All published articles of this journal are available on ScienceDirect.

The Use of Glass-fibers Ribbon and Composite for Prosthetic Restoration of Missing Primary Teeth-Laboratory and Clinical Research
Abstract
Very few modalities can be used for restoring missing primary anterior teeth, although the impact of missing anterior teeth during early childhood can be harmful. In the permanent dentition the use of glass-fibers ribbon and composite materials are frequently used for restoring missing teeth with no or minimal preparation. The purpose of this study was to examine the possibility to use the glass-fibers ribbon (ever-Stick from GC Corporation, Japan) together with esthetic composite materials (G-aenial A1 from GC Corporation, Japan) for restoring anterior primary teeth and to determine the best methodology and bonding system to be used.
The effect of etching time was analyzed using 20-80 sec on primary buccal enamel with SEM and the results showed that at least 60 second is necessary in order to remove the prismless layer and to affect the prismatic layer similar (as observed by SEM) to the 20 sec etching time on permanent enamel. Three bonding systems (SE Bond by Kurary, Japan, Scotchbond Universal by 3M/ESPE, Germany and G-aenial bond by GC Company, Japan) were compared for bonding the glass-fibers ribbon to the primary enamel and microtensile strength analyses were performed. Mean tensile strength ranged from 10.9 to 13 MPa with no statistically significant differences between all three systems.
Based on the laboratory results it can be concluded that the glass-fibers ribbon together with the composite material can be used clinically to restore missing primary teeth for esthetic and functional reasons. Two clinical cases are presented that show favorable results.
INTRODUCTION
Missing primary teeth due to extraction because of carious attack or trauma and avulsion may have significant functional and psychological impact on young children. Esthetics of the dentofacial area contributes to the total attractiveness of the face and acceptance of children by their peers and adults [1]. Well being of young children may be affected by the lack of long lasting restorative options for missing primary teeth. The importance of restoring grossly carious maxillary primary incisors was perceived by parents of young children [2], and the esthetic appearance and longevity of the restorative material plays an important role in its' acceptance for both dentists and parents. [2-5] For grossly carious maxillary primary incisors several esthetic restoration are available, from bonded resin composite strip crowns [6] to pre-veneered stainless steel crowns [7] and recently with polyethylene fibers as posts under composite strip crowns or as base for a reinforced prosthesis to replace missing incisors [8, 9].
The relatively new generation of fiber-reinforced composites is commonly used in permanent dentition to splint periodontally compromised teeth [10] or to restore missing teeth [11] due to their high bond strength to enamel after standard acid-etch and adhesive techniques [12]. The main problem in using this technique for restoring primary missing teeth is the differences between the enamel of permanent versus primary dentition. The enamel thickness of permanent teeth is between 1-2 mm while in primary dentition the thickness is between 0.5-1 mm. The enamel of both primary and permanent teeth is covered by a prismless layer [13, 14], but while in the permanent dentition the thickness of this layer is less than 5 microns, in the primary dentition it can reach as high as 45 microns [15]. The uni-directional orientation of crystals and their relative dense arrangement in prismless enamel results in relatively uniform dissolution and creation of limited random porosity. The primary prismatic enamel also showed a lower degree of microcrystal arrangement due to less mineralization. The acid etching procedure using 15-20 seconds etching time removes about 10 microns of the enamel surface and creates a porous layer ranging from 5-50 microns deep for the "resin tags" mechanical retention of composites. In permanent enamel this method removes the prismless layer and exposes the prismatic layer. In primary enamel etching time of even one minute showed an amorphous substance and no evidence of prisms [16]. An acceptable etch-pattern was obtained with three minutes acid treatment after mechanical grinding of the enamel [17]. More recent research looked at shear bond strengths of orthodontic brackets to permanent and primary enamel. No significant differences were found between etching system, but the results were significantly lower than the results for permanent teeth [18, 19]. The only possibility to restore missing primary teeth has to be based on attachment of the prosthetic restoration to enamel using the etch and bond system similar to the method used for permanent teeth.
The aim of this study was: a. to analyze in vitro the effect of different etching time on enamel of primary molars. b. to measure the shear bond strength of adhesive bonded fiber-reinforced composite to etched primary enamel using three different bonding systems. c. to use in vivo the fiber-reinforced composite for prosthetic restoration of missing primary teeth.
