to evaluate the accuracy of ultrasonography in the diagnosis of the osseous lesions of the jaws including cysts, benign tumors and malignant tumors. All the findings obtained by ultrasonography were compared and correlated with the clinical diagnosis, radiographic diagnosis and histopathological findings.
Materials and Methods:
The study was conducted on 42 patients with osseous maxillofacial swellings. The clinical and radiographic examination was carried out for all the patients who were afterward subjected to ultrasonography with color Doppler followed by histopathology. All the findings obtained were then statistically analyzed.
Results:
The utility of ultrasonography was evaluated considering histopathology as a gold standard. The diagnostic accuracy of ultrasound was found to be 100% in cystic lesions, 80% in benign tumors, and 85.71% in malignant tumors.
Conclusion:
Ultrasonography provides an accurate imaging of the head and neck region and does provide information about the nature of the lesion, its extent, and relationship with the surrounding structures. We propose the use of ultrasonography as an adjunctive examination for osseous lesions of the jaws before any invasive treatment.
1. INTRODUCTION
Maxillofacial tumors are commonly encountered in dental clinics. History, the location of the lesion and radiographic findings can be helpful in the diagnosis; but due to the wide variation of the jaw lesions, sometimes the diagnosis becomes complex [1, 2]. In recent times, modern imaging techniques like digital radiography, Computed Tomography (CT), Magnetic Resonance Imaging (MRI) and nuclear medicine made an immense contribution in the diagnosis of intra-osseous and extra-osseous swellings in the head and neck region [2]. But very expensive equipment and non-availability universally limit their use in the routine cases.
Ultrasonography is recognized as a safe, noninvasive and inexpensive method that has been found to be a reliable and sensitive diagnostic tool in head and neck for the evaluation of soft tissue masses, vascular neoplasms, deep neck abscesses, salivary gland diseases, cancer and nodal metastases [3, 4]. Recent studies have focused on potential applications of ultrasonography for diagnosis of temporo-mandibular joint pathology [3], fractures of facial bones and evaluation of the periapical lesions [5].
Ultrasonography is based on non- ionizing radiations with no known adverse biological effect. USG; a dynamic imaging technique, also known as sonography or echography or real-time imaging is the imaging of the structures of the body by recording the echoes of pulses of ultrasonic waves directed into the tissues and reflected by tissue planes where there is a change in the density. This, in turn, depends on the acoustic impedance of the tissues. On electrically stimulating a piezoelectric crystal called a transducer the ultrasound waves are produced. As the ultrasound waves strike a boundary between tissues of varying acoustic impedance, the sound waves are reflected back to the transducer in the form of echoes which are converted into electrical impulses and are displayed on a computer system. The images obtained by real-time ultrasonography are interpreted in terms of anechoic, hypoechoic and hyperechoic. The principle of USG is based on the fact that, there are large differences in the impedance for ultrasound waves between the soft tissue and air, and between the soft tissue and bone. Bone and air are absolute barriers to an ultrasound beam, this means that no image within or behind bony or air containing structure can be produced by ultrasound [6].
Ultrasonography has still not found its place as a routine diagnostic aid in spite of being known as one of the most risk-free investigations for evaluating human diseases [3].Various studies have proved its accuracy in the diagnosis of soft tissue lesions and pathologies but not in osseous lesions. The literature reveals that high resolution ultrasound is an efficient and reliable investigation in evaluating tumor thickness and clearance of surgical margins of tumor. Ultrasonography serves as a commendable adjunct to clinical and conventional radiographic examination in the oral malignancies. This is a boon especially for the developing nations like India, because ultrasound is more economical than advanced modalities such as CT and MRI [2]. However, studies have shown that the investigating role of ultrasound in the diagnosis of bone lesions of the jaws is limited.
Although ultrasonography does not establish a definitive diagnosis, it facilitates differential diagnosis between solid and cystic lesions, it can assess the stage of infection and the exact anatomic location and provides an excellent guide to represent biopsy area.
This study was conducted with an objective to evaluate the accuracy of ultrasonography for the diagnosis of the osseous lesions of the jaws including cysts, benign tumors and malignant tumors. All the findings obtained by ultrasonography were compared and correlated with the clinical diagnosis, radiographic diagnosis and histopathological findings.
