All published articles of this journal are available on ScienceDirect.

Experimental Animal Models in Periodontology: A Review
Authors Info & Affiliations
Abstract
In periodontal research, animal studies are complementary to in vitro experiments prior to testing new treatments. Animal models should make possible the validation of hypotheses and prove the safety and efficacy of new regenerating approaches using biomaterials, growth factors or stem cells. A review of the literature was carried out by using electronic databases (PubMed, ISI Web of Science). Numerous animal models in different species such as rats, hamsters, rabbits, ferrets, canines and primates have been used for modeling human periodontal diseases and treatments. However, both the anatomy and physiopathology of animals are different from those of humans, making difficult the evaluation of new therapies. Experimental models have been developed in order to reproduce major periodontal diseases (gingivitis, periodontitis), their pathogenesis and to investigate new surgical techniques. The aim of this review is to define the most pertinent animal models for periodontal research depending on the hypothesis and expected results.
1. INTRODUCTION
The presence of oral bacterial biofilm in gingival and periodontal tissues provokes an immune-inflammatory response that can result in the progressive destruction of the structural components of the periodontium. This condition leads to the clinical signs of periodontitis, with the breakdown of the tooth-supporting structures until tooth loosening. In order to arrest the progression of the disease, scaling and root-planning are performed, together with rigorous oral hygiene. The objective of periodontal treatment should ultimately be to regenerate the periodontal tissue by using non surgical or surgical techniques, biomaterials for guided tissue regeneration, bone substitutes (e.g. Calcium phosphates or others), growth factors (e.g. enamel matrix derivatives) or, as more recently proposed, mesenchymal stem cells [1]. Appropriate experimental animal models are required for testing and validating new regenerative therapies for damaged periodontal tissues. Animal studies are effectively complementary to in vitro experiments prior to testing new clinical treatments where biopsy harvesting for histology is generally not accepted in human. Different animal species could be used for modeling periodontitis and treatments, but primates, dogs, rats, rabbits, pigs, hamsters and ferrets are the most commonly employed. Experimental animal models should be used with care, particularly primates and canines, for ethical reasons [2, 3]. It may be preferable to use small animals (e.g. rats, hamsters, rabbits, ferrets) but their physiopathology is not as similar as humans and so, experimental models needs to be reproducible in order to obtain relevant results.
Research in periodontology involves different strategies, principally the etiology of periodontal diseases using experimental models of periodontitis, and the regeneration of damaged periodontal tissues by surgically creating bone defects in combination, or not, with experimental periodontitis. The outcomes of animal studies using new biomaterials and therapies designed for medical applications other than periodontal diseases, such as filling bone defects in orthopedics, are not particularly valuable in the specific periodontal context. Periodontal lesions effectively appear as open and non vascularized cavities with chronic inflammation in the tissues and specific experimental models should thus be used. Concerning etiopathologic studies, non-human primates are preferred but large series are not ethically and economically acceptable. Small animal models (e.g. rats or hamsters) have been developed for periodontal research but these studies mainly focus on bacteriology and immune response.
Depending on species, periodontal diseases could be induced spontaneously, experimentally or both. In the context of regenerative medicine using biomaterials, large animal models have been preferred due to the reproducibility and surgical accessibility of experimental defects. Apart from monkeys, which are the ideal model in pre-clinical studies, dogs have been widely used for modeling the regeneration of periodontal defects with biomaterials. Some studies have also used rats, mini-pigs, sheep, rabbits and cats. Different methodologies have been proposed in order to ensure reproducible models that make statistical analysis possible.
The aim of this review is to summarize the animal models used for periodontal research. The first part concerns the choice of the most suitable animal model related to expected results. In the second part, the different animals will be detailed, describing their anatomy, physiopathology of periodontal disease and their preferential interest in periodontal research.
2. SELECTION OF ANIMAL MODELS FOR PERIODONTAL RESEARCH
The selection of an experimental model is determined by research objectives, as well as laboratory constraints such as housing of large or non standard animals. The use of large animals with ethical and social issues such as monkeys and dogs should be reserved for last phase validation of new treatments prior to use in human clinical practice. In most cases, small animal models such as rats or hamsters will be sufficient to assess the role of bacteria, diet or other factors in periodontal inflammation at the histological level, providing sufficient statistical significance and pre-clinical relevance.
Table 1 summarizes the different animal models used in periodontal research. The relevance of animal models for studying periodontal diseases, biomaterials, dental implants, or new regenerative strategies is indicated.
