All published articles of this journal are available on ScienceDirect.

The Relationship Between the Mid-Point and Most-Prominent Point on the Labial Curve of Upper Anterior Teeth
Abstract
Objectives: This study investigates coincidence of the most-prominent point and the mid-point on upper anterior teeth in relation to the use of straight-wire appliances.
Materials and Methods: Alginate impressions of the upper jaw were obtained from forty Caucasian patients. Impressions were cast using hard dental stone. The teeth on each upper study model (canine to canine) were marked along the facial axis of the clinical crown (FACC line) then separated using a very thin diamond disc. Each tooth was mounted on a glass slide using sticky wax and cut into two halves down this FACC line. Images were acquired of the sections and a straight line connecting the gingival margin and the incisal edge was drawn on the flat cut surfaces (now the proximal crosssectional view). From this line, perpendicular lines were drawn at the mid-point and most prominent point to the labial curve. Coincidence rate was calculated or whether the most prominent point was gingival or incisal to the mid-point.
Results: Approximately 80% of upper central incisors had coincident mid- and most-prominent points. Upper lateral incisors and canine teeth had approximately 50% coincidence. The vast majority of cases without coincidence showed the most-prominent point incisal to the mid-point for all tooth kinds with just 5% or less gingival.
Conclusions: The high proportions of non-coincident examples found suggest that clinicians should be aware of individual variation and that this may possibly effect 3rd order alignment.
INTRODUCTION
Modern orthodontics has been described as the creation of the finest occlusal relationship within the framework of acceptable facial aesthetics and stability of occlusal result [1]. This requires positioning the crown of each individual tooth in its appropriate position for optimum function and appearance. Straight-wire appliances were designed to reduce or eliminate the need for placing bends in fully engaged straight arch wires. Andrews [2] studied the average torque angles, rotation angles, height and depth of each facial surface of each tooth type from untreated and treated patients having excellent occlusion. He found that when the brackets are precisely positioned at the midpoint of the facial axis and aligned with the facial axis, they collectively become the appliance providing specific tip, torque, rotation angle, height and depth position for each tooth. Limitations have been found in the effectiveness of this bracket system due to several factors, the most important of which is inaccurate bracket positioning [3]. This inaccuracy can only partly be blamed on clinician error as positioning the brackets on the mid-point should ideally be the same location as the most- prominent point [2] to ensure the desired torque effects and tooth movement. These points, however, do not always coincide and in fact may vary around each other to a large degree.
This study was conducted to evaluate the coincidence rate of the mid- and most-prominent points on the labial surface of upper central and lateral incisors and upper canines and possible implications when using straight wire appliances.
METHOD
One hundred and fifty patients presenting for treatment in the Orthodontic Department, School of Clinical Dentistry, Sheffield, UK were examined by one Orthodontist. Each patient file contained a medical questionnaire signed by the patient’s guardian, along with a written examination sheet signed by an orthodontic consultant indicating the level of the patient’s oral hygiene, general records, x-ray records and occlusion type. Any missing teeth, supernumerary teeth or other abnormalities were also noted. From the one hundred and fifty patients, forty fulfilled the following inclusion/ exclusion criteria: all patients were of Caucasian origin, aged between 13-16 years, had fully erupted upper incisor and canine teeth, good oral hygiene, with a healthy gingival margin around the upper anterior teeth, intact teeth e.g. no restorations, attrition or abrasion, mild or no crowding in the anterior region and the cases did not exhibit any abnormality of tooth number, form or structure and no medical or other health problems. This sample size exceeded others used within the department for morphology studies after statistical advice and calculation. The authors suggest that further calculations may be required when considering cases other than those with class 1 relationships.
The age of the sample was limited to between 13 and 16 years old to ensure that the teeth of interest were fully erupted but not worn. There were no restorations of their crowns.
An alginate impression (Alginoplast, Bayer) was taken of the upper jaw of the forty patients using hard dental stone (Kaffir D, British Gypsum. All the study models were duplicated using Erkoflex (2mm EVA, Erkodent, Germany).
