All published articles of this journal are available on ScienceDirect.

Variable Torque Prescription: State of Art.
Authors Info & Affiliations
Abstract
The variable prescription is widely described under the clinical aspect: the clinics is the result of the evolution of the state-of-the-art, aspect that is less considered in the daily literature. The state-of-the-art is the key to understand not only how we reach where we are but also to learn how to manage propely the torque, focusing on the technical and biomechanical purpos-es that led to the change of the torque values over time. The aim of this study is to update the clinicians on the aspects that affect the torque under the biomechanical sight, helping them to understand how to managing it, following the “timeline changes” in the different techniques so that the Variable Prescription Orthodontic (VPO) would be a suitable tool in every clinical case.
INTRODUCTION
In orthodontics the meaning of the torque is different clinically and biomechanically. Clinically, the “torque” is the third key of the occlusion, described by Andrews as the inclination of the dental crown antero-posteriorly in the frontal teeth and traversal in the backward teeth. The clinical evaluation of torque is made by tracing a line perpendicular to the dental margin and passing through the Facial Axis Crown (FAC) of the tooth: the torque is considered “positive” when the crown is in a forward position to the line and the root is in backward position: in the opposite situation there is the “negative” torque [1]. Biomechanically, the torque is represented by the torsion of a rectangular archwire in the bracket slot [2]. The adequate torque is related to good aesthetics, a correct anterior guidance is associated with the overjet and overbite correction: conversely a limitation of torque control in the anterior area causes a shortening of the dental arch, while a limitation of torque in the posterior area can determine a narrower smile and possible interferences [3-5]. Considering the importance of the torque management, the knowledge of the factors affecting the torque is mandatory: the torque depends on the dental morphology, the arch wire material, the bracket position and ligature [6-2]. The bracket/archwire interaction is one of the most discussed items within torque management and control, especially in this historical moment, where the self-ligating brackets are catching on the orthodontic view: the self-ligating brackets present advantages such as achieving a good occlusion associated to a good aesthetics, less treatment time, less time at the chair side with less appointment need and greater patient satisfaction [13, 14]. The advantages of self-ligating brackets have a high support by clinicians and a lower support by the evidence, especially on the toque management, where the maintenance/loss of torque in the bracket is debated [15]. The aim of this review is to describe the current state of the art, following the timeline of the different techniques, from the pre-adjusted system to the VPO: this update allows the clinician to understand the mechanisms that underlying the torque control, giving guidelines for each clinical situation.
MATERIALS AND METHODS
The literature has been reviewed to describe the historical development of the appliances, from the origin of the pre-adjusted appliance until the Variable Prescription Orthodontics, especially regarding to the change of the bracket-wire interaction and the change of the biomechanical principles that underlying various techniques and justify different torque management.
The Origin of VPO
The pre-adjusted appliance started with Lawrence Andrews, author that re-evaluated the previous orthodontic experiences that began his research studying the occlusion and identifying six keys of optimal occlusion: the third key is represented by the torque and the technique was characterized by a bracket containing the angulation, inclination and in-out of each tooth, interacting with a straight-wire [1,16-19]. The aim of Andrews was to achieve the six keys of the occlusion, using different bracket prescriptions for each clinical situation, dividing the extractions cases from non-extraction cases [20] Table 1. Subsequently, Roth criticized Andrews furnishing of brackets: Roth sustained that a large inventory was difficult to manage, so he suggested a new prescription that he called Straight Wire, with a unique torque value of the upper canines (11°), aiming to use the same brackets for extractions and non-extraction cases [21]. The idea of Roth was to develop a new treatment planning aiming to achieve a facial and dental aesthetics associated to a functional occlusion, a healthy periodontium and healthy TMJ Table 2. The third-generation of Straight wire devices is represented by the MBT technique. McLaughling, Bennet and Trevisi modified the prescriptions of Roth and Andrews: this modification is due to the introduction of a sliding mechanics, so that light forces could be used to close the extraction spaces. The versatility of torque is represented by three different prescriptions for the upper and lower canines, choosing the correct value on the malocclusion characteristics and on the treatment goals [22, 23] Table 3. The MBT technique added to Andrews’s and Roth’s treatment goals also that the condyle has to be seated in a centric relation and the musculature has to be in a relaxed position during the occlusion [22, 23].
