All published articles of this journal are available on ScienceDirect.

Long-term Caries Preventive Effects of a School-Based Fluoride Mouth Rinse Program in Adulthood
Abstract
The purpose of this study was to evaluate the long-term caries preventive effects of school-based fluoride mouth rinse (FMR) program in adults aged 20 years and older. 637 mothers aged from 20 to 39 years were surveyed. Clinical examinations were carried out for subjects to obtain data on dental caries prevalence when they visited local health centers to take their children for medical and dental check-ups at 1.5- or 3-years old. We also obtained information regarding the FMR program: the duration that the subjects participated between nursery school and junior high school. When analyzing data, subjects were divided into 4 groups: FMR from nursery to junior high school group (N-JH group, n=22), FMR limited to the elementary school group (El group, n=62), FMR no-experience group (n=545), and other subjects whose FMR experience is not clear (n=8). For evaluation of the FMR program effect, multiple regression analysis was used. As independent variable, the FMR program patterns were converted into dummy data, and mean DMFT was used as dependent variable. The results of multiple regression analysis between mean DMFT and FMR program patterns showed that the N-JH group and El group were negatively associated with the mean DMFT (ß=-0.20, p<0.001 for N-JH group and ß=-0.11, p=0.003 for El group).
The positive caries preventive effects of school-based FMR program from nursery school to junior high school can continue in adults aged 20 years and older.
INTRODUCTION
Dental caries often begin in childhood and increases with age. Pain and degradation of chewing function may result. A fluoride mouth rinse (FMR), which can prevent caries, is appropriate for use in schoolchildren. The effectiveness of FMR is primarily due to fluoride’s ability to enhance the remineralization process; thus low levels of fluoride make the crystal surface of the teeth resistant to acid attacks, which can lead to caries.
Many clinical studies [1-6] show that daily or weekly FMR result in reductions in DMF scores from about 50% when subjects start using the mouth rinse between 7 and 14 years of age, and when the study lasts from 2 to 3 years. Other studies [7, 8] suggest that topical fluoride is more effective on newly erupted teeth than on teeth that have been in the mouth for several years. Thus, theoretically, increased benefits should be seen with a regimen that is initiated at a younger age and continued thereafter.
Generally, in school-based FMR programs, participants start to rinse at age 4-years and continue until the age of 14-years in Japan. We should be able to determine the long-term effects for caries prevention using FMR program in adults who participated in the program during school years. However, few studies have been conducted [2, 8, 9].
The purpose of this study was to evaluate the long-term effects of a FMR in adults aged 20 years and older.
MATERIALS AND METHODS
Study Population and Measurements
We first enrolled all 35 cities, towns and villages in Niigata Prefecture, Japan. The municipalities in this study were selected using a stratified random sampling technique. After, we have divided the municipalities to cities (n=19), towns (n=11), and villages (n=5), we then randomly selected 2 cities, 2 towns, and 1 villages for this study using the STATATM software package (StataCorp., College Station, Texas, USA). The concentration of fluoride in the community water supply in all the municipalities was less than 0.1 ppm during this study.
In Japan, dental and medical health examinations for both 1.5- and 3-year-old children are implemented by the governments of municipalities under the law of child and maternal health and welfare. 637 mothers aged from 20 to 39 years who visited local health centers to take their children for medical and dental check-ups at 1.5- or 3-year-old were surveyed in 2004-2005. All subjects were Japanese. Participants were asked to sign consent forms regarding the protocol, which was approved by the Ethics Committee of the National Institute of Public Health.
Standardized dental examinations for the counting of decayed, missing, and filled permanent teeth were conducted according to World Health Organization criteria [10]. Interexaminer reliability for caries detection was assessed for the 2 examiners using 10 volunteer patients with 280 teeth. The Kappa value between examiners was 0.89 (p<0.001). We also obtained information regarding the FMR program, the duration that subjects participated between nursery school and junior high school from the database of Niigata prefecture supervised by the Niigata prefecture government. We divided the subjects into 4 groups: “FMR from nursery to junior high school group” (N_JH group, n=22); FMR limited in elementary school group (El group, n=62); FMR no-experience group (n=545); and other subjects whose FMR experience is not clear (n=8). Subjects in the N_JH group or El group received FMR with 500 ppm sodium fluoride solution daily for 2 years (from age 4 to 5), and received FMR with 2000 ppm sodium fluoride solution weekly for 9 years (from age 6 to 14). The FMR was performed under the supervision of school teachers.