This study was done in continuation of our earlier study on the role of ultrasonography in maxillofacial swellings [5], but with a different aim and with a different set of pathologies as only a few studies have been done to evaluate the usefulness of ultrasonography in the diagnosis of osseous lesions such as maxillofacial cysts and tumors.
2. MATERIALS AND METHODS
Prospectively, 42 osseous jaw lesions were evaluated in patients who visited the department of oral medicine and radiology at ITS Centre for Dental Studies and Research, Muradnagar, Ghaziabad. A written consent was obtained from the study subjects. The patients reporting to the department with any swelling in the orofacial region were included in the study. The ethical clearance was obtained from the ethical board of the dental college.
2.1. Inclusion Criteria
The subjects with chronic orofacial swellings who had not undergone any previous investigations or treatment for the pathology were included. Only the subjects who fall clinically under the category of cysts, benign tumors or malignancies were selected.
2.2. Exclusion Criteria
The patients with acute swellings were excluded as the radiographic changes are not well appreciated in such conditions. The medically compromised patients with any systemic illness and patients who had undergone aspiration or any treatment for the swelling were excluded.
All the patients were explained about the study and were subjected to a detailed case history format. All the lesions were confirmed by detailed extra oral and intraoral clinical examination by trained and experienced oral medicine specialists. The best possible provisional clinical diagnosis was given based on history, clinical features and diagnostic criteria given in the literature depending on the type of the pathology. The patients were then subjected to routine radiography and findings were recorded.
All the patients were evaluated with LOGIQ-500 PRO ultrasound machine with color Doppler function, incorporating a linear array transducer, operating at a frequency of 8-12 MHz.
Ultrasound images are identified in terms of echoes as hypoechoic, hyperechoic and anechoic images [6, 7]. A mass is hypoechoic if it has an intensity lower than that of the adjacent tissue e.g. solid benign tumors. Hyperechoic is used for masses of higher intensity such as tumors and isoechoic is used for masses with intensity similar to the adjacent tissue. The appearance of hypoechoic masses is darker/black whereas the hyperechoic masses appear rather bright/white. A calcified mass appears hyperechoic and a clear fluid or blood appears anechoic such as cysts [8].
With the above background, all lesions were evaluated for location, shape, size, border, internal architecture, Doppler flow and echogenicity relative to adjacent tissues and based on the findings the ultrasonographic diagnosis was given.
Finally, histopathological examination of all the pathologies was carried out to set a gold standard for the comparison.
After completing the sample, for the statistical evaluation, the patients were divided into three groups based on clinical and histopathological findings. The group I consisted of cystic pathologies; group II consisted of benign tumors and group III consisted of malignancies.
3. RESULTS
42 subjects with an age range of 8 to 72 years were examined for maxillofacial osseous lesions. The study sample consisted of 20 (47.6%) females and 22 (52.3%) males.
3.1. Histopathological Diagnosis of Swellings
The histopathological diagnosis was made for 42 swellings. Out of which 18 (42.85%) were diagnosed as cystic pathologies, 10 (23.80%) as benign tumors and 14 (33.33%) as malignant tumors (Table 1).
| Total=42 |
Group I Cysts |
Group II Benign Tumors |
Group III Malignant Tumors |
|---|---|---|---|
|
Number of Cases |
18 | 10 | 14 |
| Percentage | 42.85 | 23.80 | 33.33 |
3.2. Cystic Lesions (Group1) as Compared on Clinical, Radiographic and Ultrasonography and Histopathology
Considering, histopathology as a gold standard, the diagnostic accuracy of clinical diagnosis and radiographic examination in evaluating cystic lesions was found to be 88.88% and 83.33% respectively. Ultrasonography could diagnose all the cystic lesions correctly with a diagnostic accuracy of 100%. Contingency coefficient was found to be highly significant showing a high association between the clinical diagnosis, radiography and ultrasonographic diagnosis in the evaluation of cystic lesions of the jaws (Table 2). The positive predictive value of ultrasonography for the cystic swellings was found to be 100% and the 95% confidence interval was found to be in the range of 74% - 100%.