Prescription in Andrews technique.
| Upper Arch | Inclination | Angulation | Counter Rotation | Lower Arch | Inclination | Angulation | Counter Rotation |
|---|---|---|---|---|---|---|---|
| Central | +7° | +4° | 0 | Central | -6° | +1.5° | 0 |
| Lateral | +4° | +8° | 0 | Lateral | -6° | +1.5° | 0 |
| Cuspid | 7° | +8° | 0 | Cuspid | -11° | 3° | 0 |
| Cuspid | -7° | +10° | 2M | Cuspid | -11° | 5° | 2M |
| 1st Bicuspid | -7° | +2 | 0 | 1st Bicuspid | -17° | 2° | 0 |
| 1st Bicuspid | -7° | +4° | 2M | 1st Bicuspid | -17° | 4° | 2M |
| 2nd Bicuspid | -7° | +2 | 0 | 2nd Bicuspid | -22° | 2° | 0 |
| 2nd Bicuspid | -7° | 0° | 2D | 2nd Bicuspid | -22° | 0 | 2D |
Prescription in Roth technique.
| Upper Arch | Inclination | Angulation | Off-set | Lower Arch | Inclination | Angulation | Off-set |
|---|---|---|---|---|---|---|---|
| Central | 12° | 5° | 0° | Central | 0° | 0° | 0° |
| Lateral | 8° | 9° | 0° | Lateral | 0° | 0° | 0° |
| Cuspid | 0 | 11° | 0° | Cuspid | -11° | 5° | 0° |
| 1st Bicuspid | -7° | 0° | 0° | 1st Bicuspid | -17° | 0° | 0° |
| 2nd Bicuspid | -7° | 0° | 0° | 2nd Bicuspid | -22° | 0° | 0° |
Prescription in MBT technique.
| Upper Arch | Inclination | Angulation | Lower Arch | Inclination | Angulation |
|---|---|---|---|---|---|
| Central | +17° | +4° | Central | -6° | 0 |
| Lateral | +10° | +8° | Lateral | -6° | 0 |
| Cuspid | 7°/-7° | +8° | Cuspid | 6°/-6° | 3° |
| Cuspid | 0 | +8° | Cuspid | 0 | 3° |
| 1st Bicuspid | -7° | 0 | 1st Bicuspid | -12° | 2° |
| 2nd Bicuspid | -7° | 0 | 2nd Bicuspid | -17° | 2° |
The Concept of Variable Torque Prescription
The evolution of orthodontics with self-ligating brackets pave the way for orthodontist not only to a new biomechanics but also to a new concept of treatment planning: each malocclusion present peculiar characteristics in the inclination of posterior and anterior teeth in both arches so the information inside the bracket must be chosen considering the occlusal features before the treatment and the biomechanics to achieve the final result. The different characteristics that could be found inside a malocclusion lead to develop of different prescription of torque for the upper and lower six anterior teeth: the aim of this individualization is to achieve a better functional and aesthetic outcome, with less risk of orthodontic relapse. The beginning of interest on the torque values has born from the clinical evaluation of the loss of torque with passive self-ligating brackets: the correct torque value could be achieved reducing and/or adding the degrees of torque inside the prescription [24]. Nowadays, the authors that most emphasized the VPO concept are A. Sondhi and D. Damon: they suggest that the correct torque value has to be selected considering the patient malocclusion and periodontal characteristics, the inter- and intra-arch variables and the class correction biomechanics [25, 26]. All the possible clinical combinations lead to high-, standard and low- torque prescriptions for upper and lower anterior teeth: the high torque values are taken by Hilgers, the standard torque correspond to the MBT values, whereas the low torque values are the Roth values (Fig. 1).