MATERIALS AND METHODOLOGY
- In vitro estimation of etching time on primary molars outer surface. Four naturally exfoliated second primary molars were used. The teeth were sectioned mesio-distally using a diamond bur under copious amount of water. The buccal and lingual surfaces were cleaned using a rotatory brush. On each surface, each half was etched with a 37% phosphoric etch solution (Scotchbond Universal etchant by 3M/ESPE AG, Seefeld, Germany, lot 464502) for a different time: 20, 40, 60 and 80 sec, so that on the same tooth four different etching time were used. The enamel surfaces were rinsed with tap water for 10 second and dried with air. The teeth were coated with gold and examined with SEM (JEOL 5500, JEOL ltd, UK) at high magnifications (X500, X1000), in order to determine the effect of etching time on enamel. As controls, buccal surfaces of two upper premolars were etched for 20 sec, rinsed, dried and gold coated before mounted into the SEM and examined.
- Determination of microtensile bond strength of fiber-reinforced composite (ever-Stick, GC Company, Japan, lot 120020130611) to primary enamel using three different bonding systems. Fifteen naturally exfoliated primary upper second molars were sectioned mesio-distally using a diamond bur under copious amount of water. Each half was embedded in epoxy resin so that the buccal or lingual surfaces were exposed. Each surface was etched with a 37% phosphoric etch solution (Scotchbond Universal etchant by 3M/ESPE) for 60 seconds, rinsed for 10 seconds and dried. On each surface two 3 mm high polycarbonate cylinders with a base area of 10 mm2 were attached (Fig. 1). On each surface a similar bonding system was applied according to manufacturer instructions: a. Scotchbond universal (3M/ESPE, AG, Seefeld, Germany, lot 459407), b. G-aenial Bond (GC Co Tokio, Japan, lot 1304151) and c. Clearfil SE bond (Kurary Noritake Dental Inc. Okayama, Japan, primer lot 2U0021 and bond lot 2T0037). A round piece of perio fiber-reinforced ribbon was activated according to manufacturer instructions with Stick-Resin (GC Co Tokio, Japan, lot 1203211) and bonded to the enamel surface. The polycarbonate cylinder was placed on top of it and filled with 1 mm of flowable composite (MI Fil A2 by GC Co Tokio, Japan lot 1110132) and 2 mm of conventional composite (G-aenial A2 by GC Co Tokyo, Japan lot 1205212). Each layer was cured with a light cure machine (Elipar S10 by 3M/ESPE, Seefeld Germany) for 20 sec. After curing the polycarbonate cylinder was removed and the specimens were tested using a microtensile test apparatus (LR30k Lloyd Instruments, USA). Microtensile bond strength was expressed in MPa by dividing the tensile force (N) at fracture by the bonded surface area (10 mm2). The debonded surfaces were analyzed for failure determination (adhesive or cohesive). The data was transferred to the computer and SPSS statistical software was used to analyze between different bonding techniques.
 Fig. (1).
Fig. (1).The cylinders filled with composite material attached to the glass-fibers ribbon bonded to primary molars enamel surface after embedding.
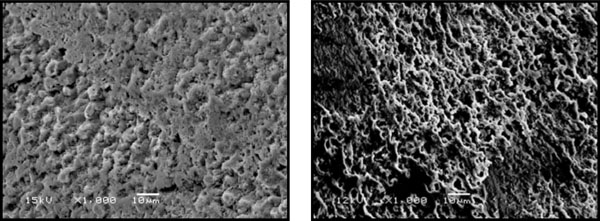 Fig. (2).
Fig. (2).The effect of 20 sec etching on the enamel of 2 permanent premolars as observed by SEM at x1000 magnification. Note on the left the removal of inter-prismatic layer (type 1) and on the right the removal of the intra-prismatic layer (type 2).
