All published articles of this journal are available on ScienceDirect.

Experimental Study on Strength Evaluation Applied for Teeth Extraction: An In Vivo Study
Authors Info & Affiliations
Abstract
Purpose:
The aim of this work was to analyse all the applied movements when extracting healthy upper and lower jaw premolars for orthodontic purposes. The authors wanted to demonstrate that the different bone densities of the mandible and maxilla are not a significant parameter when related to the extraction force applied. The buccal and palatal rocking movements, plus the twisting movements were also measured in this in-vivo study during premolar extraction for orthodontic purposes.
Methods:
The physical strains or forces transferred onto the teeth during extraction are the following three movements: gripping, twisting, and traction. A strain measurement gauge was attached onto an ordinary dentistry plier. The strain measurement gauge was constituted with an extensimetric washer with three 45º grids. The system operation was correlated to the variation of electrical resistance.
Results:
The variations of resistance (∆R) and all the different forces applied to the teeth (∆V) were recorded by a computerized system. Data results were processed through Microsoft Excel. The results underlined the stress distribution on the extracted teeth during gripping, twisting and flexion.
Conclusions:
The obtained data showed that the strength required to effect teeth extraction is not influenced by the quality of the bone but is instead influenced by the shape of the tooth’s root.
INTRODUCTION
Today, the evolution of scientific dental knowledge gives clinicians the opportunity to save a tooth affected by different pathologies such as deep caries, tooth pulp inflammation or periodontal diseases. The association between modern endodontic and conservative techniques have meant that results are more predictable, with long-term clinical success while avoiding tooth extraction. However, tooth extraction is still indicated for those teeth which are considered “hopeless”; for large destructive caries; teeth with high mobility, or extractions association with orthodontic treatment. In addition, tooth extraction may represent one of the first oral surgery acts that a young dentist will face at the beginning of his career [1-3].
Exodontia is the most common procedure performed in oral surgery and, as mentioned before, is often the first surgical procedure carried out by young dentists. Complications, unexpected clinical episodes in respect to regular operative procedures under normal circumstances, can increase morbidity [4, 5].
Even if tooth extraction complications are rare, their occurrence can create a prolonged treatment phase, often inducing discomfort in the patient as well as causing further problems for the clinician.
Prevention is the best way of avoiding future complications. Therefore, it is fundamental that the clinician is able to evaluate the whole spectrum of complications and their implications. Complications can be wide ranging: from common ones like dry sockets or root fractures to uncommon and serious ones like displacement of a root fragment into the maxillary sinus and its consequent oro-antral fistula [2, 5].
The instrumentation used to execute tooth extraction has been modified over time [4-6]. Modern pliers are specific in shape and length for each tooth. The pliers used for tooth extraction can be considered as the first type lever. Resistance is represented by the tooth while the power/force needed is contained within the operator’s hand strength [7].
Tooth extraction is a surgical act and several complications may arise directly connected to the operator’s actions. Fracture of the alveolar bone is the most frequent complication during tooth extraction. This situation is connected to too much force being transferred onto the tooth through the instrument. In addition, incorrect hand movements can increase the possibility of tooth apex fracture. Other complications can be classified in the pre or post operational phase. The breakage of basal bone or lower jaw dislocation, swelling, edema and bleeding are all complications related to the extraction procedure [8, 9].
Results have confirmed that the bone resilience is connected to the number of structural components and this parameter is influenced by subsequent bone tissue modification, such as after tooth extraction [10, 11].
Other research work has evaluated tooth extraction through the recording of the applied twisting movement and forces. It has been able to classify the rocking and twisting movements. The data result showed, for the rocking movement, a high value for canine tooth extraction and a low value for the incisor. Moreover, the different strength needed for the upper jaw compared to the lower jaw during canine extraction has been highlighted [6, 12-14].
The rocking movement in tooth extraction has also been studied in connection with the alveolar bone function and resistance. It has been emphasized that the strength applied in tooth extraction is directly connected to the functionality of the alveolar bone, the dimension of the periodontal lamina and the angle of the root divergence [4, 6, 13]. Therefore, an important connection between the extractive strength, and hard and soft tooth tissues has been underlined. For this reason, correct geometric-shaped pliers plays a fundamental role in tooth extraction. Pliers with the correct shape and size can simplify extraction movements by reducing the applied strength needed [2, 4-6, 9, 14].
In this study we want to analyse the problems of tooth extraction related to the force applied through the pliers. The quantification of the active forces used may be useful in avoiding future complications like alveolar bone or apex fractures. Careful attention to details, including a thorough case history and anamnesis of the patient, radiographs and blood investigations, are fundamental treatment steps for exodontia. Before approaching tooth extraction, clinicians should evaluate the tooth root form and shape by radiographic image and clinical investigation. Consequently, the choice of instrument and surgical movements can then be decided on, using all the information obtained.