Decision Making of Laboratory Animal Model
| Research Based on Pathogenesis of Periodontal Disease | Research Based on Periodontal Treatment Modalities | ||||
|---|---|---|---|---|---|
| Pertinence of the Model | Disease etiology | Calculus | Immunology and Micriobiology | Biomaterials | Implant |
| Non Human Primates | Excellent | Medium | Excellent | Excellent | Good |
| Dog | Good | Good | Good | Excellent | Excellent |
| Minipig | Low | Low | Low | Good | Medium |
| Rabbit | Low | Low | Low | Medium | Medium |
| Ferret | Medium | Good | Low | Low | Low |
| Rat | Low | Medium | Good | Medium | Low |
| Hamster | Low | Medium | Good | Low | Low |
3. EXPERIMENTAL GINGIVITIS AND PERIODONTITIS
In order to study the origin and evolution of periodontal diseases, the animal model should have characteristics for the disease process that are similar to those encountered in humans. These experimental etiopathogenics studies should use indices similar to those in clinical practice: gingival index, calculus index, depth of subgingival pockets, tooth loosening. These experimental data may be completed with radiographs, blood immunology assays, bacteria determination and histology analysis.
Experimental studies conducted in monkeys are highly relevant for human clinical practice as they present comparable anatomy and develop similar periodontal diseases with similar clinical symptoms. However, experimental research in monkeys requires a strong ethical justification of their care and use and should take into account the purchasing, transportation and housing expenses of these animals over long periods.
The occurrence of periodontal diseases in dogs is high, increases with ageing and thus, the etiopathology is closely related to humans [4]. Although there are certain differences in the inflammatory response as well as in the bacterial population, dogs are widely used in gingivitis and periodontitis research. Calculus deposits lead to gingivitis [5] but contrary to humans, the sub-connective tissue remains almost normal in dogs. The conversion from gingivitis to periodontitis is not systematic but could be experimentally induced by fixing ligatures around the teeth [6, 7].
Rodents and rats in particular, are ethically relevant models for experimental periodontal research. The structure of the dental gingival area is quite similar to that observed in humans [8]. However, the occurrence of periodontal diseases in rats is less frequent than in human, although the pathology can be induced by inoculating bacteria, giving a carbohydrate-rich diet and fixing ligatures around the teeth. This experimental model is not optimal for studying the evolution of the disease over long periods using histology because of the continuous growth and migration of the teeth. This model is widely used for microbiological and immunological studies [9]. In addition, the use of gnobiotic or germ-free animals appears to be very interesting for the opportunities they give for carrying out mono-infections by periodontopathogens bacteria of human origin.
The etiopathology of periodontal diseases in hamsters is similar to that in rats. Experimental periodontitis is easily obtained by feeding animals with a carbohydrate-rich diet. In this model, research focuses on microbiology and immunology [10].
4. CALCULUS
Although monkeys are the most closely related model to humans, research on calculus has mainly been conducted on dogs, rats or ferrets. Abundant calculus deposits associated with periodontitis was observed in aged dogs. This model is therefore of value for testing different techniques for removing subgingival calculus. Rats and hamsters with appropriate feeding develop dental and subgingival calculus making research possible on large numbers of animals.
5. SURGICAL PERIODONTAL DEFECTS AND TREATMENTS
Different biomaterials and tissue regenerative treatments have been tested in large pre-clinical models, mainly monkeys and dogs and to some extent in pigs and rabbits. A literature research on Medline (key words: experimental periodontal disease, various animals such as dog, surgical techniques such as regeneration, biomaterials) gave about 200 publications, in the last ten years (1999 to 2009), in experimental periodontitis using biomaterials (guided tissue regeneration, grafting biomaterials or enamel matrix proteins) and tissue engineering. Most of these papers published in the last decade concern new materials as enamel matrix proteins or BMP, compared to standard procedures as guided tissue regeneration or grafting material, used to evaluate histologically the regeneration of periodontal tissues. Thus, the information obtained allows the passage to clinical use in humans.