| – | Group 1 | – | ||
|---|---|---|---|---|
| – | Histopathological Diagnosis | Clinical Diagnosis | Radiographic Diagnosis |
Ultrasonography Diagnosis |
| Cyst | 18 | 16 | 15 | 18 |
| Other diagnosis or no diagnosis | - | 2 | 3 | - |
| Diagnostic accuracy | 100% | 88.88% | 83.33% | 100% |
3.3. Benign Tumors (Group II) as Compared on Clinical, Radiographic, Ultrasonography and Histopathological Findings
In comparison to histopathology, the diagnostic accuracy of clinical diagnosis and radiographic examination in evaluating benign tumors was found to be 90% and 80%, respectively. Ultrasonography could diagnose 8 out 10 benign tumors with a diagnostic accuracy of 80%. One of the two lesions with odontoma as histopathological diagnosis had mixed cystic and solid appearance at ultrasonography and another one was inconclusive because of sclerotic texture. Contingency coefficient was found to be highly significant showing a strong association between the clinical diagnosis, radiography and ultrasonographic diagnosis in the evaluation of benign lesions of the jaws (Table 3). The positive predictive value of ultrasonography for the benign tumors was found to be 100% and 95% confidence interval was found to be in the range of 0.44 - 0.97.
| – | Group 1I | – | ||
|---|---|---|---|---|
| – | Histopathological Diagnosis | Clinical Diagnosis | Radiographic Diagnosis |
Ultrasonography Diagnosis |
| Benign tumors | 10 | 9 | 8 | 8 |
| Other diagnosis or no diagnosis | - | 1 | 2 | 2 |
| Diagnostic accuracy | 100% | 90% | 80% | 80% |
3.4. Malignancies (Group III) as Compared on Clinical, Radiographic, Ultrasonography and Histopathological Findings
The diagnostic accuracy of clinical diagnosis and radiographic examination in evaluating malignant tumors was found to be 85.71% and 78.57%, respectively. Ultrasonography could diagnose 12 out of 14 malignant tumors with a diagnostic accuracy of 85.71%. A significant association was observed between ultrasonography, clinical diagnosis and radiographic diagnosis with p-value < 0.000 and a highly significant contingency coefficient (Table 4). The positive predictive value of ultrasonography for the malignancies was found to be 100% and 95% confidence interval was found to be in the range of 0.57-0.982.
| – | Group 1II | – | ||
|---|---|---|---|---|
| – | Histopathological Diagnosis | Clinical Diagnosis | Radiographic Diagnosis |
Ultrasonography Diagnosis |
| Malignancies | 14 | 12 | 11 | 12 |
| Other diagnosis or no diagnosis | - | 2 | 3 | 2 |
| Diagnostic accuracy | 100% | 85.71% | 78.57% | 85.71% |
3.5. Diagnostic Accuracy of Ultrasonography as Compared to Histopathology
The histopathology was considered as a gold standard. Ultrasonography was able to diagnose accurately 100% in cystic, 80% in benign tumors and 85.71% in malignant tumors. The diagnostic accuracy of clinical examination, radiography and ultrasonography was found to be 88.09%, 80.95% and 90.47% respectively in comparison to histopathological diagnosis in maxillofacial osseous pathologies.
4. DISCUSSION
Ultrasonography provides an accurate imaging of the head and neck region and does provide information about the nature of the lesion, its extent, and relationship with the surrounding structures. As stated by Peterson et al., in 2003, the various lesions manifesting in the maxillofacial region need different treatment plans and thus it is necessary to have accurate information on the pathological nature of the lesion [9].
Ultrasonography has been proven to be a valuable diagnostic modality for the evaluation of head and neck lesions [7-9]. In 1996, Luciano et al., evaluated the role of ultrasonography as a complementary examination in the diagnosis of bony jaw lesions and reported positive ultrasonography findings in the differential diagnosis of intraosseous lesions of the jaws [10].