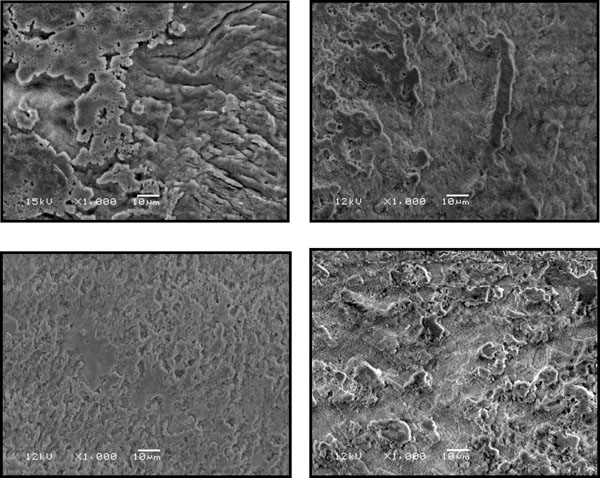 Fig. (3).
Fig. (3).The effect of 20 sec etching on enamel of 4 primary molars as observed by SEM at x1000 magnification. Note that the acid affected the aprismatic layer only on all teeth.
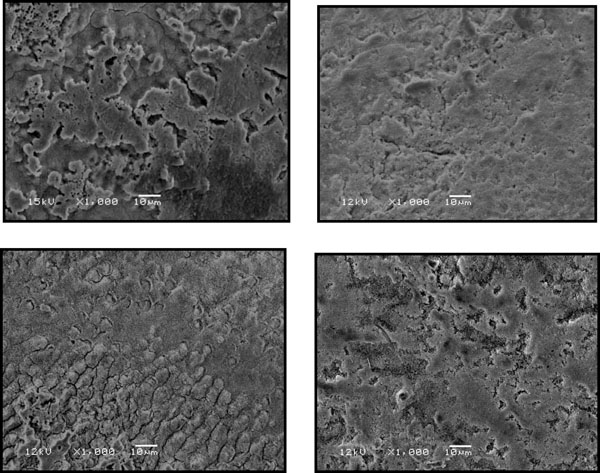 Fig. (4).
Fig. (4).The effect of 40 sec etching on enamel of 4 primary molars as observed by SEM at x1000 magnification. Note that on 3 teeth the acid affected the aprismatic layer and only on 1 tooth the acid exposed the prismatic layer (lower left).
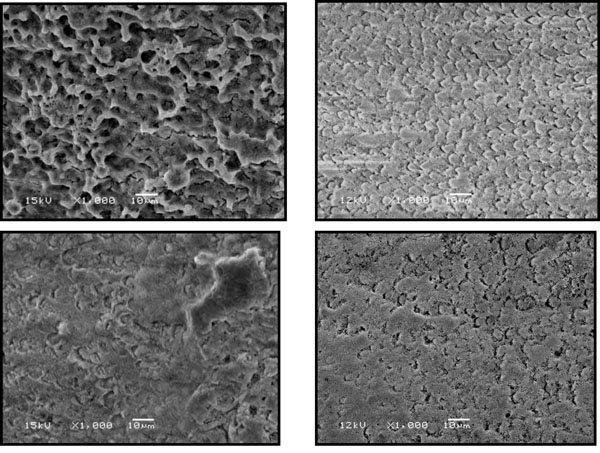 Fig. (5).
Fig. (5).The effect of 60 sec etching on enamel of 4 primary molars as observed by SEM at x1000 magnification. Note that on 3 teeth the acid exposed the prism layer and affected the inter-prismatic layer.
 Fig. (6).
Fig. (6).The effect of 80 sec etching on enamel of 4 primary molars observed by SEM at x1000 magnification. Note that the acid exposed the prismatic layer on 3 teeth, similar to the effect of 60 seconds etching.
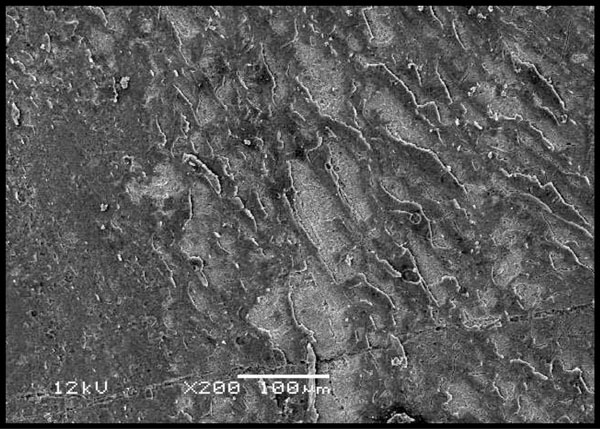 Fig. (7).