SECTIONING THE UPPER ANTERIOR TEETH
All practical work was carried out by one examiner. The upper anterior teeth on each study model (canine to canine) were marked along the facial axis of the clinical crown FACC line [4], with a thin pencil (size 0.3 mm). The FACC line was located manually using electronic callipers accurate to 0.01mm (Mitutoyo, Japan). A pencil line was placed down the centre of the labial surface to pass through 2 marks made halfway between the calliper widths at 2 different positions down the crown length. A line was then drawn through these points to meet with the gingival margin in one direction and the incisal edge in the other direction (Fig. 1). The teeth were individually separated using a very thin diamond disc (Microslice II precision slicing machine, Malvern Instrument, England) with a round annular blade having the cutting surface on the inner edge. The blade was approximately 17.5cm in diameter and 0.3mm thick. Each tooth was mounted on a glass slide using red wax and yellow sticky wax. The labial tooth surface was aligned parallel to the glass slide, so that the FACC line was perpendicular to the slide edge to aid alignment for cutting the tooth along this line. Information for later identification was added to each slide prior to cutting. The slides were placed on the platform beneath the cutting disc and adjusted such that the pencil line was parallel to the cutting edge of the blade. The platform of the machine was adjustable (0.01mm steps) facilitating precise positioning of the slide. Red and green marker spots were used for identifying the mesial and distal portion of each sectioned tooth and included in subsequent imaging.
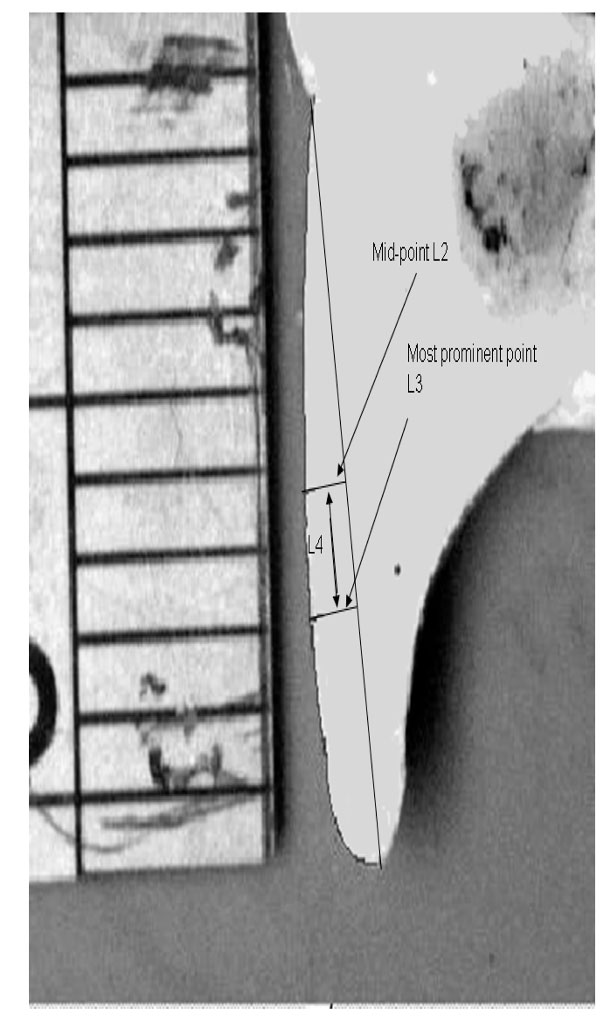
Proximal section of a central incisor displaying the variables.
IMAGE ANALYSIS SYSTEM
A computerised image analysis system [5] was used to analyse the study models. A 32-bit digital camera (Kodak Nikon DCS 410, with a 1.5 mega pixel resolution in an array of 1012 × 1524 pixels, producing 4.6 MB TIF files) was attached to a copy stand (Kaiser, Germany) using an adjustable camera mount. The copy stand had a base marked with a grid to aid specimen relocation. The camera was connected to a computer (Viglen CX1 Dual processor, 2× 850 MH2 CPU's, Viglen Ltd, UK) via an Adaptec 2940 SCSI card (KJP Ltd, UK). Light was provided by two white fluorescent tubes on the right and left side of the copy stand. Each light was adjustable in all three planes.