The selection of these animals was based on similar pathologies and the ease of surgically created clinically-relevant defects. Experimental periodontal defects may be obtained in three different ways [11]: (i) the acute defect model, (ii) the chronic defect model and (iii) the acute/chronic defect model. In the acute model, all defects are surgically-induced by removing surgically all the periodontal components (bone, cementum and periodontal ligament). Reproducible defects in experimental and control sites are created. In the chronic model, lesions are obtained by placing orthodontic elastics, silk sutures or ligatures around teeth during 12 to 20 weeks, depending on the type of animal studied. These defects are deeper in the interproximal spaces than in the buccal or lingual surfaces. In the combined acute/chronic model, the defects are surgically-created and ligatures are placed to ensure calculus accumulation and to prevent spontaneous regeneration of the defects. Periodontal and osseous defects are created at the alveolar crest of the ramus bone. These studies concern critical-sized defects that will not spontaneously heal during the study in order to prevent bias. The size of the defect depends on the anatomy and physiology of the species considered. The most commonly used models in periodontal research are monkeys and dogs.
6. THE DIFFERENT ANIMAL MODELS IN PERIODONTOLOGY
The animals used in periodontal research have a different anatomy, dentition and structure of periodontal tissues. Furthermore, the physiopathology, oral bacteria and inflammation response vary between species.
1. Non-Human Primates
Monkeys have the advantage of probably being philogenetically similar to humans. All non-human primate species offer a wide range of sizes: from about 300 to 350 gram for certain marmosets, to sizes similar to humans for the largest such as chimpanzees and gorillas. All these species are diphyodont. Macaques, baboons and chimpanzees have the same dental formula as human: I 2/2, C 1/1, Pm 2/2 and M 3/3. However, marmosets have a different formula with I 2/2, C 1/1, Pm 3/3 and M 2/2. The anatomy of teeth and roots is close to that of humans, but the size is smaller. The canines in most non-human primates are elongate and prehensile. In gorillas and baboons, the premolars have more than one root.
Certain species of non-human primates have periodontal diseases at an adult age [12]. Histologically, the structure of the periodontium is also similar to that observed in humans. Microbiologically, in Macaca fascicularis (cynomolgus monkeys), the composition of the plaque is Gram positive rods and cocci for supragingival plaque and anaerobic Gram negative rods for subgingival plaque [13, 14]. The inflammatory response to periodontal disease is quite similar to that found in humans. Connective tissues are infiltrated by plasma cells, lymphocytes and neutrophils. In other species, such as squirrel monkeys and marmosets, there is very limited inflammatory infiltrate. These major differences with humans make them inappropriate models for studying the pathogenesis of periodontitis [15]. Nevertheless, the marmoset has been the most frequently-used non-human primate in periodontal research.
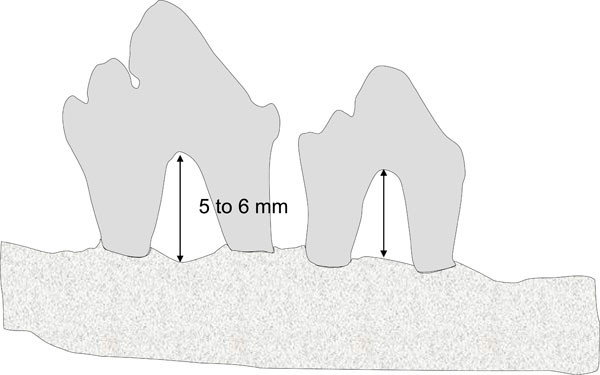
In the last ten years, 25 articles have been published using monkeys for research relating to periodontal healing [16-18] filling with biomaterials [19, 20], guided tissue regeneration [21], enamel matrix derivatives [22-24], or implant surgery [25-31]. These surgical approaches, are, for the most part, carried out on Macaca fascicularis. All the teeth can be used, which makes it possible to obtain an important number of test sites, with a limited number of animals. For example, in the study by Sculean et al. [23], 24 lesions (intraosseous and fenestration defects) were created at the level of the incisors and premolars in only 3 monkeys. The intraosseous defects (n=18) were located in the mesial part of each tooth and had a depth of between 6 and 8 mm (Fig. 1). In order to prevent any spontaneous healing and to promote plaque accumulation, metal strips were placed in the defects and were attached to the teeth using a composite material. Standardized critical-sized defects of the fenestration type (n=6) were made in the same monkeys. The defects were treated by guided tissue regeneration (GTR) or by induced guided regeneration by enamel matrix proteins (EMD). Control defects were treated with coronally repositioned flaps. This model is quite similar to those used in clinical human studies, and, for this reason, appears to be a pertinent animal model.

Intrabony defects on mesial root of monkey mandibular molars as described by Sculean et al. 2000.
Class III furcation lesions can also be used as surgical periodontal model in the mandibular molars of monkeys [32].