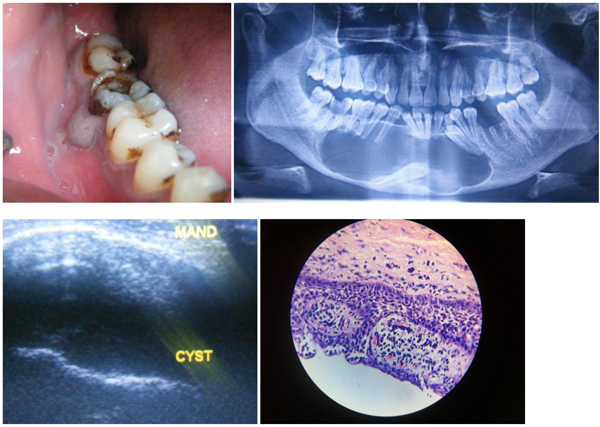
In the present study, 18 cases were diagnosed histopathologically as cysts. This included three odontogenic keratocyst, three dentigerous cysts and twelve radicular cysts (Table 2). Radicular cyst appeared as anechoic well-defined lesions (Fig. 1). Three odontogenic cysts had mixed solid and cystic appearance on ultrasonography which were Odontogenic keratocysts. Vascularization was not detected at Doppler ultrasonography in 17 lesions. Peripheral vascularization was detected in one lesion with a final diagnosis of the infected radicular cyst.
Cotti E et al., in 2002 did a similar study in 11 patients and obtained 100% agreement between ultrasonography and histology in all their cases [11]. The present study reported a diagnostic accuracy of 100% for ultrasonography in the diagnosis of cystic lesions and the results harmonize with the studies of Gundappa et al., in 2006 [12] and Shambulingappa et al., in 2012 [4] which also reported a sensitivity of 100%.
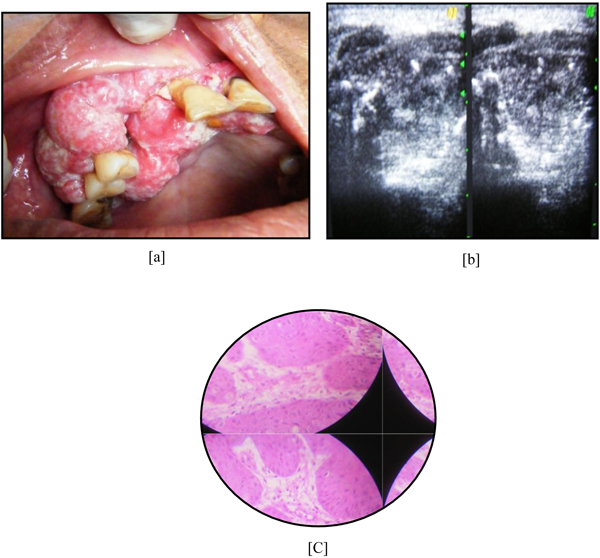
Group II consisted of 10 benign odontogenic and non-odontogenic tumors confirmed histopathologically. Ultrasound was able to identify 8 benign tumors which included two hemangioma, 3 ameloblastomas, 2 central giant cell granuloma and 1 odontogenic myxoma (Fig. 2). The diagnostic accuracy of ultrasound was found to be 80% in the diagnosis of benign tumors.

Kalinowska et al., 2007 [13] reported that ultrasound can characterize the flow of blood and can differentiate hemangiomas from other lesions. In the present study, one out of two hemangiomas which was clinically considered to be some traumatic lesion was found to be hemangioma on color Doppler ultrasonography. Mehdizadeh et al., in 2009 [14] reported 100% sensitivity of ultrasound in the diagnosis of solid tumors.
Group III constituted 14 cases which were diagnosed histopathologically as malignancies. “It included 10 cases of squamous cell carcinomas, one adenocarcinoma of salivary glands and one case of osteosarcoma, one primary intraosseous carcinoma and one malignancy of maxillary sinus”. Ultrasonography could identify 12 malignancies including adenocarcinoma and osteosarcoma. One case, which was histopathologically primary intraosseous carcinoma, where ultrasound provided with a wrong diagnosis, the lesion was small and without destruction of the cortex, which hampered the use of this technique.
