All published articles of this journal are available on ScienceDirect.

Conservative Socket Regeneration with Buccal Wall Defect Using Guided Tissue
Abstract
Progressive alveolar bone resorption after tooth extraction may lead to surgical and prosthetic-driven difficulties, especially when deciding to use a dental implant to replace the extracted tooth. This case report discusses an irreparable lower left second premolar tooth with a periodontal lesion on the buccal side. A preservative tooth extraction was performed. Then, the socket was grafted with bovine bone, a collagen membrane was placed between the buccal bone and the attached gingiva, covering the bone dehiscence buccally, and the socket without a flap was raised. After a 6-month healing period, there was minimal socket width resorption and a shallow buccal vestibule. The implant was placed with high primary stability and sufficient buccal plate thickness. In conclusion, this guided tissue regeneration technique can minimize alveolar bone resorption in a socket with buccal dehiscence, but technical difficulties and shallowing of the buccal vestibule still exist.
INTRODUCTION
Many causes and factors can lead to buccal wall socket defects or loss, with a common factor being periodontal lesion [1]. Periodontal lesions can cause bone resorption and destruction during lesion expansion, leading to sinus discharge or chronic swelling [2]. After extraction of a tooth with a periodontal lesion, socket collapse will occur, leading to fibrous tissue formation and narrowing of the alveolar ridge [3].
With the evolution of socket preservation and socket grafting, many grafting materials and techniques have been reported [4-7]. Many reports agree that socket grafting preserves the socket from collapse and is better than a non-grafted socket or a socket that underwent normal healing [4-7]. Other studies have found that covering the grafted socket with a collagen membrane or soft tissue graft provided better results than uncovered grafted or non-grafted sockets in terms of the amount of bone formation [6, 8]. One reason for this result is that the collagen membrane preserves the blood clot, maintains the space and prevents soft tissue migration into the socket [9].
However, using bone graft material alone without a collagen membrane or soft tissue coverage may result in a lower percentage of bone formation [4, 8]. A study conducted by Bozidar et al. [10] showed that sites that were grafted with a membrane demonstrated a more uniform bone structure in both the apical and coronal regions of the sockets. Tarrnow [11] invented his technique (ice cream cone) to augment the socket with buccal dehiscence, but his technique is only recommended for simple dehiscence and not a wall defect. Briefly, the technique involves shaping the collagen membrane into an ice cream cone shape and placing it inside the socket, which will cover the dehiscence site and the socket occlusally at the same time. However, this technique is not applicable for a completely defective or missing bone wall unless a flap is raised and a guided bone regeneration (GBR) procedure is performed. This case report describes an attempt to invent a new technique using GBR for a socket wall defect without a flap.
CASE REPORT
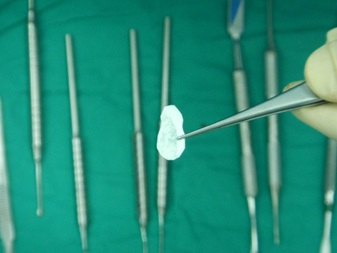
The patient was a 55-year-old woman with history of hypertension that was under medical control. The patient presented at this facility complaining of recurrent infection, tenderness and swelling in the lower left second premolar tooth. When the patient was examined clinically, a badly carious tooth with a 5-mm swelling buccally Fig. (1) and grade I tooth mobility was found with mild tenderness to percussion. A periodontal probe was used to examine the pocket depth, revealing a depth of greater than 7 mm on the buccal side. A radiograph showed that the lower left second premolar tooth had periodontal widening, periapical radiolucency and proximal bone resorption. Plaque control and motivation start before implant placement, for mal alignment teeth the patient needed to instruct about interdental plaque control through the periodontal aid. The patient was briefed regarding her situation and the treatment plan. After discussing the options with the patient, she agreed to remove the tooth with socket preservation and a healing period of 6 months before an implant would be placed to replace the missing tooth. Under local anesthesia, a periotome was used to first cut the periodontium and then luxate the tooth Fig. (2). Finally, a lower forceps was used to remove the tooth without trauma. After tooth extraction, the socket was examined with a periodontal probe to estimate the width and depth of the buccal bone defect. The defect was 9 mm in depth and 5 mm in width at the crestal bone. Curettage was performed in the socket with a spoon excavator, and the remaining soft tissue with inflammation was removed. Using a scalpel, a small pouch was created between the bone and the gingiva, which will allow the periosteal elevator to reflect the gingiva around the defect for placement of the collagen membrane Fig. (3). The collagen membrane was shaped to cover the buccal bone defect with at least 1-mm spacing from the bone margin defect to ensure the membrane would not collapse inside the socket. The membrane was shaped according to the shape of the bone defect; in this case, it was shaped like an “Ice Man” Fig. (4). The membrane was placed above the bone and below the gingiva, and the membrane was confirmed to be resting on the remaining buccal bone plate Fig. (5). One difficulty of this technique occurs when the membrane becomes wet with blood, resulting in the membrane becoming soft and thus not rigid enough to be pushed underneath the gingiva. Another difficulty is the limited access space and view in this procedure due to the delicate tissue. All these factors make this technique difficult, requiring more time and microsurgery instruments to perform atraumatic surgery. After collagen membrane insertion, part of the collagen membrane should remain outside the socket to cover the socket after bone graft placement. Bovine bone (Cerabone, Botiss, Berlin, Germany) was mixed with saline and applied in layers inside the socket without packing until reaching the bone level Fig. (6). Next, the exposed part of the collagen membrane was flipped to cover the grafted socket, with a margin of the membrane tag underneath the gingival margin. Vicryal suture 4/0 was used to secure the membrane in place with a Fig. (8) suture Fig. (7). Postoperative instruction was given to the patient, with special care to clean the exposed membrane. The patient was advised to use a 0.12% chlorhexidine mouthwash after each meal, using an irrigation syringe. A combined antibiotic was prescribed (amoxicillin 500 mg tds for 5 days and metronidazole 200 mg tds for 5 days). Paracetamol was also prescribed to control the pain. After two weeks, the sutures were removed, the wound healed uneventfully, and the membrane remained exposed. After one month, the wound was completely closed with healthy gingival tissue.

