All published articles of this journal are available on ScienceDirect.

Evaluation and Gender Base Comparison of Single-Root Canal Treatment Performance by Clinical-Phase Dental Students Using an Analytic Rubric System
Authors Info & Affiliations
Abstract
Introduction
This study aimed to determine the effect of gender on the performance of a summative assessment of a nonsurgical Root Canal Treatment (RCT) on single-rooted teeth. Additionally, the association between Cumulative Grade Point Averages (CGPA) and performance was also evaluated.
Methods
A total of 74 fifth-year dental students (31 males and 43 females) were evaluated by two examiners using a calibrated analytic rubric. The scoring system included a 4-point scale (36 points) for examination/diagnosis and clinical steps, and a 5-point scale (15 points) for chairside oral parameters. For the different rubric parameters, the descriptive statistics were calculated, and following that, a pairwise test, as an independent t-test, was performed to compare the rubric scores between student groups and examiners. The reliability of the rubric was assessed using the Intraclass Correlation Coefficient (ICC). Furthermore, Pearson's correlation coefficient tests analyzed the associations between CGPA, examiners, and RCT performance scores.
Results
Results revealed nearly identical overall scores (43.375/42.720) for males and females, with no statistically significant differences in any evaluated parameters or examiner assessments (p ≥ 0.050). Inter-examiner reliability, measured using the ICC, was excellent, with values ranging from 0.75 to 0.86 across all parameters. A strong positive correlation was found between students' GPAs and their performance in specific assessment criteria (p = 0.001).
Discussion
The findings indicate that gender does not significantly influence dental students' performance in nonsurgical root canal treatment of single-canal teeth, as assessed using a calibrated analytic rubric. High inter-examiner reliability and a strong positive correlation between cumulative GPA and performance scores suggest that academic achievement may be a better predictor of clinical competency than gender.
Conclusion
Male and female dental students demonstrated comparable, consistently high performance across most evaluation criteria for single-canal RCTs. Their performance scores showed a positive correlation with their CGPAs, and the evaluations by both examiners were consistent and reliable.
1. INTRODUCTION
Undergraduate dental students acquire theoretical and hands-on knowledge of RCTs during preclinical and clinical endodontic courses, which helps them accurately screen and diagnose patients and manage clinical practice [1]. To pass these courses, students in both phases are regularly required to complete a specified number of cases and successfully undergo competency assessments and examinations [2]. This process ensures that preclinical and clinical students have developed the skills necessary to perform RCTs, thereby increasing their self-confidence [3]. As future dentists, these students must deliver the highest caliber of RCT to provide optimal patient care [4, 5].
In developing countries, most patients receive RCT from general practitioners' dental clinics [6]. Regularly assessing the clinical outcomes of RCTs conducted by dental students in the clinical phase will improve the quality of dental education and students' clinical performance [7]. Traditional methods of evaluating student performance have relied on visual grading methods, often expressed as individual marks or subdivided numerical scores [8]. However, clinical endodontic courses require a more objective approach, with multiple faculty examiners to ensure fair evaluations [9]. The valuation steps and techniques should exhibit validity, effectiveness, efficiency, and reliability to maintain consistency and standardization among examiners. Additionally, both the evaluator and the student should have a clear understanding of the assessment's objectives [10]. Evaluations should also provide detailed and constructive feedback, allowing students to reflect on and improve their performance [11].
The American Dental Education Association mentions several assessment systems utilized to capably assess clinical skills and competence, aiming to develop the skills desired for proper and active clinical services and clinical practice [12]. Rating scales and checklists are commonly employed, although their benefits and drawbacks are subject to ongoing debate [13]. In medical education, universal rating scales are designed to measure learners’ proficiency across diverse skills, typically requiring assessors to provide an overall numerical score [14]. Checklists use binary choices to specify undergraduate performance against predefined measures [15]. These tools are favored in higher education due to their lack of special equipment requirements and their adaptability in scheduling assessments [16]. However, these traditional assessment methods lack objective statements and point scales, leading to problems such as examiner subjectivity, insufficient meaningful feedback, and confusion among students [17]. The evaluation tool should include clear criteria for each grading component in the quality assessment, providing solid rules for examiners and immediate feedback for learners [18].
One currently used assessment tool is rubrics, defined as “scaled instruments with achievement levels and specific criteria arranged in a grid format” [3, 11, 19]. Rubrics create clear guidelines for assessment, outline the principles for performance, and offer faculty rules for standardizing the grading method [3]. By using rubrics, students can better understand the basis of their grades and pinpoint areas needing improvement. The benefits of rubrics include enhancing instructional clarity, improving grading efficiency, and fostering consistency in scoring [20]. They also improve the quality of undergraduate work by clearly outlining expected standards, thereby shifting evaluation from a subjective to an objective process [21]. While rubrics are not a concept, their implementation remains limited in many dental education institutions [22].
Educational factors such as socioeconomic, academic, cultural, and gender are associated with CGPA. In particular, gender has been widely studied, but the results vary. No significant difference in grades between genders was documented among Japanese dental students [23, 24]. Further studies suggest that males often overestimate their performance compared to females [25, 26]. Recently, a study stated that females achieved slightly higher than males in clinical restorative courses [27]. In contrast, other studies documented no gender-significant differences among dental students performing preclinical single-crown preparation, single RCT, and clinical all-ceramic preparations. Similarly, CGPA had a weak relationship with clinical and preclinical performance in both genders [28-30].