ACQUISITION AND STORAGE OF IMAGES
Images were displayed using Adobe Photoshop acquisition software (V5.02, Adobe Systems, Ltd, Europe) and viewed within ten seconds on the computer screen. Once acquired, each image was checked for quality and re-imaged if necessary. The images were saved as tagged image format files (TIFFs) as this format contains all of the original data. A permanent database was created of the original images.
PROXIMAL SURFACE OF UPPER ANTERIOR TEETH
Each tooth section was placed on a blue rubber base to provide consistent background contrast when imaged, and a steel rule was placed on the base adjacent to the tooth section for calibrating the image. All the sections were positioned with the same orientation to remove the need to rotate the images on screen later. Following acquisition each image was viewed using “Adobe PhotoShop” and was re-imaged if required.
The perimeter of the labial curve was traced from the gingival margin to the incisal edge. A straight line connecting the gingival margin and the incisal edge called the proximal line was then drawn (Fig. 1). The distance (L2) from the proximal line to the labial curve at the mid point was then obtained using the ‘length’ option within the Image Pro Plus software (version 4, Media Cybernetics, UK). Similarly, the most prominent point of the labial curve to the proximal line was obtained by drawing a tangent parallel to the proximal line using the length option (L3). The point at which the tangent was the greatest length from the labial curve was the most prominent point. The vertical distance between L2 and L3 along the proximal line was determined (L4). L4 was measured and was either negative or positive in value, according to the position of the most prominent point being incisal or gingival respectively to the mid-point (Fig. 1).
DATA ANALYSIS
The reliability of the total procedure was calculated from 20 of the study models (10 male and 10 female randomly selected) and included duplicating study models, re-sectioning and re-imaging the cut sections. The labial curve (gingival margin to incisal tip along the labial edge of the section) and the proximal line were used to show that the mesial and distal portions of the teeth were reproducibly created and that either side could have been chosen. The mean difference, standard deviation of the difference, standard error of the difference and intra-operator repeatability coefficients were calculated as well as Fleiss [6] Intra-class Correlation Coefficient of Reliability (ICCC). Bland Altman plots were produced for all repeat measures to ensure no size/error relationships and to check for outliers and bias [7].
For L2, L3 and L4 forty cases were assessed for the experimental data including the mean value, standard deviation and range (minimum and maximum values). A negative L4 value signifies the most-prominent point is incisal to the mid-point, whereas a positive L4 values infers the most-prominent point is gingival to the mid-point (Fig. 2). The authors would also like to recognise the importance of further study assessing the shape of posterior teeth. These could not be considered here due to time constraints of the main author.
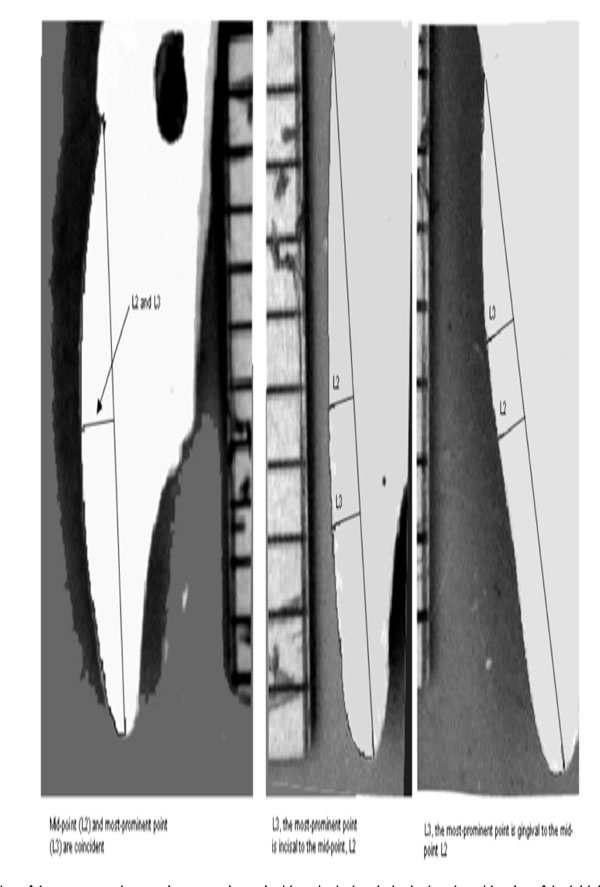
Examples of the most-prominent point presenting coincident, incisal and gingival to the mid-point of the labial curve.