Monkeys were used because they present anatomical similarities with humans. However, it is difficult to obtain a large number of animals and it is thus imperative that a maximum number of defects be created in order to obtain a sufficient quantity of test and control sites to make adequate statistical analysis of the results possible. Moreover, ethical considerations and regulations should be fulfilled in order to prevent any trafficking of protected species.
2. Dogs
Many experimental studies on gingival and periodontal diseases have been conducted in dogs. The beagle is one of the most commonly used due to its size and its extremely cooperative temperament. Globally, all periodontal tissues and the size of the teeth are quite similar to those observed in humans. However, some major differences exist between dogs and humans as the lack of lateral movements, no occlusal contacts for all the premolars and presence of open contacts between teeth. The frequent lack of gingival sulci and crevicular fluid, a different composition of periodontal plaque and calculus are other important differences between dogs and humans [33]. All dogs are diphyodont with deciduous and permanent dentition. The formula for permanent dentition is I 3/3, C1/1, Pm 4/4, M 2/3. All domestic dogs have a natural susceptibility to periodontal diseases in adult age but may be maintained healthy by appropriate plaque control. Periodontal alterations, including gingivitis and periodontitis, increase in prevalence and severity with age, faster than in man but with the same etiologic factors. Gingivitis may be generalized and associated with bleeding on probing, the presence of supragingival and subgingival plaque, calculus and severe bone loss including osseous defects. Currently, gingival recessions appear in the severe forms of periodontal diseases in dogs. Supragingival plaque is mostly composed of Gram positive cocci. The subgingival flora is mainly anaerobic Gram negative cocci and rods (Porphyromonas gingivalis, Fusobacterium nucleatum, Capnocytophaga).
Gingivitis in dogs may be accelerated by an appropriate soft, minced diet, promoting the accumulation of supragingival plaque and calculus [34-37]. In healthy dogs, the gingival sulcus is most frequently absent. The junctional epithelium and epithelial attachment extend to the most coronal level on the gingival margin. In early gingivitis, the inflammation is limited to this marginal part of the gingival tissue with the presence of neutrophils and monocytes leaving most of the connective tissue free of infiltrate. At the later stages, the infiltrate extends apically subjacent to the junctional epithelium with the formation of gingival pockets.
Periodontitis in dogs occurs on the basis of pre-existing gingivitis. There is a formation of periodontal pockets lined with typical pocket epithelium. In the connective tissue, the dense cellular infiltrate consists mainly of plasma cells and lymphocytes. The osteoclastic resorption of alveolar bone may result in deep, narrow lesions extending vertically around a single root leaving the interdental space intact [38, 39]. The bone defect can involve the furcation areas of premolar and molar teeth. In colony dogs, periodontitis appears earlier and more severely than in domestic dogs [40]. The bifurcation regions are more frequently deteriorated than the interdental spaces. The first and second premolars are the most frequently lost teeth.
In summary, the prevalence and severity of gingivitis and periodontitis in dogs increase with age but vary markedly between the different breeds. Some dogs are susceptible to periodontal disease and others are more resistant. The differences can be explained more by the nature of the infection or genetics than by diet. In these natural periodontal diseases, the extent and localizations of the periodontal lesions are not homogeneous [41], which may be considered to be a limitation for the model.
