All published articles of this journal are available on ScienceDirect.

Root Resorption a 6-Year Follow-up Case Report
Authors Info & Affiliations
Abstract
This paper describes the clinical course of a pediatric patient developing cervical external root resorption (CERR). An 11-year old male patient had sustained dental trauma and was diagnosed with crown fracture affecting the incisal and middle thirds of the maxillary right permanent central incisor and the maxillary right permanent lateral incisor with pulp exposure and CERR after 24 months. Diagnosis and treatment of CERR are a challenge for dental practitioners. In this case, preservation of natural dentition is shown as a successful treatment in a 6-year follow-up.
INTRODUCTION
Cervical external root resorption (CERR) is a condition frequently associated with trauma [1, 2]. Other etiological factors include intracoronal bleaching, ectopic eruption, bruxism, and idiopathic conditions [1, 3, 4]. CERR starts below the epithelial junction, and the clinical features of visible lesions may vary from a small defect at the gingival margin to a pink coronal discoloration of the tooth crown, resulting in cavitation of the overlaying enamel. Depending on the severity and location of the defect, diagnosis and treatment may become a challenge [1, 2].
Physical trauma, in turn, is very frequent among children and adolescents, with a strong impact on the quality of life. The prevalence and severity of traumatic injuries reach their peak between 8 and 15 years of age, mainly in males [1-4]. Ectopic eruption may cause CERR and in long-term follow-up teeth with this condition might show no clinically relevant symptoms [5]. In the present report, we describe the case of a young male patient with traumatized permanent maxillary central and lateral incisors who present an invasive CERR with successful treatment and follow-up.
CASE REPORT
Our patient was 11 years old and had sustained dental trauma at school, while practicing sports. He was diagnosed with crown fracture affecting the incisal and middle thirds of the permanent maxillary right central incisor and the permanent maxillary right lateral incisor, with pulp exposure; no changes in tooth positioning and no tooth mobility were observed.
Baseline periapical radiographic examination revealed that both injured teeth presented incomplete root formation and that the permanent maxillary right lateral incisor was in intimate contact with the permanent maxillary right canine (Fig. 1A, B). Pulp chambers, in booth teeth, were removed using a high-speed bur and a spoon excavator (pulpotomy). A small cotton pellet damp with formocresol was applied with pressure, and chambers were sealed with glass ionomer cement (Vitremer™ Luting Cement, 3M, St. Paul, USA). Tooth fragments were reattached using light-cured resin (Filtek™ Z350 Flowable Restorative shade A2, 3M, St. Paul, USA).
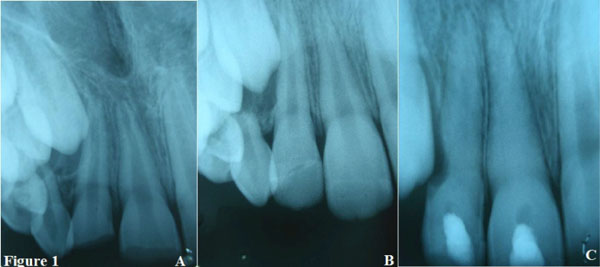
Baseline periapical radiograph (1A) periapical radiograph showing pulpotomy and reattachment of tooth fragments (1B) and root canals filled with a calcium hydroxide dressing at 24 months after the trauma (1C).

The cavity after surgical access at 24 months after the trauma.