Fig. (7).Adhesive failure of G-aenial bond as observed under SEM at x200 magnification. Note the remnants of the bonding agent on the enamel.
 Fig. (8).
Fig. (8).Cohesive failure with Scotchbond as observed under SEM at x100 magnification. Note the glass fibers.
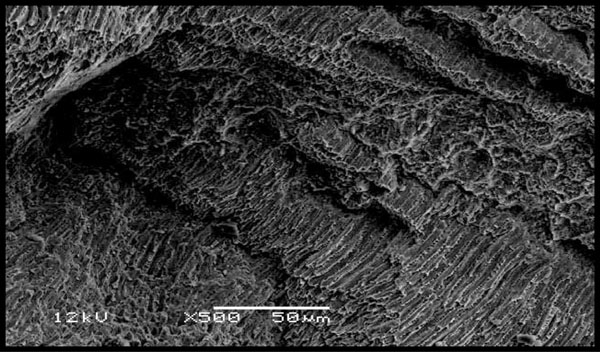 Fig. (9).
Fig. (9).Enamel fracture as observed under SEM at x500 magnification. Note the enamel prisms.
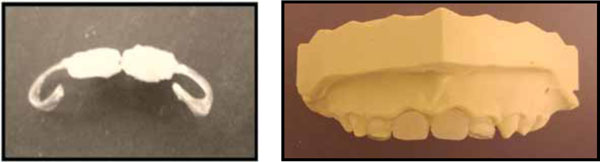 Fig. (10).
Fig. (10).The bridge frame and the restored teeth on the mold.
 Fig. (11).
Fig. (11).MI with the glass-fibers based bridge, before and after bonding with G-aenial Bond.
 Fig. (12).
Fig. (12).IM, severe ECC before treatment. Note the functional Class III occlusion.
 Fig. (13).
Fig. (13).The glass-fibers bridge on the mold and in the mouth after bonding. Note the class I occlusion reconstructed. Teeth #51-53 were restored using composite coverage.
 Fig. (14).
Fig. (14).Six months follow up.
 Fig. (15).
Fig. (15).The smiling child at follow-up meeting.
RESULTS
The effect of etching on primary versus permanent teeth (controls):
Fig. (2) shows the effect of 20 seconds etching on 2 permanent premolars used as controls. On the left the etching caused removal of interprismatic area (type 1), and on the right the etching caused microporous surface due to removal of the prisms (type 2).
Fig. (3-6) shows the effect of 20, 40, 60 and 80 seconds etching on four primary molar teeth. After 20 seconds the etching solution affected only the aprismatic layer. After 40 seconds the etching solution affected the aprismatic layer on three primary molars and on only one molar the prisms were exposed. After 60 seconds on three primary molars the prisms were exposed and after 80 seconds no significant difference was observed when compared to 60 seconds. Based on these observations an etching time of 60 seconds was used to prepare the enamel for glass-fibers ribbon attachment.
Table 1 shows the results of the microtensile strength test of the glass-fibers ribbon (ever-Stick Perio) with the three bonding systems. The mean results for SE bond were the highest (13.04 MPa) when compared to G-aenial and Scotchbond (10.92 and 10.90 MPa respectively), but the differences were not significant statistically (P=0.188). The minimal microtensile strength for all bonding systems were over 6 MPa and the highest results were observed for SE bond and G-aenial bond (>20 MPa). The enamel surfaces were examined for determination of the failure cause, adhesive or cohesive, and samples were observed with SEM after gold coating. Figs. (7 and 8) shows the differences between adhesive and cohesive failures as observed with SEM. The majority of the failures (82%) were cohesive and on the two surfaces with the highest microtensile results, fractures of enamel surfaces were observed (Fig. 9).