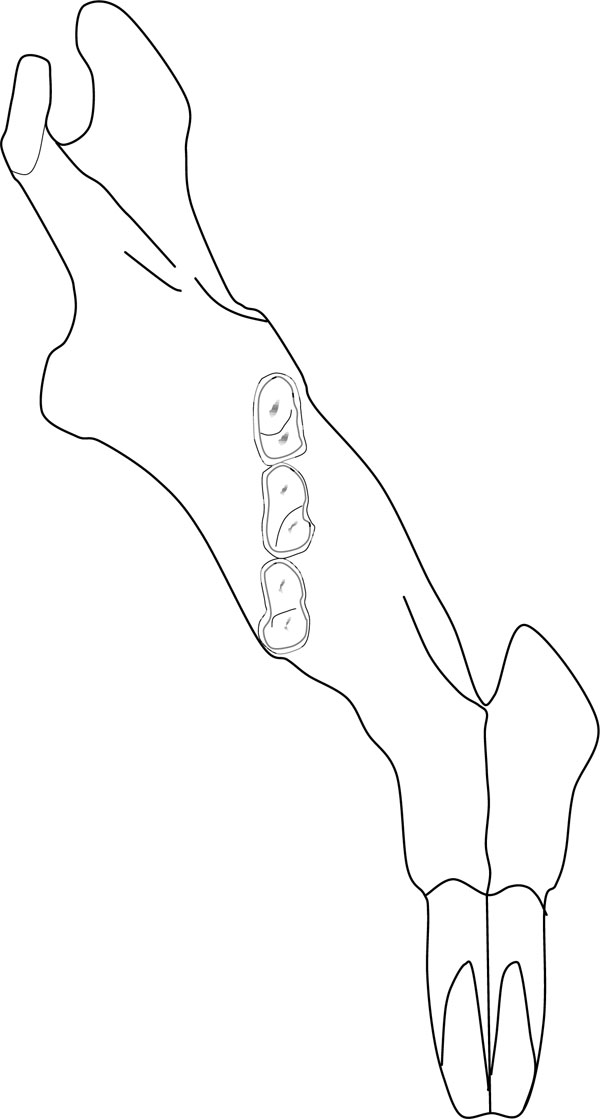
More than one hundred publications were found for periodontal research involving dogs for healing defects with various biomaterials, membranes, or with enamel matrix derivatives. A surgical model was proposed by Wikesjo in 1994 [42]. Critical-sized supra-alveolar defects [42, 43], measuring 6 mm, were created at the level of the mandibular premolars (Fig. 2). The class III furcation defects thus obtained made it possible to test various regeneration procedures, whether or not they were associated with a filling biomaterial [44-46].
Supraalveolar critical size periodontal defects on dog mandibular premolars as described by Wikesjo et al. 1994.
Two methodological approaches were described: treatment of surgical defects on the 3rd and 4th mandibular premolars [47-49], or a test based only on the 3rd premolar after avulsion of the 2nd and 4th premolars [50-53]. These approaches were used to evaluate regeneration procedures using BMP, GTR, enamel matrix proteins or grafting materials as bioactive glass [54-57].
On the upper jaw, intraosseous defects on premolars and molars were also described [45, 58, 59]. The number of residual osseous walls present at the level of the surgical defect was considered to be an important factor for healing. Defects of 4 mm in width and depth with 1 or 3 osseous walls were regarded as reproducible and relevant models for evaluating biomaterials in periodontal regeneration [60, 61]. The formation of critical-sized fenestrations on the buccal face of maxillary canines may also make it possible to evaluate filling biomaterials or regeneration techniques [62-67]. Defects in the form of dehiscence at the level of the buccal roots of the molars were also created in dogs [68]. Dogs also served as the animal model in muco-gingival surgery by creating recessions on the canines which were treated either by palatine connective tissue grafts, or by guided tissue regeneration [69-71].
Concurrently to these surgically-created lesions, it was also possible to obtain experimental periodontal defects by placing silk bindings around the teeth for a period of 4 to 6 months [72, 73] or to use spontaneous class II furcation defects occurring with periodontal disease in old dogs [74,75]. Combined techniques, such as placing bindings associated with surgical creation of periodontal defects, were also used to evaluate filling biomaterials and/or regeneration procedures [76, 77]. Dogs were also used as models in guided osseous regeneration [78, 79] and in implant surgery [80-82]. The ramic angle is also used in the implant approach, creating critical-sized defects filled with various biomaterials [83]. Peri-implantitis was induced by installing, for two months, bindings around dental implants. The osseous defects around the implants obtained in this way seemed relatively comparable with those observed in humans [84]. More recently, a study in dogs has reported research on mesenchymal stem cells and tissue engineering in the treatment of periodontal diseases [85-88]. In summary, the most commonly used animal model in periodontal research seems to be dogs due to reproducible critical-sized defects.
3. Rats
The rat is the most extensively-studied rodent for the pathogenesis of periodontal diseases. Typical rodent dentition is I 1/1, C 0/0, Pm 0/0, M 3/3. The incisor is rootless. The structure of the dental gingival area in rats is quite similar to that observed in humans [8], with a shallow gingival sulcus and attachment of the junctional epithelium to the tooth surface. However, there are some differences: the first is the keratinisation of the crevicular epithelium in rats; the second is the relationship between the gingival and junctional epithelium with desmosomal contact between the most superficial cells of the gingival epithelium and the non keratinized cells of the junctional epithelium [89]. Despite this structural difference, the junctional epithelium appears to be a pathway for foreign substances, bacterial endotoxins, and for inflammatory cell exudations, similar to what occurs in humans.