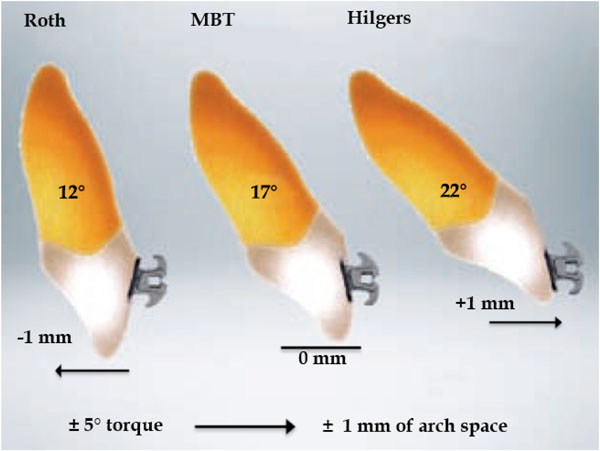
For every 5° of anterior torque, obtained by placing the bracket 1 mm higher or lower with respect to the center of the clinical crown, the space in the arch is modified by 1 mm and the prescription is changed.
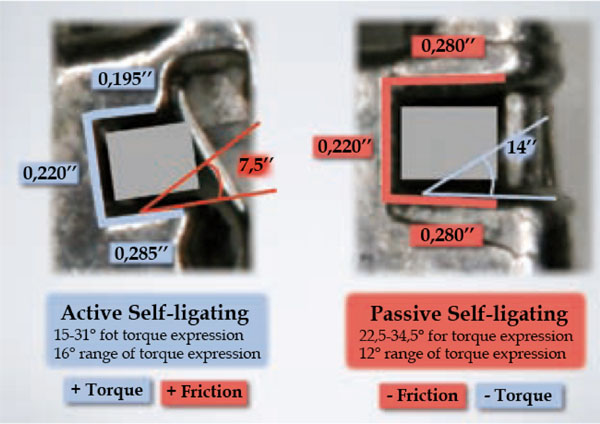
Side view of the two self-ligating braces. Left: active selfligating braces, with the interactive wall. Right: passive selfligating braces, with the typical 4-wall slot. The difference between the dimensions of the slot and their “engagement angle” or “torsional clearance” is according to Badawi et al., [3].
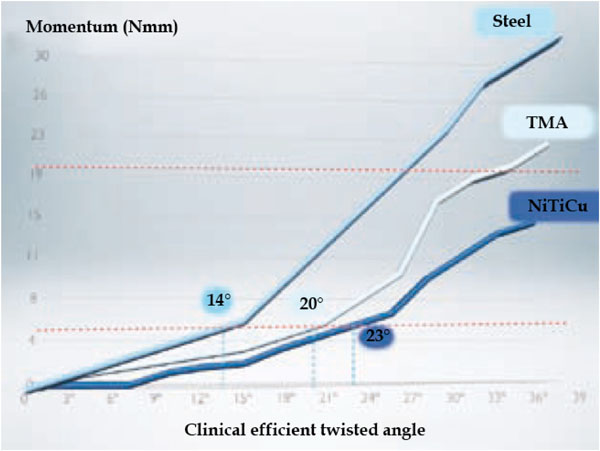
Graph comparing the torque expression capacities of different alloys for the orthodontic arch. For a section of 0.019" x 0.025" in stainless steel, with its higher hardness and stiffness, the torque is expressed more effectively.
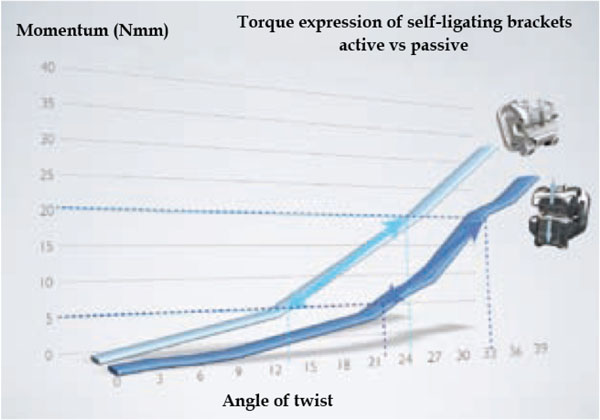
Graph comparing the torque expression capacities of active and passive self-ligating brackets. According to Badawi et al. [3], active self-ligating brackets express torque more effectively and efficiently than passive ones. Self-ligating brackets start to generate clinically effective momentum between 15° and 31°, compared to passive brackets that need higher torsion to generate the same momentum (between 22.5° and 34.5°).