RESULTS
Reliability
Table 1 shows that comparison of measurement of the labial curve and the proximal line from both mesial and distal gave ‘excellent repeatability’ according to Donner and Eliasziw [8] classification of Fleiss ICCC [6]. This indicates the model preparation, cutting and imaging and variable measurement was repeatable. This data also qualifies that either the mesial or distal slice could be used, with confidence and produce the same findings (Table 1). It was clear from the Bland Altman plots and the fact that all the mean differences were less than 1.96 x Standard error that the method produced no significant bias.
Reliability of the Preparation of the Proximal View Slices (N=40)
| Variable | Labial Curve | Proximal Line |
|---|---|---|
| Mean difference | 0.00 mm | 0.03 mm |
| SD of differences | 0.44 mm | 0.22 mm |
| SE of differences | 0.10mm | 0.050mm |
| Repeatability coefficient | 0.86mm | 0.43mm |
| ICCC | 0.94 | 0.95 |
Table 2 shows repeat measurements for variables L2, L3 and L4 for all three tooth types. Repeat measures were taken a week after the initial measurement. All the variable measurements produced ‘excellent repeatability’ with no significant bias found.
Reliability of Slice Preparation and Measurement (N=40). Left and Right Teeth Combined (mm)
| Central Incisors | Lateral Incisors | Canines | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | L2 | L3 | L4 | L2 | L3 | L4 | L2 | L3 | L4 |
| Mean difference | 0.02 | 0.03 | 0.00 | 0.03 | 0.02 | 0.00 | 0.02 | 0.03 | 0.00 |
| SD of differences | 0.09 | 0.08 | 0.06 | 0.08 | 0.08 | 0.01 | 0.09 | 0.09 | 0.08 |
| SE of differences | 0.02 | 0.02 | 0.01 | 0.02 | 0.02 | 0.00 | 0.02 | 0.02 | 0.02 |
| Repeatability coefficient | 0.18 | 0.16 | 0.12 | 0.16 | 0.16 | 0.02 | 0.18 | 0.18 | 0.16 |
| ICCC | 0.93 | 0.93 | 0.98 | 0.83 | 0.81 | 0.99 | 0.95 | 0.95 | 0.99 |
Tables 3 and 4 show the anterior labial curve is not flat (has a most-prominent point) and is often not symmetrically curved, as there are a high percentage of cases displaying a difference between the position of the mid-point and the most-prominent point. The most-prominent point on all tooth types was mainly incisal to the mid-point if it was not coincident with only a small percentage gingival to the mid-point. The upper lateral incisors showed the greatest number of instances where the most-prominent point was incisal, followed by the canines with the central incisors showing the greatest coincidence and therefore symmetry.