As rats age, their dental tissues evolve, including continuous eruption of the teeth with permanent apposition of cementum and bone in relation to wear on all molar occlusion surfaces. All these phenomena cause a progressive shift in the position of the molars in three-dimensional space, resulting in global movement in an occlusal-distal-buccal direction compared to the occluso-mesial drift observed in humans. Wear on the occlusion surfaces leads to anatomical crown attrition and an increase in root length by apposition of cellular cementum. The cemento-enamel junction moves with time in an occlusal direction more rapidly than bone deposition at the alveolar crest. All components of the periodontal tissues are in permanent remodelling and the continuous occlusal-distal-buccal movement of rat molars appears to be a physiological expression of adaptive changes required by growth changes in the jaws and by rapid occlusal wear [15]. All these physiological and age-related phenomena have a strong impact on the interpretation of data obtained in experimental periodontal diseases, not only in rats but also in other rodents.
Under natural conditions, the rat appears to be extremely resistant to periodontal diseases, which is a remarkable difference with humans. Nevertheless, some strains may develop periodontitis by inoculation of specific bacteria, or with an appropriate diet, increasing the percentage of carbohydrates in food that accelerates the progression of the disease [15], or by fixing ligatures around the teeth (Fig. 3). The first step in periodontal alterations observed in disease-susceptible strains is the appearance of marginal gingivitis with edema and ulcerations. Secondly, there is formation of deep pockets filled with food debris and hair. In severe degrees of periodontitis, the lesions affect the interradicular and interdental spaces with extensive alveolar bone resorption and denudations of the molar roots [15].
Placement of silk or cotton ligatures around teeth on rats.
The most commonly-used strains are Wistar or the Spraque-Dawley. In periodontal disease-resistant strains, like germ-free Spraque-Dawley or white Lobund, experimental periodontitis may be obtained by using silk ligatures tied around the molars or by specific bacterial inoculations [90].
In rats, periodontitis appears to be an infectious process. Inoculations or injections of various periodontal pathogens such as Prophyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Fusobacterium nucleatum, Capnocytophaga, Eikenella corrodens, Actinomyces viscosus, and Streptococus sobrinus can induce periodontal lesions [91]. After infection, the destruction of the periodontal tissue occurs quite rapidly. Inoculating Gram-negative bacteria induces a poor inflammatory response which is not similar to that found in humans. There are mainly neutrophils, few lymphocytes and an absence of plasma cells in the gingival tissues. Tissue destruction and host-response are different and depend on the type of bacterial agent applied. In rats, the appearance of gingivitis is not a systematic precursor of periodontal breakdown. At this initial stage, inflammation may only be localized around the junction epithelium. In this region, there is high phagocytic activity and neutrophils form a protective barrier. Bone resorption is then inconstant. Acute interdental inflammation characterized by an ulcerated junctional epithelium, infiltration of all supra-alveolar connective tissue by neutrophils and high osteoclastic activity has been observed in only about 10 % of animals up to 100 days of age [92, 93]. The osseous defects observed were principally crater-like. The lesions were filled with bacteria in contact on one side with the entire root surface and on the other side, with residual connective tissue infiltrated by neutrophils, macrophages and lymphocytes. In Gram-negative infection, mainly periodontal lesions develop and quite early in the maxilla, later on the mandible. The appearance of severe crater-like bone defects may occur six to eight weeks after infection, and depends on the type of bacteria. The destructive process in response to Gram-negative bacteria can take place in the absence of cell-mediated immune response [94].
In the last 10 years, a surgical model in rats has been proposed [95]. As shown in Fig. (4), this model consists of surgically creating a periodontal defect in the form of fenestrations on the radicular surfaces of the second mandibular molars. After an extraoral incision, the bone in front of the second molars, as well as cement, were eliminated by using a burr under saline irrigation. The defects were standardized both in terms of depth (1.5 mm) and width (3 mm). This surgical model on the rat was reprised by Huang [96]. The rat was also used to evaluate the healing of supra and intraosseous defects after use of enamel matrix derivatives [97]. In these studies, standardized defects were created surgically in the roots of the first molars. The ramus area was also proposed to evaluate guided osseous regeneration techniques [98]. The toothless alveolar crest between the incisor and the first molar, or the edge of the mandible, are also interesting surgical models in guided osseous regeneration [24, 32]. Furthermore, rats are well accepted animals for experimental research. The breeding and housing costs are relatively low, making it possible to carry out studies with sufficient numbers for statistical analysis. However, the continuous occlusal eruption and osseous apposition on the dental roots makes the modelling and analysis of the results difficult and can result in significant bias. The use of rats in a surgical defect model seems promising, however, and should develop in the years to come [99].
