All published articles of this journal are available on ScienceDirect.

Influence of Taper of Root Canal Shape on the Intracanal Bacterial Reduction
Abstract
Objectives:
Taper is a factor that determines final root canal dimensions and consequently, the space available for the cleaning action of irrigants. Therefore, the aim of this study was to investigate the influence of taper on intracanal bacterial reduction.
Methods:
Sterilized root canals of 25 mandibular incisors were inoculated with E. faecalis and then divided into two experimental groups and one control group (A= saline, B= NaOCl + EDTA and C= control, not prepared). Groups A and B were prepared to an apical size of #30/0.04, a culture was obtained and then prepared to #30/0.08 and cultured again. Final irrigation sequence was 30 ml of saline for group A and 10 ml of 17% EDTA followed by 10 ml of 2.5% NaOCl and 10 ml of saline for group B. The CFU ml-1 of the pre- and two post-operative samplings were recorded. Values were compared by performing ANOVA and FDR for multiple hypothesis testing.
Results:
No statistically significant difference between initial CFU ml-1 readings was recorded, whereas significant differences between group A and B at both 4% and 8% tapers were noted. Furthermore, a linear-dependent reduction of CFU ml-1 was recorded in each group from non-instrumented root canals to #30/0.04 and subsequently to #30/0.08. The positive control group shows the expected reduction of bacterial count.
Conclusion:
Chemomechanical instrumentation was more efficient at reducing E. faecalis when the taper of root canals increased from 4% to 8% and NaOCl plus EDTA led to a greater intracanal bacterial reduction than saline, regardless of the taper achieved.
INTRODUCTION
During and after its mechanical preparation, root canal (RC) should be cleaned with irrigation solutions. The dimensions of RC determine the irrigants’ volume and, consequently, describe their efficacy. In 1965, Wandelt [1] stated that only a small and ineffective volume of a chelator can be placed in narrow root canals. In a recent study, Brunson et al. [2] confirmed Wandelt’s statement, showing that an increase in root canal dimensions leads to an increase in the mean volume of irrigant used inside the canal. The clinician has the ability to alter root canal dimensions by changing the final apical preparation size and/or the taper.
In the era where endodontic instruments were handly used, keeping the apical preparation as wide as possible was believed to be the only way for the irrigation fluids to reach and reduce the microbial population at the critical apical 3 mm of the root canal [3-7]. On the other hand, it is believed that if apical preparation could be kept as narrow as possible while increasing root canal taper by using nickel-titanium rotary systems, this would create a greater deposit for the irrigation fluids [8]. At the same time, it would lead to the greater removal of dentin from the canal walls, thus producing a cleaner root canal [8].
Although the effect of the taper of a root canal on its smear layer and/or debris elimination [9-11], as well as on irrigant volume [2, 12, 13], have been studied, the taper influence on intracanal bacterial reduction has not been studied as a separate variable. Therefore, the aim of this paper is to investigate the influence of taper on intracanal bacterial reduction.
MATERIALS AND METHODS
Twenty-five single canal mandibular incisors, which had been freshly-extracted for periodontal reasons and stored in 10% formalin, were used in this study.
Specimens’ Preparation
Teeth were cut at the level of the cementoenamel junction perpendicular to their long axis by a diamond disk, 10 mm from the root tip. Patency of the RCs was ensured by using a #10 K-file (Dentsply/Maillefer, Ballaigues, Switzerland); root canals were prepared to an apical size #20 ISO and irrigated with saline for residual pulp tissue removal. In order to remove the smear layer from the RCs, teeth were treated with 17% EDTA in an ultrasonic bath (Vista Dental Products, Racine, WI) for 10 minutes and with 2.5% NaOCl solution for another 10 minutes.
Finally, the apical 3 mm of each specimen, including the foramen, was covered with acrylic resin (Dyract AP, DeTrey, Dentsply, UK) to prevent any extrusion or leakage of materials during root canal preparation and sample collection.