MATERIALS AND METHODS
The aim of this work is to analyse the actual strength used by an operator during tooth extraction. High-tech gauges were applied onto dental pliers by a mechanical engineer in order to quantify the stress distribution of tooth extraction.
Three different phases of extraction have been classified and divided as follow:
- Gripping
- Rocking
- Twisting
127 young patients (aged 13 – 17 years old) were included in this study and 220 premolars teeth were extracted. All the selected patients were receiving orthodontic treatment at the Catania Policlinic Medical Surgical Specialties Department. The patients’ parents signed consent forms after receiving a thorough explanation about the experiment, clinical procedures and possible risks. Both the consent forms and the research protocol were reviewed and approved by the Human Subject Review Committee from the University of Catania, Italy.
The Orthodontist requested the first upper and lower premolars extraction to create space and to complete the orthodontic treatment. No extracted tooth was affected by periodontal inflammation or dental caries. The group of selected patients was similar in, height, weight and age, and especially with regards to tooth root length and form (analysed by dental panoramic radiographic investigation). All extractions were performed by the same surgeon.
Two dental premolar pliers, both for the upper and lower jaws, constituted the instrumental system. A mechanical screw-clamp system was applied onto each plier, near the part grasped by the operator. The clamp was used to lock the pliers in place when gripping the tooth. The angle obtained represents the crown size. (Figs. 1-4).
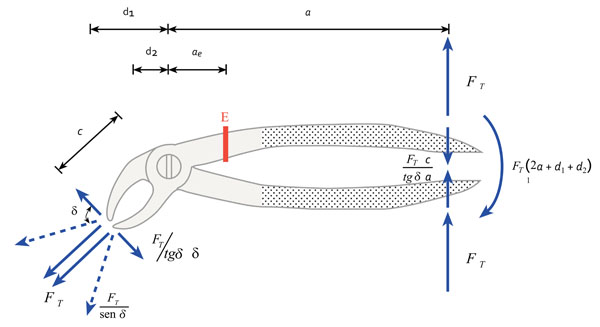
Scheme of the engineer formula for calculating force on mandibular premolar plier.
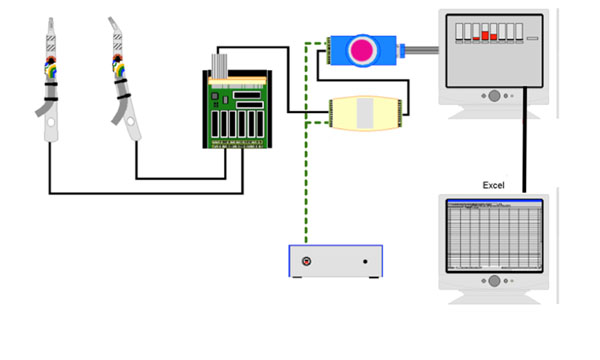
Scheme of the System of distribution data.
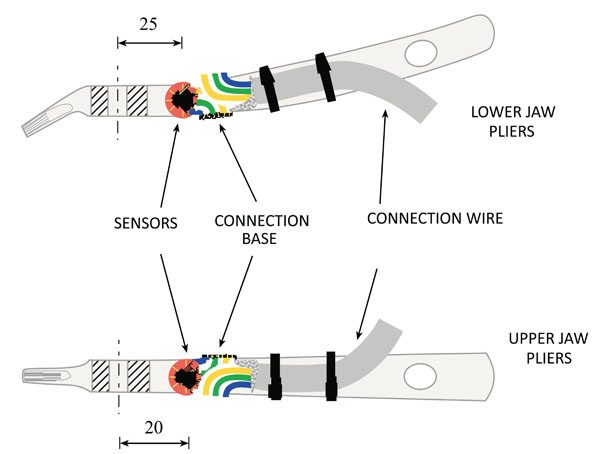
The strain gauge applied onto the pliers is an estensimetric washer with three grids in 45º types F L A 3-11. The estensimetric washer was positioned at the end of the pliers, precisely at 25mm from the centre of the pliers for the upper jaw, and at 20mm from the centre for of the lower jaw. The washer’s electrical contacts were protected by a silicone scabbard. The estensimetric washer was made up of three estensimetres (grids of wires). These grids were superimposed to form a geometric system. The axis of the pliers’ handle oriented one grid and it analysed the central component of the axial strength. The other grids were positioned with a 45º inclination during axis of the pliers’ handle. These grids analyse the transversal component of the force in action.
The tension of a material “σ”, can be defined as the strength applied on every mm² of material surface. The deformation of material “ε”, can be defined as the ratio between the variation of material length (under a strength action), and the original length of the same material [15].
The ratio between superficial tension “σ” and material deformation “ε” can be called “elastic form” and this value can be indicate with “E” (N/mm²) [15].