The results of microtensile strength of glass-fibers ribbon (Stick-tech) for three bonding systems.
| Brand | N | Mean MPa | SD | Min | Max |
|---|---|---|---|---|---|
| G-aenial bond (GC) | 16 | 10.92 | 4.2 | 6.1 | 20.4 |
| SE bond (Kurary) | 18 | 13.04 | 4.5 | 6.8 | 22.6 |
| Scotchbond (3M/ESPE) | 17 | 10.90 | 2.9 | 6.3 | 16.5 |
Clinical cases:
MI, a 3Y6M old boy was treated under general anesthesia due to severe ECC (Early Childhood Caries) and lack of cooperation. The upper primary centrals were extracted and an impression was taken. On the mold a restorative bridge was fabricated using the Perio glass-fibers ribbon (ever-Stick, GC Co, Japan) as base, treated using the Stick-Resin (GC Co Tokio, Japan, lot 1203211) and the missing teeth were restored using A1 G-aenial flowable composite (G-aenial flo, GC Co, Tokyo, Japan lot 1102091) and A1 restorative composite material (Fig. 10). Two weeks after the extractions the bridge was re-treated with Stick-Resin and bonded to teeth #52,62 after 60 seconds etching, rinsing for 10 seconds and drying, using the G-eanial bond according to manufacturer instructions and light cured for 60 seconds (Fig. 11). The glass fibers base on teeth #52,62 was coated with flowable composite.
IM, a 4 years old boy was treated under GA due to severe ECC (Fig. 12). An impression was taken prior to treatment and a glass-fibers based bridge was fabricated. During the treatment, tooth #62 was extracted and the fabricated bridge was bonded similar to the previous case to teeth #61,63 (Fig. 13). Teeth #51,52,53 were restored using the pediatric strip crown forms (3M/ESPE) and A1 restorative composite material after 60 seconds etching and bonding with G-aenial bond (GC Company, Japan).
DISCUSSION
Restoration of missing anterior teeth in the permanent dentition is a very common procedure in dentistry [20, 21]. In primary dentition, the impact of missing anterior teeth may affect physical and social development, and yet only a few papers describe clinical cases of restoring these teeth [8-9]. The aim of this study was to determine the best procedure for direct or indirect restoration of missing primary teeth using glass-fibers ribbons and composite materials. The retention of the restoration is based on the etch and bond technique, but the differences between primary and permanent enamel have to be taken into consideration for the procedure. The SEM analyses of the primary enamel showed that it takes at least 60 sec to remove the prismless layer and to reach the prismatic layer for etching, similar to previous publications [16-17]. When using 60 seconds etching the tensile strength of the glass-fibers to primary enamel was between 10.9 and 13 MPa for all three bonding systems and the differences were with no statistical significance. These results are greater than what is believed to be clinically sufficient strength of 6-8 MPa for bonding to primary teeth outer enamel [18, 19]. The most of the failures were cohesive, in the glass-fibers ribbon, demonstrating that the attachment between the three bonding systems and the enamel was stronger than the microtensile strength results. The clinical cases showed that the use of the glass-fibers ribbon (everStick from GC corporation) together with esthetic composite (G-aenial A1 by GC corporation) can be a very promising method to restore missing primary teeth with minimal clinical intervention. The smile of the children after the restoration of the upper front teeth (Fig. 15) showed that decayed or missing teeth have a very negative impact on their well being and acceptance in their society.
CONCLUSION
- The effect of etching on the primary outer enamel is different than that of permanent enamel. Due to the thick prism-less layer of primary enamel, the etching time should be 60 seconds in order to reach the prismatic layer and affect the inter-prismatic sheath.
- The tensile strength of the perio glass-fibers (ever-Stick, GC Company, Japan), bonded with 3 different bonding systems, to primary enamel was between 10.9 to 13 MPa. The differences between the bonding systems were not significant statistically.
- Using the 60 seconds etching time, G-aenial bond (GC Company, Japan), perio glass-fibers ribons (stick-Tech, GC Company, Japan) and A1 resin composite material, a prosthetic bridge was performed and cemented in two cases (3.5 and 4 years old boys) of missing upper primary incisors. Six months follow-up showed very promising results, both esthetically and functionally (Fig. 14).
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
None declared.