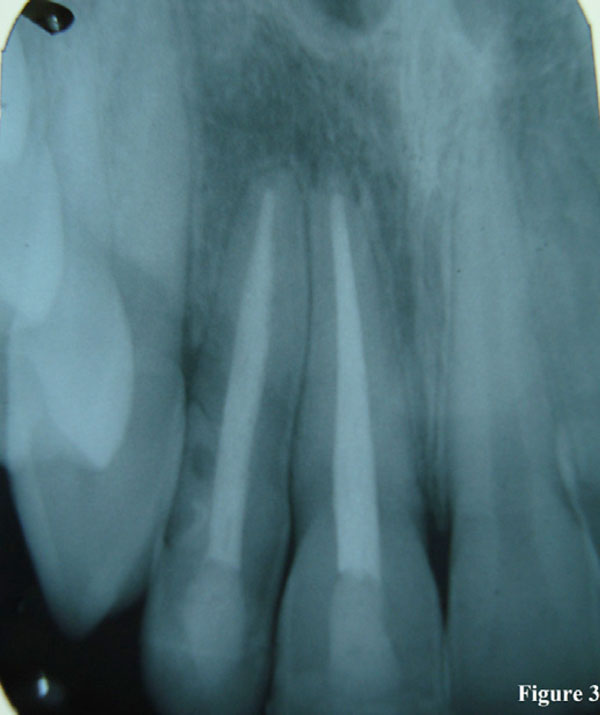
Six-year follow-up periapical radiograph.
After 24 months, radiographic examination revealed the presence of CERR on the permanent maxillary right lateral incisor (Fig. 1C).
Pulp sensibility test resulted negative on the permanent maxillary right central incisor. Endodontic treatment in booth teeth was conducted under rubber dam isolation. The tooth was surgically accessed to seal the cervical defect (Figs. 2, 3).
DISCUSSION
The etiology of external root resorption remains the object of extensive debate, and some causes are still unknown, posing difficult challenges to the establishment of clinical diagnosis in some cases [6-8].
Pulpotomy was chosen to treat our patient because it is considered as an adequate conservative indirect pulp treatment approach in trauma victims [2]. Age is an extremely important factor in the selection of any treatment approach for a vital pulp [9]. The pulpotomy allows further root development and to guarantee apical closure after the procedure, based on the presence of Hertwig’s epithelial root sheath [signaling the physiological development of the root]. The treatment plan here described is supported by Fuks et al. [10].
When successful, this therapy allows long-term completion of apexification and the formation of dentin around canal walls [2]. Rubber dam isolation is a routine during endodontic treatment: it provides better visualization, adequate isolation to conduct restorative procedures, and particularly, prevents root canal contamination. In our case, we used a rubber dam to guarantee absence of contamination in the root canal [11, 12].
The baseline periapical radiograph does not show a close relationship of the upper canine eruption to mesial of the upper lateral. These findings can be observed in panoramic radiographs or computed tomography (CT). An orthodontic extrusion would be a good treatment option, causing occur stimulation of bone formation. Dental extrusion and panoramic radiograph or CT were not discussed in this case because the patient’s family did not have the conditions that pay for the orthodontic routine visits and complementary exams on other hand, the orthodontic extrusion of the upper lateral incisor could result in a faster resorption of this tooth, presented incomplete root formation, resulting in the lost of his incisors at such an important phase of growth and development.
At 6 years’ follow-up, the permanent maxillary right lateral incisor showed normal clinical and radiographic findings and no root fracture. Therefore, we infer that CERR in our patient was not caused by trauma or pulpotomy, but rather by ectopic eruption of the permanent maxillary right canine.
It is very important to maintain a regular clinical and radiographic follow-up of victims of dentoalveolar trauma and to control tooth eruption in this population, so as to prevent potential sequelae [2, 4]. Our case had a poor prognosis, but satisfactory long-term results were obtained as a result of a strict follow-up regimen along 6 years: 1) the patient did not lose his incisors at such an important phase of growth and development; 2) early tooth loss was avoided, as well as the accompanying esthetic and functional complaints (the wear of adjacent teeth for the fabrication and placement of a fixed prosthetic crown would be extremely invasive); and 3) we managed to preserve the patient’s natural teeth, which should always be the preferred approach in clinical practice.
It underscores the importance of keeping a regular follow-up regimen and of adopting an interdisciplinary approach (pedodontics-endodontics-periodontics- restorative dentistry) in the treatment of CERR.
CONCLUSION
Ectopic eruption of the right maxillary canine should have caused CERR in our patient. This conclusion was drawn based on the follow-up data. In spite of a poor prognosis, satisfactory long-term results were obtained and potential sequelae were avoided as a result of strict 6-year follow-up regimen.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