DISCUSSION
Traditionally, the torque is achieved when the rectangular wire is full engaged to the slot of the bracket: the full-size wire is the last one of the archwire sequence and it must allow the sliding movement of the dentition and the torque control at the same time. For many authors the optimal bracket-archwire relationship is represented by a 0.022”x 0.028” slot and the 0.019”x 0.025” stainless steel wire [5, 11, 27]: this combination does not permit a full-engagement of the arch wire in the slot because only 10% of the wire is used. This aspect opens a discussion about the discrepancy between the information provided by the companies and the real wire-bracket interaction, especially because during alignment and levelling the discrepancies are less evident [28-31]. In this situation the orthodontist needs a more clear view about the variables concerning the torque expression and, on this topic, some keys of comprehension are fundamental: the different effectiveness in torque expression of the different alloys, the effect of bracket position and dental morphology on torque expression, the influence of bracket design on its capacity to read the torque (friction and bracket/wire interaction).
The Archwire Alloy
The archwire alloy is fundamental for the expression of the torque because it is the stiffness of the material that determines the complete reading of the bracket information: in fact, at the same thickness values, NiTi and the TMA alloys presented a lower stiffness, so they present a lower torque expression then the Stainless steel alloy [32] (Fig. 2). The aspect that is considered critical in the torque achievement with the TMA and NiTi alloy is represented by the twist angle produced by the wire in the bracket: Archambault referred that, if the angle is lower then 12° there are no differences between the wires [33]. With this assumption, using the variable prescription will provide the correct torque because the loss of torque determined by the wire could be compensated by the information inside the bracket.
The Bracket Positioning
The force that determines the torque is correctly expressed when the force is applied in the center of the clinical crown: a different positioning, as demonstrated by Meyer and Mietheke, could determine a variation of the torsion angle by 10° to 15° [6, 31] Fig. (3). The bracket positioning could also be affected by the dental morphology: a divergency between the longitudinal axis of the crown and of the root could change the effect of the same bracket [34]. If on the one hand the orthodontists are used to correct the bracket’s position by correctly debonding and rebonding the bracket, on the other hand, the debonding procedures present their unfavorable effects [35]: the change of bracket position on the vertical aspect, if the verticality is properly controlled, could be a good clinical option to reduce/add torque, especially when the VPO is applied.
The Brackets Design
The brackets are built in different materials and present more then one design: Morina compaired the ability of conventional brackets versus self-ligating brackets to generate the moment angle able to produce the torque. The ceramic brackets showed the best function in torque maintenance, followed by conventional metal brackets, then self-ligating active brackets and self-ligating passive brackets: in agreement with other researches, this study also revealed that the best range of moment of forces that generates the torque is between the 5 and 20 Nmm [36-38]. The authors detected that, with active self-ligating brackets the angle formed between the bracket and the wire had to range between 15° and 31° to achieve the optimal torque, with passive self-ligating brackets the same values of torque were achieved with angles between 22.5° and 34.5°: these results agree with previous literature such as Gymrek’s and Harzer’s studies [38, 39] Fig. (4). The conclusion on most of these studies are clinically useful up to a certain point because most of them are in vitro studies, so the in vivo studies show lower levels of moments: the most difficult part under a clinical point of view is represented by the engagement of the archwire when the malocclusion is severe, and torque is determined not only by the momentum angle, but is also influenced by the friction due to dental malposition.
CONCLUSION
In orthodontics the torque control is fundamental under a clinical point of view. Nowadays, many studies underline the importance of considering the factors that affect the torque expression and management, such as the patient’s malocclusion and general characteristics, the bracket’s design, the wire’s components and sequence, the bracket positioning and the treatment biomechanics. The VPO is a good tool for the orthodontist to manage the torque since The beginning of treatment, because many of the factors affecting are considered. Looking forward, new comparative studies on the effectiveness of the treatment planning using the VPO versus the conventional treatment planning are required.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.
AUTHORS’ CONTRIBUTIONS
ML, EA, AMR contributed to the concept and design of the study, the analysis and interpretation of the data and drafted the manuscript. AM, GM, MTD and MC were involved in the interpretation of the data and contributed to the revision of the drafted manuscript. All authors read and approved the final manuscript.