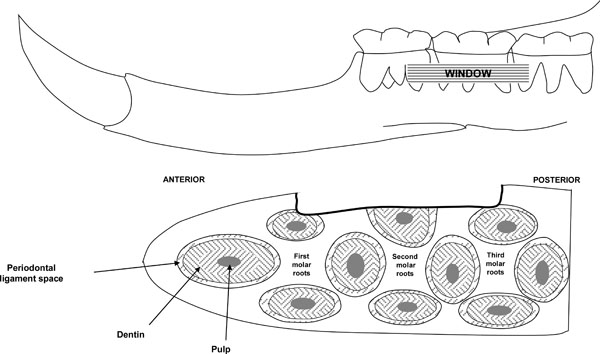
Periodontal surgical defects on rats as described by King et al. 1997.
4. Hamsters
In hamsters, periodontal disease does not occur spontaneously but may be obtained experimentally. The golden Syrian hamster is the most commonly used. The dentition formula is identical to rodents: I 1/1, C 0/0, Pm 0/0, M 3/3. As in rats, the molars move with time following the growth of the jaws and occlusal wear. The shift in the occluso-distal direction and the continuous eruption of molars seem to be less evident than in rats. Histologically, the structure of the periodontal tissue is very similar to that of rats [100] but due to the small size of this kind of animal, the interdental septum is narrower than in rats. Spontaneous periodontal disease was obtained using an appropriate diet containing high concentrations of carbohydrates, particularly sucrose [10]. With this specific diet, the plaque consisted of formic acid bacteria mixed with food debris, affecting principally the palatal and lingual surfaces, more than buccal. After plaque accumulation, there was a breakdown located at the junction epithelium and formation of crater-like gingival pockets. The inflammatory response consisted principally of neutrophils. Osteoclastic activity was stronger on the palatal and interdental side of the molar. Due to the small size of the interdental crest, bone resorption was almost exclusively horizontal with alteration of the interradicular spaces. The dynamics of alveolar bone resorption decreased significantly along the alveolar walls, and the palatal and lingual regions reacted more strongly than the buccal regions, which seemed quite inactive [101].
In summary, as in rats, the inflammatory response is very limited in hamsters and is very different from that observed in humans. The mechanisms of alveolar bone resorption in hamsters with diet-dependent periodontal lesions are quite similar to those observed in rats infected with Gram-positive bacteria.
5. Ferrets
Ferrets have a deciduous and permanent dentition. The formula is I 2/2, C 1/1, Pm 4/4, M 2/2. Ligature-induced periodontitis was obtained within 4 weeks [102, 103]. The evolution in the periodontal lesions was quite similar to that observed in humans. As the disease progressed, calculus increased both in quantity and extent. The gingiva showed signs of inflammation. Secondly, after the junctional epithelium split, gingival pockets formed that were similar to those observed in hamsters. At the histological level, the connective tissue showed large numbers of neutrophils, plasma cells and lymphocytes. Alveolar bone resorption was severe, rating up to 50 % [104].
6. Minks
The dentition formula of the adult mink is I 3/3, C 1/1, Pm 3/3 and M 1/2. In minks, spontaneous periodontitis, which is age- and plaque-dependent, is observed. Nevertheless, the extent of this periodontal disease appears to be severe only in very old animals. Ranch-raised minks may carry Chediak-Higashi syndrome (CHS), genetically transmitted by an autosomal trait [105]. Young adult minks with CHS have developed aggressive periodontitis, accompanied by severe periodontal lesions and bone loss. The extent of the gingiva was quite different between the maxilla and mandible. In the upper jaw, the vestibule was deep. The incisors and canines showed a large band of attached gingiva. The later is less important at the level of the premolars and molars. In the lower jaw, the amount of attached gingiva is narrow in the incisors and premolars. Around the molars, attached gingiva appeared to be comparable to that observed in the upper jaw [106]. In CSH-affected minks, periodontal disease occurs rapidly with a high hemorrhagic inflammatory response in the marginal gingiva. Bone resorption may be variable and associated with bone crater formation and furcation lesions, correlated with the location and extent of the gingival inflammation. Histologically, the inflammatory response appears to be quite different from that observed in humans with an acute exudative and persistent inflammatory reaction added to vascular proliferation. At the level of the marginal gingiva, there was proliferation of the blood vessels, all this zone was invaded by neutrophils. The epithelium extension into connective tissue was, in proportion, greater than in other species. The space occupied by connective tissue decreased dramatically. Plasma cells and lymphocytes were rare. In CHS-minks compared to normal minks, the quantity of neutrophils and small vessels, the extent and severity of the epithelial proliferation as well as bone resorption strongly increased. In minks, neutrophils play a key role in periodontal destruction due to deficiencies in the chemotactic response and massive release of lysosomal enzymes and proteases into periodontal tissue. Minks are therefore interesting experimental models in research on the etiology of periodontal diseases. Nevertheless, housing these animals may be difficult or require specific authorizations that may explain the absence of recent publications in the literature.