Specimen Sterilization
Aliquots of 5 ml sterile Tryptic Soy Broth (TSB) solution were added to vials containing each specimen. Agitation was performed for about 15 min in an ultrasonic bath to aid the penetration of TSB into the RC and then the samples were autoclaved at 121°C for 30 min. Following that, samples were incubated for 48h at 37°C in 10% CO2. Frequent visual checks were made to assess and reject any specimen in which TSB in the vials became turbid, as this indicated that bacteria had survived.
E. faecalis Culturing and Specimen Inoculation
Sterile samples were captured with wet sterile gauze, covered externally with two nail varnish layers and then placed in an upright position in a special plastic sterile sheath (Terassaki wells, E & K Scientific Products, Santa Clara, California). After the canals were dried with sterile paper points, they were infected with E. faecalis (ATCC 29212). An E. faecalis suspension was prepared in BHI broth which was incubated for 48 hours at 37°C in 10% CO2. This suspension was adjusted to a turbidity of 0.5 on the McFarland scale (1.5 x 108 bacteria/ml), and 0.1 ml was inoculated into each canal. A size #10 K file was used to mix the content of the root canal five times, with peripheral movements up to working length. The inoculated teeth were then incubated at 37°C in 10% CO2 for a week. Every second day of incubation, 0.1 ml TSB was added to each sample.
Pre-operative Sampling
Control of contamination was done by collecting the fluids from RC with three sterile paper points for 30 sec each, which were immediately placed in test tubes containing 1ml TSB. Then, they were vortexed for 30 sec and 0.1 ml was cultivated on blood agar plates at 37°C in 10% CO2 for three days. With the described process, the colonization of all RCs with E. faecalis was determined and the calculation of CFU ml-1 was performed.
Specimen Grouping and Chemomechanical Preparation
Roots were randomly divided into 2 experimental groups (A and B, n=10 each) and one control group (C, n=5). Instrumentation was performed to a working length of 9mm, with GT rotary files Series 20 and 30 (Dentsply/ Maillefer), placed in the hand-piece of an Endo IT motor (Aseptico, Woodinville, WA). A protocol was used to ensure that the root canal taper was 4% (phase I) and finally 8% (phase II). In phase I, GT file Series 30 was used in a crown-down manner. Files 30/0.10, 30/0.08, and 30/0.06 were placed 2, 5, and 7 mm inside the canal, respectively, and file 30/0.04 placed to working length. In phase II, instrumentation of the root canals continued with files 20/0.08, 30/0.06, 20/0.10 and 30/0.08 to length. During the procedure, light lateral pressure was applied to the canal walls. Between files, canals were irrigated with saline in group A or 2.5% NaOCl in group B with a 27-gauge blind-ended endodontic irrigation needle (Hawe Max-I-probe; Kerr-Hawe, Bioggio, Switzerland). The volume of irrigant flushed after each file was 3 ml. The final irrigation sequence was 30 ml of saline (group A) or 10 ml of 17% EDTA (Vista Dental Products, Racine, WI) for 3 minutes, followed by 10 ml of 2.5% NaOCl and 10 ml of saline (group B). The total amount of irrigants used in each canal in each phase was 42 ml. Roots in control group were inoculated but not mechanically prepared. All procedures were carried out by the same operator (M.P) to reduce variables.
Post-operative Samplings
After achieving 4% conicity, RCs were dried with sterile paper points, irrigated with 5 ml of 5% sodium thiosulfate for NaOCl neutralization and dried again in the same manner. One ml of TSB was then transferred into each canal and a #10 K file was used to mix the root canal content 5 times, with peripheral movements, up to working length. Three sterile paper points were used consecutively for 30 sec each and finally transferred to test tubes containing 1 ml of TSB solution. The same procedure was repeated when a conicity of 8% was achieved in the same RCs.