Statistical Analysis
At first, we classified the subjects into two groups according to the age (20-29, 30-39). Means and standard deviations were used to characterize continuous variables. The percentage distribution or average of the difference levels of caries were compared among the N_JH group, the El group and the no-experience group. Statistical differences in DMFT among groups were tested by analysis of variance (ANOVA), and Scheffe multiple comparison test. In addition, the statistical difference in percentage of persons with DMFT (prevalence rate) in the N_JH group, the El group and the no-participating group was tested by Fisher’s exact test. We also used Fisher’s exact test to evaluate the difference in prevalence rate between N_JH group and the no-participating group or the El group and the no-participating group.
For evaluation of the FMR program effect, multiple regression analysis was used. As independent variables, the FMR program pattern was selected. First, we made the three variables such as N_JH group, the El group and the no-experience group. After using the no-experience group as reference, we inserted the data (yes or no) in each variable according to the subject’s FMR program pattern. Age was also selected as independent variable because there was a positive relationship between age and mean DMFT scores according to The Japanese National Survey [11]. In addition, as dependent variable, mean DMFT was used.
All calculations and statistical analyses were performed using the STATATM software package (StataCorp., College Station, Texas, USA).
RESULTS
Data on caries experience among 20- to 29-year-old subjects, based on mouth rinse groups (no-experience group, El group, and N_JH group) are shown in Table 1. All variables were lowest in the N_JH group. In particular, there was a statistically significant difference in overall prevalence rate (p=0.013, Fisher’s exact test), mean DMFT (p<0.001, ANOVA), mean DMFT_anterior (p=0.022, ANOVA), and mean DMFT_molar (p<0.001, ANOVA). Compared with the no-experience group, values for prevalence rate, mean DMFT, and mean DMFT_molar for the N_JH group were significant (p<0.05 by Fisher’s exact test for prevalence rate, p<0.001 by Scheffe multiple comparison test as the post-hoc procedure for mean DMFT, p<0.001 by Scheffe multiple comparison test as the post-hoc procedure for mean DMFT_molar). The same tendency was also recognized in a group of 30- to 39-year-olds (Table 2). There was a statistically significant difference in prevalence rate (p=0.015, Fisher’s exact test), mean DMFT (p<0.001, ANOVA), mean DMFT_anterior (p=0.046, ANOVA), and mean DMFT_molar (p<0.001, ANOVA). In addition, the values of prevalence rate, mean DMFT, and mean DMFT_molar at the N_JH group were significant compared with the no-experience group (p<0.05 by Fisher’s exact test, p<0.01 for mean DMFT, p<0.001 for mean DMFT_molar).
The Comparison in Prevalence Rate and Mean DMFT Among FMR Program Patterns (20-29 Years Old)
* p<0.05 by Fisher’s exact test for the no-experience group.
** p<0.001 by Scheffe multiple comparison test for the no-experience group as the post-hoc procedure.
§ Subjects who did not participated in FMR program.
$ Subjects who participated in FMR program during elementary school days.
¶ Subjects who participated in FMR program from nursery school to junior high school days.
$$ Percentage of persons with DMFT.
The Comparison in Prevalence Rate and Mean DMFT Among FMR Program Patterns (30-39 Years Old)
* p<0.05 by Fisher’s exact test for the no-experience group.
** p<0.01 by Scheffe multiple comparison test for the no-experience group as the post-hoc procedure.
*** p<0.001 by Scheffe multiple comparison test for the not participating group as the post-hoc procedure.
§ Subjects who did not participated in FMR program.
$ Subjects who participated in FMR program during elementary school days.
¶ Subjects who participated in FMR program from nursery school to junior high school days.
$$ Percentage of persons with DMFT.
Fig. (1) shows the percentage distribution of the subjects with DMFT in the three groups (no-experience group, El group, and N_JH group) for 20- to 29-year-olds. Statistical analysis showed a significant difference in the caries distribution of DMFT among the three groups (p=0.003, chi-square test).
Fig. (2) shows the percentage distribution of the subjects with DMFT in the three groups (no-experience group, El group, and N_JH group) for 30- to 39-year-olds. Statistical analysis showed a significant difference in the caries distribution of DMFT among the three groups (p<0.001, chi-square test). As seen in Figs. (1) and (2), there were a higher number of subjects with higher DMFT in the no-experience group.