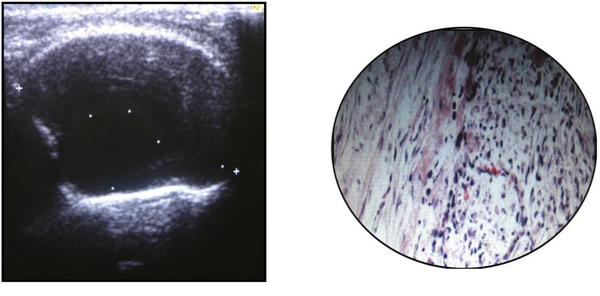
Malignant tumors showed complex echo texture with heterogeneous internal echo pattern and irregular boundaries (Fig. 3). These findings were in accordance with the studies of Bhosle in 1992, Jacob A., in 2007 [15], Sumer et al., [16], and Wakasugi et al., [17].
Unlike radiography, adverse effects of ultrasonography have not been reported. The method is quick, widely available, relatively inexpensive, painless, reproducible and can be repeated as often as necessary without any risk to the patient. Thus, ultrasonography can be a valuable aid to the diagnosis. The results in the presented study state that ultrasonography can be used safely and efficiently in the diagnosis of maxillofacial osseous swellings. The findings in the present study are in concordance with the study done by Garg et al., in 2017 [18] and Shah et al., [19].
Musu et al., in 2016 reviewed ultrasonography in the diagnosis of bony lesions of the jaws [20, 21]. This review determined that ultrasonography can be used effectively for the diagnosis of infective and/or inflammatory lesions, cysts, non-odontogenic tumors, odontogenic tumors, and arteriovenous malformations and for the differential diagnosis of lesions of endodontic origin, compared with the gold standard of histologic analysis.
A similar previous study was done by us eight years back to evaluate the efficacy of ultrasonography in evaluating “soft tissue as well as hard tissue” pathologies of maxillofacial region with a small sample size. “Ultrasonography for soft tissue pathologies is already been well recognized. But when it comes to the bony pathologies this non-ionizing, biologically safe and comparatively less expensive modality has still not found its place as a routine diagnostic technique which is much needed in developing countries such as India where most of the patients cannot afford the expensive diagnostic techniques”. Thus, there was a need for further research regarding the accuracy of ultrasound in hard tissues/ bony pathologies so that it can be extensively and widely used. Thus, in view of this, a newer present study was planned to evaluate the accuracy of ultrasonography in the pathologies which involve bone but with different sample size, different demographic data and with the aim restricted to the pathologies involving the hard tissues/bone.
The present study evaluated accuracy USG in only “cysts, tumors and malignancies” which was the need of the hour as the use of USG in soft tissues is already well established in the previous studies. The present study included pathologies of wide varieties with different sources of origin to widen the use of ultrasonography. “The results suggest that whenever there is a breach in the continuity of the bone, ultrasonography can be used with high accuracy and efficacy”. The previous study evaluated the accuracy and contingency coefficient between different groups whereas the present study evaluated the accuracy, positive predictive value and confidence interval between the different groups. Thus, the present study further adds to the literature about the use of this biologically safe imaging process.
A limitation of the present study is the smaller sample size used especially for the tumors. Further studies exclusively on tumors with a larger sample size should be carried out to prove its accuracy in the diagnosis of such pathologies.
CONCLUSION
The results of the present study allow concluding that ultrasonography can be a good and economical alternative for the diagnosis of maxillofacial swellings including osseous swellings such as cysts, benign and malignant tumors. The USG modality can be used with the greatest accuracy with the cysts whereas in benign and malignant tumors it could be used as an adjunctive investigation. Proper diagnosis is the backbone of the treatment planning which could be achieved better if ultrasonography is used as an adjunctive investigation. This will improve management of the patients in clinical practice as it provides several advantages like it is non-invasive, easily reproducible, widely available, rapid, and inexpensive.
Suggestions by The Authors: All the dentists should be well versed with this imaging technique and more studies should be done to promote the usefulness of ultrasonography. It can be carried out as a routine diagnostic test for evaluating various maxillofacial pathologies, thereby providing an early diagnosis and treatment planning required for better patient care.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical clearance was obtained from the ethical board of the I.T.S. Dental College.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
A written consent was obtained from the study subjects.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
None declared.