Culturing Procedures
Test tubes containing paper points and TSB were vortexed for 30 sec and two serial 10-fold dilutions were used to inoculate blood agar plates. Each agar plate was inoculated with 0.1 ml of the undiluted sample and also with each of the two dilutions. The plates were incubated at 37°C in 10% CO2 for 3 days at which point CFU ml-1 calculations were performed.
STATISTICAL ANALYSIS
Data are expressed as mean ± 1 standard deviation (S.D.) for continuous variables. The normality of the distributions was assessed with Kolmogorov-Smirnov test and graphical methods. Comparisons between more than two groups were performed with Analysis of Variance (ANOVA). The Kruskal-Wallis test was utilized as a non-parametric test for multiple group comparisons, using the Mann-Whitney U test and FDR for post hoc multiple testing. Comparisons between more than two measurements were performed using Repeated Measures ANOVA, along with Friedman’s test and Wilcoxon’s signed rank test with FDR as non-parametric tests. The Pearson correlation coefficient and the Spearman rho were calculated in order to examine linear relationships between variables. In all cases of multiple hypothesis testing, FDR was utilized in order to assess between-group differences, as well as to control family-wise error to <0.05. All tests were two-sided. Differences were considered statistically significant if the null hypothesis could be rejected with >95% confidence (p<0.05).
RESULTS
There was no statistically significant difference between the initial CFU ml-1 of all groups (p>0.05). All instrumentation and irrigation sequences used in this study significantly reduced the number of bacterial cells in the root canals; however, total elimination of the bacteria was not achieved with any of the techniques.
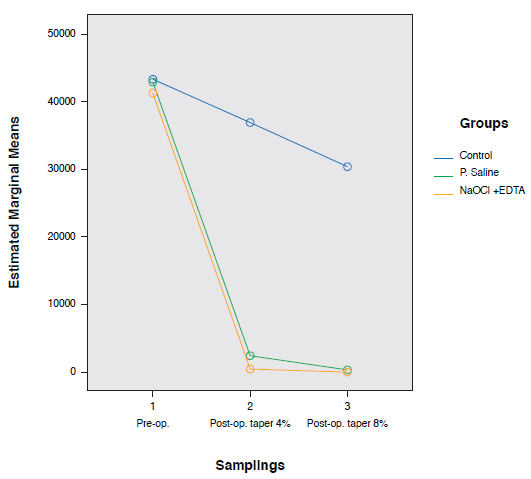
There was a statistically significant difference of CFU ml-1 between group A (Saline) and group B (NaOCl + EDTA), at 4% and 8% tapers (p<0.001), as well as between each experimental group and the control group, at 4% and 8% tapers (p<0.001). Also, a significant reduction in CFU ml-1 was recorded when the same specimens were prepared to 4% taper and subsequently to 8% taper, in each group (p<0.01). The positive control group shows the expected reduction of bacterial count (p<0.05). (Table 1, Fig. 1).
| Group | Mean | Std. Deviation | N | |
|---|---|---|---|---|
| CFU *** Pre-op. sampling |
Control ° † | 43222.00 | 10297.423 | 5 |
| P. Saline ° | 42916.00 | 13494.894 | 10 | |
| NaOCl + EDTA ° | 41216.00 | 10199.904 | 10 | |
| Total | 42297.20 | 11216.236 | 25 | |
| CFU *** Post-op. sampling Taper 4% |
Control * † | 36976.00 | 8355.048 | 5 |
| P. Saline * | 2455.00 | 1468.357 | 10 | |
| NaOCl+ EDTA * | 512.00 | 268.361 | 10 | |
| Total | 8582.00 | 14940.196 | 25 | |
| CFU *** Post-op. sampling Taper 8% |
Control ** † | 30330.00 | 7619.403 | 5 |
| P. Saline ** | 379.00 | 170.909 | 10 | |
| NaOCl + EDTA ** | 67.00 | 24.967 | 10 | |
| Total | 6244.40 | 12679.876 | 25 |
DISCUSSION
The objective of the present study was to evaluate the influence of taper on intracanal bacterial reduction. Therefore, RCs were prepared to a standard apical size of #30/0.04 and subsequently to #30/0.08. Saline and a combintion of NaOCl and EDTA were used in two separate groups as irrigation solutions. Size #30 was chosen as a final apical size because it was shown to be the minimum apical preparation size which provides irrigants with apical access [14].