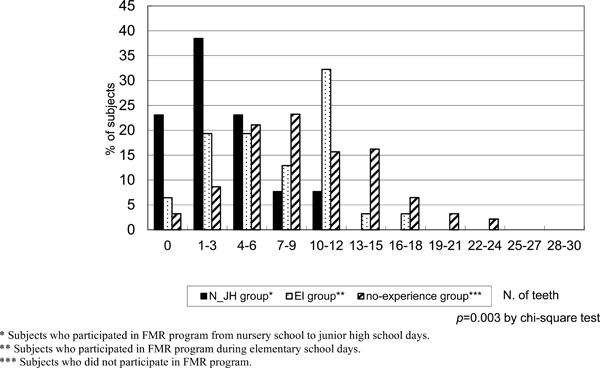
The percentage distribution of the subjects with DMFT in the three groups (20-29 years old).
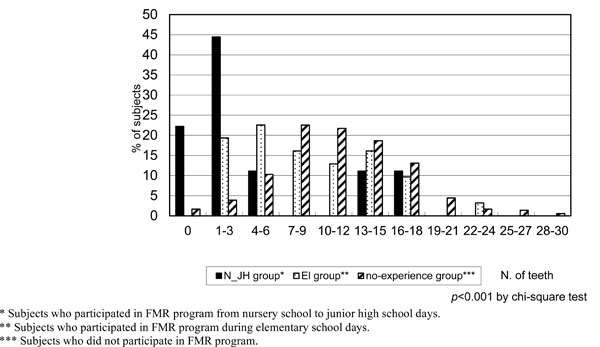
The percentage distribution of the subjects with DMFT in the three groups (30-39 years old).
Results of multiple regression analysis between mean DMFT and FMR program patterns are shown in Table 3. The N_JH group and El group were negatively associated with the mean DMFT (β=-0.20, p<0.001 for N_JH group, β=-0.11, p=0.003 for El group).
The Relationship Between FMR Program Pattern and Dental Caries Prevalence by Multiple Linear Regression Analysis
R2=0.107, p<0.001
* Subjects who participated in FMR program from nursery school to junior high school days.
** Subjects who participated in FMR program during elementary school days.
*** Subjects who did not participated in FMR program.
DISCUSSION
This study demonstrated that the mean DMFT in the no-experience group was about three times as high as that in the N_JH group. This shows that the favorable effects of FMR likely remain after discontinuation of rinsing. A low prevalence of dental caries in adults might prevent degradation of chewing function. Therefore, the most effective and realistic program for the prevention of permanent tooth caries consists of the use of a FMR beginning at 4 years of age and which continues until graduation from junior high school.
The protective effect of fluoride against dental caries occurs for early erupted teeth. Because the first molar, which has highest risk for dental caries, erupts during nursery school days, it is important to start the FMR program from this time point. In addition, the FMR program should be continued until the end of junior high school because permanent teeth continue to erupt during this period.
There have been many pervious reports on the effects of FMR for dental caries prevention in schoolchildren [2, 4-6, 12-16]. These reports show that the prevention rate was 35%-50% for children who had participated in FMR program during elementary school days, and 55%-80% for children who had participated in FMR program during not only elementary school days but also nursery school days. Nursery school, elementary school, and junior high school are the most suitable places for carrying out FMR program.
In addition, a systematic review was recently reported to evaluate the effectiveness of self- and professionally applied fluoride and water fluoridation among adults [17]. The findings suggest that fluoride prevents caries among adults of all ages [17]. Our study supported these findings. There is much literature on this subject. Several clinical trials on the effectiveness of fluoride were conducted before 1980. Because of the paucity of studies, the authors were not able to exclude studies without blind outcome assessment. There is a clear need for further well-designed studies.
In this study, it was impossible to obtain sociodemographic data on subjects. However, we thought that selection bias might have been limited because we selected subjects who participated in 1.5-year-old or 3-year-old dental and medical health examinations for their children. In addition, there were some subjects who participated in the FMR program in their childhood, but had some caries. The reason is unclear because of lack of any additional information.
CONCLUSIONS
In conclusion, the positive caries preventive effects of a school-based FMR program from nursery school to junior high school can continue in adults aged 20 years and older.