After 6 months, the patient returned for a review and augmented site evaluation. There was mild buccal plate resorption and shallowing of the buccal vestibule Fig. (8). Under local anesthesia, a crestal incision was performed to expose the crestal bone. An implant with a 3.6 mm diameter and 10 mm length (Dentium, superline) was selected for the missing tooth (no. 34). Bone drilling and an osteotomy were performed according to the manufacturer’s recommendations. The implant was placed with more than 45 Ncm torque with high primary stability Fig. (9). A non-submerged implant was selected due to its high primary stability, and flap closure was performed with cut gut suture 3/0. Postoperative instructions were given to the patient. The sutures were removed after one week. The wound healed uneventfully, and the implant was loaded after 3 months.







DISCUSSION
Socket preservation with the GBR procedure has been approved by many studies with different grafting materials and techniques. Studies have found that collagen membrane placement during the socket grafting procedure produces better results than no collagen membrane placement [4-7].
In our case report, there was a need for socket regeneration rather than socket preservation. Most of the procedures for socket regeneration are performed with a raised flap and complete surgical field exposure. The ice cone technique, which was invented by Tarrnow et al. [11], is indicated when socket dehiscence is detected but there is no socket wall defect. Advance technique maybe needed to improve the implant site such as bone block, flap advancement technique and novel material of bone grafting [12-14]. In term of implant site development, bone morphogentic protein play a crucial role in enhancing bone formation and speed up healing time [15, 16]. The drawbacks of a raised flap during socket augmentation are flap tension, wound dehiscence, decreased vestibule depth and decreased amounts of keratinized tissue [17]. Additional drawbacks include post-operative complications from pain, edema and the need for suturing and suture removal. Therefore, in this case, we tried to be more conservative and proceeded with socket augmentation without flap reflection [18, 19]. Collagen membrane insertion between the bone and mucogingival tissue became difficult as the membrane softened when exposed to fluid. Additionally, the limited space for insertion of the collagen membrane made the procedure more difficult to perform. Our procedure found that socket preservation can minimize, but not eliminate, bone resorption as buccal bone resorption was found at the time of implant placement. Another interesting drawback of this technique is the shallowing or decrease in the depth of the buccal vestibule at the end of healing period. Although the flap was not raised and flapless socket preservation was performed, the disadvantages of flap reflection still remained. This drawback may be due to periosteal detachment on the buccal side that may lead to wound contracture or to placement of the collagen membrane between the buccal plate and the gingival tissue, which leads to soft tissue adhesion to the membrane and omission of the buccal vestibule.
CONCLUSION
This guided tissue regeneration technique can minimize alveolar bone resorption in a socket with buccal dehiscence, but technical difficulties and shallowing of the buccal vestibule still exist.
CONFLICT OF INTEREST
The author confirms that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Special thanks go to Monica Arrogancia and Lee Li Chong for their extensive assistance with the clinical portion of this study.