7. Other Species
Other animal models have been investigated for modelling periodontal diseases. For instance, mice have been studied but periodontal disease is very different to that observed in humans. The dental formula of mice is typical rodent dentition: I 1/1, C 0/0, Pm 0/0, M 3/3. Incisors have continuous growth and molars present complex physiological modifications with ageing. There is occlusal wear, bucco-occlusal motion and high hypercementosis at the apical part of each root [107]. Periodontal alterations are characterized by bone loss which is more severe at the lingual and palatal sides of the molars than at the buccal sides. There is also the presence of crater-like defects at the interdental and interradicular spaces. However, periodontal disease does not appear in mice younger than one year. The inflammatory response is relatively poor. The extensive physiological alterations in molar position in the alveolar socket over time mean that mice are not the best model for studying natural or induced periodontal disease.
Sheep have also been studied in the context of periodontal diseases. The permanent dentition of sheep consists of 32 teeth with a formula: I 0/3, C 0/1, Pm 3/3, M 3/3. The incisors have a very short root and are physiologically mobile. Periodontitis may affect these anterior teeth and is quite rapidly accompanied by deep periodontal pockets and severe bone loss. Histologically, the pocket wall is covered by a typical pocket epithelium. The connective tissue behind it is infiltrated by plasma cells. At the base of the pocket, the junctional epithelium is very short and connective tissue is infiltrated by neutrophils migrating to the apical plaque border , then forming an interface layer [108]. The inflammation of the gingiva appears to be moderate. However there are no recent publications available using sheep as the animal model in periodontology.
Rabbits have mainly been used for testing biomaterials or for treatment of peri-implantitis. However, transcortical drilled holes creating tibial or radial critical-sized femoral defects are traditionally the most commonly used models in rabbits [109-111]. These defects in long bone are far from the specific situation of periodontal diseases but appear as a very interesting model for testing the bone healing.
One publication [112] used the cat as animal model. In this research, class III furcation defects were surgically created at the level of the premolars in order to study ankylosis at root level during periodontal healing.
Five studies have reported mini-pigs for research, mainly related to dental implant surgery and periodontal regeneration by enamel matrix derivatives [113, 114], as well as the effects of dental lasers on periodontal healing [115].
CONCLUSION
Experimental models for periodontal diseases are essential for understanding the origin and evolution of the pathology in humans. The use of animal models in periodontal research is a necessary step prior to entering into clinical trials with new biomaterials and treatments. The anatomy, physiology and pathogenicity of experimental models should relate as much as possible to those of patients in order to demonstrate the safety and efficacy of new biomaterials or treatments in periodontal regeneration. Monkeys are the models that are closest to human beings in terms of dental anatomy and physiology, but their use is limited by ethical and economic constraints. Experimental models in dogs have been widely used in periodontal research. As with monkeys, studies in dogs are difficult and protocols should rationalize the lesions as much as possible in order to obtain statistically exploitable data. Monkeys and dogs, as their anatomy and physiopathology are comparable to those of humans, should be restricted to pre-clinical studies for validating new treatments. Apart from these large animal models, smaller, easier to maintain and less expensive species have been proposed. Rats and hamsters develop experimental periodontal diseases. A surgical model for periodontal critical-sized defects in rats has been validated, making it possible to test new biomaterials in combination with growth factors or mesenchymal stem cells. The use of gnobiotic or germ-free rats is a major model for all research on the microbiology of periodontal diseases. In the same way, the gilded hamster remains an interesting model for any immunological research. However, the continuous growth of the teeth in rodents makes the modeling more difficult to understand, but this problem seems to have been solved in this last decade. New avenues are now available in periodontal research, allowing larger cohorts that are easier to maintain. A more systematic use of these small animal models appears evident for future research, especially from a surgical point of view.