The system functionality is directly connected to the resistance ® variation of the washer grids. T The force used was converted into grid resistance ® during tooth extraction., the analyses can be quantified by a difference between the resistance values of a Wheatstone bridge [15-17].
The computerized system used was able to evaluate and quantify all tension variation in all the washer’s grids. This variation is called ∆V. We called “ε” the plier’s deformation in the washer localization and we identified “K” as a constant (related to the material quality of the washer). We obtained “∆V/V=Kε”.
The elastic module form is E= σ/ε. Therefore with these considerations, ∆V/V= σ/E * K where E represents the pliers’ elastic form and this is 210.000 N/mm².
THIS RELATIONSHIP IS TRUE FOR ALL GRID ANGLES
Numerous mathematical formulas between the hand and pliers and between the pliers and tooth in the three types of strength movements were created. Some graphics were used to simplify the measurements of the force used. The graphics produced a difference for the upper and lower jaw. The ordinate line represents the strength value in N; the abscissa line represents the tooth number according to international nomenclature.
Using these mathematical formulas, two types of tensions were obtained; the tension parallel to the handle, and the tension orthogonal one. The changing of the three grids’ structure into the two direction system represented the real value of the strength distribution.
SYMBOL DEFINITION
σ = Tension of a Material
ε = Material Deformation
E = Ratio between Material Deformation and Tension of Material = ε/σ
K = constant (dependent by material quality of washer).
∆V = Variation
N = Value for the strength measurement
RESULTS
The strength data was recorded with an electronic paper, elaborated in Microsoft Excel. Values of gripping, rocking, and twisting were classified and tabled (Fig. 5).
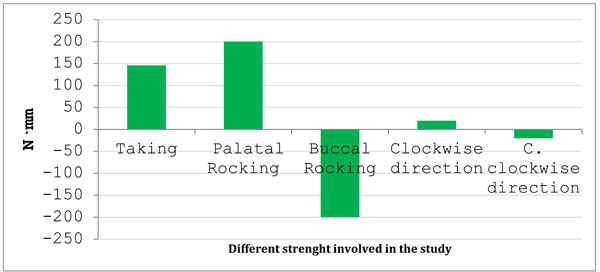
Evaluation of the total recorded data.
The average of the gripping values are 146 Nmm (9.81 Nmm about 1Kg). In particular, the average upper jaw gripping value is 165,6 Nmm, and the average lower jaw value is 126,4 Nmm. The strength in Nmm is noted on the ordinate lines, while the single value of the strength applied onto tooth (classified by international nomenclature) is noted in the abscissa lines (Figs. 6, 7).
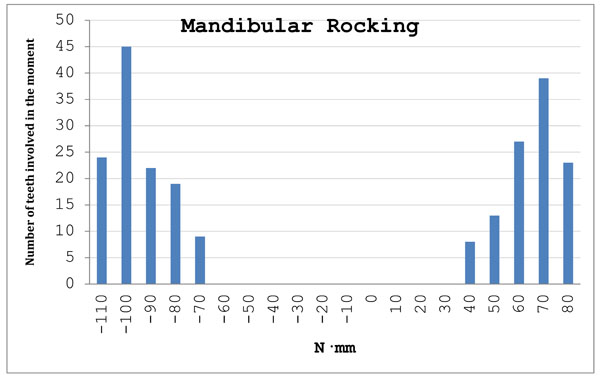
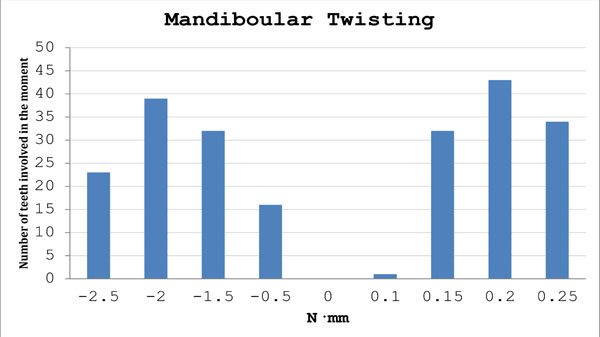
Mandibular rocking values recorded.
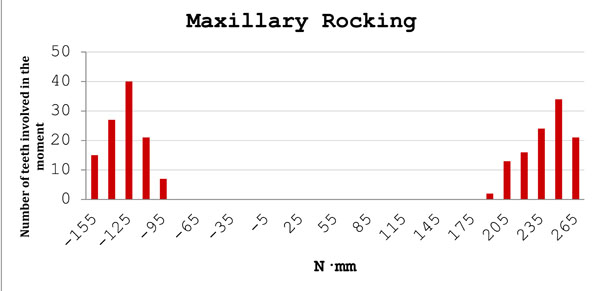
Maxillary rocking values recorded.