Descriptive Statistics for L2, L3 and L4 for 40 Right and Left Upper Anterior Teeth (mm)
| Variable | Range | Mean | Sth. Deviation | |
|---|---|---|---|---|
| Upper right central incisors | L2 | 0.77, 1.91 | 1.18 | 0.25 |
| L3 | 0.77, 1.91 | 1.20 | 0.27 | |
| L4 | -2.08, 1.10 | -0.14 | 0.59 | |
| Upper left central incisors | L2 | 0.39, 1.64 | 1.08 | 0.30 |
| L3 | 0.74, 1.64 | 1.14 | 0.24 | |
| L4 | -2.69, 1.02 | -0.56 | 1.07 | |
| Upper Right Lateral Incisors | L2 | 0.50, 1.42 | 0.90 | 0.19 |
| L3 | 0.68, 1.42 | 0.97 | 0.16 | |
| L4 | -2.25, 1.07 | -0.89 | 0.95 | |
| Upper Left Lateral Incisors | L2 | 0.57, 1.50 | 0.94 | 0.22 |
| L3 | 0.70, 1.50 | 1.00 | 0.19 | |
| L4 | -2.14, 0.00 | -0.69 | 0.86 | |
| Upper Right Canines | L2 | 0.59, 1.87 | 1.01 | 0.29 |
| L3 | 0.75, 1.99 | 1.08 | 0.27 | |
| L4 | -2.50, 0.90 | -0.75 | 0.96 | |
| Upper Left Canines | L2 | 0.61, 2.02 | 1.07 | 0.31 |
| L3 | 0.61, 2.07 | 1.11 | 0.32 | |
| L4 | -2.62, 1.40 | -0.33 | 0.91 |
Percentage of Most-Prominent Point’s Found Coincident, Incisal or Gingival to the Mid-Point’s on Upper Anterior Teeth
| Tooth Type | Tooth Location | Coincident | Incisal | Gingival |
|---|---|---|---|---|
| Upper Central Incisors | Right | 82.5% | 12.5% | 5.0% |
| Left | 72.5% | 25.0% | 2.5% | |
| Upper Lateral Incisors | Right | 47.5% | 50.0% | 2.5% |
| Left | 60.0% | 40.0% | 0.0% | |
| Upper Canines | Right | 55.0% | 42.5% | 2.5% |
| Left | 75.0% | 20.0% | 5.0% |
DISCUSSION
From Tables 1 and 2 it is clear that this method was repeatable and therefore a sound approach to assessing the curvature of upper anterior teeth from study models. All ICCC’s were in the excellent range of reliability and the Bland Altman plots showed no significant bias and acceptable repeatability coefficients.
Previous research studies have investigated the variation of tooth morphology and its relationship to bracket positioning. Variation in labial tooth surface morphology affects the angle at which a bracket may be seated in relation to the facial axis of the clinical crown. It has been presumed, in respect of bracket placement, that the mid-points and most-prominent points are coincident on the labial surface of anterior teeth [4,9]. This study has shown, for the first time that these two points show coincidence at approximately 80% on central incisors reducing to approximately 50% on lateral incisors and canines. This means that on approximately 20% of central incisors and 50% of laterals and canines, brackets will be placed at the mid-point of the labial curve when it is not the most-prominent point. In this situation the labial curve is not symmetrical vertically about the mid-point such that the bracket will not sit in the preferred position parallel to the proximal line (facial axis of the clinical crown) as mentioned by Andrews [2]. This situation could introduce axial forces affecting the inclination of these teeth (3rd order correction) and increase the need for extra final adjustment after initial alignment. Our data is in agreement with previous tooth morphology studies on labial surface variation [10-15] but provides extra specific information regarding mid- and most-prominent point coincidence and location.
This study only considered class 1 relationships from patients requiring minor adjustments only to the lower dentition. The size and shape of a tooth will obviously affect the amount of torgue/ force required but the effect of each measurement variation would require a separate study. This paper and study discuss’ the effect of the curvature of the tooth surface and therefore difference between the mid and most prominent points only.
CONCLUSIONS
This method of preparing proximal sections of upper anterior teeth from study models and there subsequent measurement by image analysis, has demonstrated a reliable way of assessing coincidence of mid- and most-prominent points on the labial surface of upper anterior teeth.
The assessment of mid- and most-prominent point location on the central incisor cases showed greatest symmetry with only 20% of cases having non coincident mid- and most-prominent points whilst lateral incisors and canines presented with approximately 50% non coincidence.
The, overall, high proportions of non-coincident examples found suggest that clinicians should be aware of individual variation and that this may possibly effect 3rd order alignment.