Our findings showed that there was a significant reduction in CFUs when the same specimens were prepared from #20 ISO to #30/0.04. Subsequently, a further and significant reduction was noted in each group when taper was increased from 4% to 8%.
The higher reduction of the microbial load which was associated with the greater taper produced in our research, when the apical preparation was kept at a standard size, can be explained in two ways: first, due to the greater removal of infected dentine from the RC walls, as has been proven earlier [8]; and second, due to the greater irrigant volume which was delivered as taper was increased. The latter was confirmed by previous researchers [2, 13].
However, there are currently conflicting findings about the influence of the increased RC taper on the intracanal microbial load reduction. Our results are in agreement with those of other groups [15, 16] who prepared root canals to a standard apical preparation size of #30 and #40, using different rotary and hand instruments and who concluded that greater intracanal microbial reduction was evident when the highest taper degree was achieved. Coldero et al. [17] also showed that the coronal flare generated by GT rotary and Profile instruments is sufficient to allow access to the apical part of the root canal with antimicrobial irrigant without the need for the removal of dentine at the working length.
However, our results do not agree with those of other researchers [18-20] who studied the influence of different rotary systems or techniques on the intracanal bacterial reduction. Siqueira et al. [18] found that canal preparation to #30/0.02 with Nitiflex was significantly more effective than a GT file 0.12 taper in reducing the number of intracanal bacteria. It is possible that the oscillating motion that they used with Nitiflex files compared with the pecking motion of the GT files was the cause of this unexpected result.
Similarly, Aydin et al. [19] failed to prove that dentin removal through greater-tapered instrumentation can reduce the intracanal bacterial load more effectively than conservative instrumentation. They used rotary instrumentation techniques with an in-out motion and with no lateral pressure applied to the root canal walls of mandibular premolars. As mentioned by that group, it is possible that surfaces harboring bacteria in ovoid extensions remained untouched by the instruments, and were later sampled, thereby yielding the recovery of bacteria of similar quantity in both groups.
Chuste-Guillot et al. [20] intended to compare the intracanal bacterial reduction achieved by instrumentation using stainless steel K-files versus three NiTi rotary instruments. In this study, different teeth groups, different tapers and different apical sizes were used. As a result, anatomical and motion differences reported by the different investigation groups may have led to the identification of no differences between the techniques used.
Our results confirmed a large number of previous studies which have proved that even though mechanical preparation leads to a significant intracanal bacterial reduction, the combined utilization of antimicrobial irrigant solutions can result in even greater reduction [21-23]. However, post-operative samplings of RCs where NaOCl and EDTA were used demonstrated that despite instrumentation and antiseptic irrigation, bacteria could remain, maintaining the infection inside the pulp canal space. The aforementioned result is similar to that of previous studies [24-26].
Finally, it would be interesting to further investigate the efficacy of passive ultrasonic irrigation on microbial reduction when applied to root canals of different tapers.
CONCLUSION
Our results support the concept that the degree of the taper preparation is important for the reduction of intracanal bacterial load. Achieving 8% conicity of the root canal shape led to a greater intracanal bacterial reduction, than 4% conicity. Irrigation protocol used in clinical practice can lead to a greater reduction of intracanal bacterial load, regardless of the degree of taper.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
This article was adapted from a thesis submitted by Dr. Mary Th. Paraskevopoulou in partial fulfillment of the requirements for the MSc degree in Endodontics at University of Athens, School of Dentistry. We acknowledge the Technical Assistant of the Medical Laboratory, Mrs. Efterpi Kontou, for her assistance in the microbiological procedures used in this research.