The rocking average was evaluated as follows: the rocking strength values were recorded within a range of -200 Nmm and + 200 Nmm and distinctly into a range of -153,5 Nmm and + 266,3 Nmm for the upper jaw, and into a range of -108,1 Nmm and + 74,1 Nmm for the lower jaw (Figs. 7, 8).
Mandibular twisting values recorded.
The twisting strength values were recorded within a range of -20 Nmm and + 20 Nmm and fell into a range of - 4,01 Nmm and + 13, 9 Nmm for the upper jaw and – 2,74 Nmm and + 0,22 Nmm for the lower jaw (Figs. 8, 9).
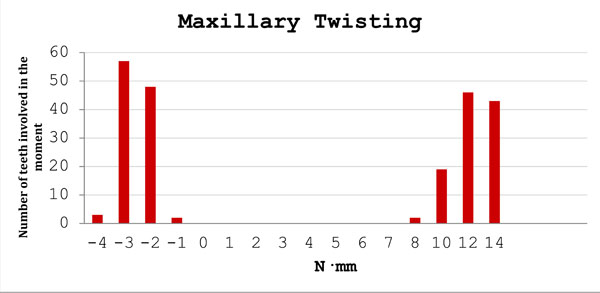
Maxillary twisting values recorded.
The negative values of rocking graphics indicated the movements in the palatal direction and the negative value of twisting graphics represented the movements in a counter clockwise direction.

Upper premolar plier used for the study.
Engineer mechanical model for strength evaluating.
DISCUSSION
The results obtained by this investigation were compared to the limited data found in the international literature. All results show that the strength used by the operator during tooth extraction may be the most important factor that influences this surgical act.
Several surgical details, including proper patient preparation, asepsis, and meticulous management of hard and soft tissue, haemostasis and adequate postoperative control, may help to reduce the rate of complications. Moreover, the controlled force used when applying surgical instruments is one of the most important factors to influence intraoperative complications [2, 4, 5, 7, 9, 12, 14].
In fact, the force used by the operator during tooth extraction has previously been studied [1-6]. In those studies, the strength applied in tooth extraction on the lower jaw was recorded and evaluated. The different force used for different tooth extraction was also analysed. Data has confirmed that the rocking movement was high in canine extraction and low in incisor extraction [1-4].
In another study, Lehtinen and Ojala analysed the strength used in extraction of upper jaw teeth and confirmed how the strength needed to extract superior or inferior canine teeth was not significantly different [2, 4].
All factors and phases of tooth extraction were investigated in other papers in which the rocking movements, the functionality of alveolar bone, the length of periodontal lamina and the angle of roots are significant parameters to be taken into account by clinicians before carrying out extractions. Data presented in the literature confirms the data obtained in this study. The difficulty in performing exodontia is higher when clinicians perform extraction of a tooth with two or more roots [1-4].
Results in other studies have demonstrated that when there is a 20% loss of alveolar bone, the value of the rocking movement is not the same as in the extraction of high quality bone. The average of the rocking force value was small when the loss of alveolar bone was higher than 20% of the total alveolar bone volume. The root inclination and angle was an investigated parameter that may influence tooth extraction. This condition justifies why molar extraction is more difficult than anterior single root incisor extraction. The data results have shown how the presence of a double root in the upper premolar tooth increases the strength needed for the extraction. Maxillary bone is a low-density structure compared to mandibular bone [17-22].
This study shows the result that the force applied by the operator during tooth extraction should be constant when applied to similar teeth, however several factors may influence the need to increase the strength used [2, 5, 18, 23, 24].
This study has also shown that the force required to have a controlled tooth extraction (expressed in N) is variable and specific to the operator: the active forces of twisting and rocking were always influenced by the resistance of the tooth. Twisting and rocking values were different for the upper and lower jaw due to the fact that the superior premolar gives much more resistance because of the presence of a double root, which sometimes merged together.
CONCLUSION
This study was carried out on teeth of young patients with a regular root formation and without any structural anomaly or shape alteration. The results of the study showed how the strength, needed for performing the first upper premolar extraction is 25 times higher than the lower jaw. This confirms that tooth extraction of multi-root teeth will result in a very difficult surgical operation. The rocking movement recorded high values of +199 Nmm while the twisting recorded maximum values of +8,69 Nmm. This data showed how the strength needed for double rooted teeth extraction is not proportional to the strength needed for single ones.
The complications of tooth extraction are connected to an incorrect force application [18, 25]. Several factors, such as strange tooth anomalies, large root angles or strange root forms seem to be present when exodontia complications occur. However, bone structure and density do not influence the strength value.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflicts of interest.
ACKNOWLEDGEMENTS
Authors would like to express their gratitude to Prof Veronica Gavin, B.Sc; T.E.F.L. for her precious contribute on giving English language proof to this manuscript.