The use of rubrics in assessing student performance across different specialties of dentistry programs seems to be limited. Earlier studies have recognized the use of rubrics for assessing students' performance in preclinical endodontic steps and courses [18, 20, 22, 31], conservative dentistry courses [27, 32], single prosthesis preparation steps [33], and oral presentations in orthodontics [34] and periodontics [35]. However, research on applying rubrics to evaluate and assess clinical single-canal RCTs is lacking.
The clinical endodontic course at the College of Dentistry, Jazan University (CODJU), Saudi Arabia (SA), takes place during the 5th year of the curriculum and consists of 4 credit hours for theory and clinic session training (1 and 3 hours). Over the duration of this course, students attend 33 theory lectures and contribute to an equivalent number of 3-hour clinical sessions. During the clinical exercise, students in the clinical phase perform RCT steps according to meticulously designed analytic rubrics for anterior and posterior single or multirooted teeth. Their faculty supervisors closely supervise these different steps and their parameter outcomes at each stage of the treatment plan by using the analytic rubrics for each dental procedure.
There are few clinical studies on using rubrics to assess single-canal RCT performed by undergraduate dental students. To investigate this, a literature search (PubMed, Scopus, Web of Science) was conducted up to August 2023, using terms like rubric, endodontic, and clinical assessment. Our criteria included original studies of clinical-phase dental students performing RCTs with rubrics, published in English. The findings indicate a scarcity of research on the application of rubrics for evaluating clinical competency in RCTs, particularly in live clinical settings.
This study, therefore, utilized an analytic rubric to assess single-canal RCT performance among clinical phase dental students at CODJU, SA. The assessment was conducted at the final clinical exams at the end of the second semester of the 2022/2023 academic year. Gender differences were evaluated, inter-examiner reliability and CGPAs were calculated. The null hypothesis is that there will be no significant gender differences in performance among the clinical dental students of the CODJU, SA, who completed a single-canal RCT at the end of the academic year. Additionally, differences in CGPAs did not result in significant differences in total rubric scores among students.
2. MATERIALS AND METHODS
2.1. Study Design and Ethical Approval
This cross-sectional study was conducted in the Department of Restorative Dental Sciences at CODJU, SA, involving all 5th-year dental students during the 2022-2023 academic year in the clinical phase. This study was conducted in accordance with the Helsinki Declaration. Ethical approval was gained from the College of Dentistry's Ethical Committee (Code: CODJU-2321F) on August 21, 2023, and by Jazan University's Standing Committee for Scientific Research (Approval No. REC-45/03/761) on September 22, 2023. All the 74 dental students (31 males and 43 females) registered in the 5th-year clinical endodontic course were included without exclusion based on gender distribution. Two male faculty members with similar teaching and assessment experience in clinical endodontics participated.
2.2. Study and Investigation Type
This cross-sectional study evaluated the performance of clinical-phase dental students in conducting a single root RCT as part of their final academic year clinical exam, carried out during the last week of the semester, to meet clinical requirements. After the treatment, a few chairside oral questions were also asked. The enrolled students were informed about the exam requirements and the rubric criteria used for evaluation. Additionally, they received training on a similar procedure earlier in the academic year to prepare for this step.
2.3. Inclusion and Exclusion Criteria
The study included consistent students of both genders who had completed and finalized their clinical course requirements and were eligible to take their final clinical exam. For the RCT, the criteria required a single canal in an anterior tooth in either the maxillary or mandibular arch, anterior or posterior. Students who required assistance from others, altered the prepared canal tooth, or failed to complete the exam exercise within the allotted time were excluded. Teeth with calcification, severe root curvature, an open apex, or those previously initiated or treated were not accepted for the exam. The whole time allowed for the clinical exercise was 3 hours. After completing the tasks, the two examiners collected, numbered, and graded the rubric evaluation sheets.
2.4. Cases Selections
The diagnostic department initially screened all cases based on specific requirements and instructions from the endodontic division and course coordinator. All selected teeth had to be ready for RCT and periodontally treated, restored, and rebuilt to the entire contour anatomy.
2.5. Rubric Scoring and Data Processing
An analytic rubric was used to assess the clinical performance of dental students in completing a single-canal RCT. The analytic rubric was developed and refined by a panel of endodontic faculty experts at CODJU to ensure content validity, aligning its criteria with the learning objectives of the clinical endodontic course. The evaluation was conducted by two examiners with nearly equivalent teaching experience who were familiar with the rubric criteria and had further training before the assessment. The examiners independently graded the students' performance immediately after the clinical examination, ensuring that evaluations were conducted individually and not in groups. The examiners were blinded to the students' CGPAs throughout the assessment process. The allocated time for the exercise was segmented into diagnosis and treatment planning, the RCT procedure, and the chairside oral exam.
As shown in Table 1, the analytic rubric employed in this research utilized a 4-point scale assessing two parameters (examination and diagnosis, root canal treatment and instrumentation) and a 5-point scale for one parameter (chairside oral evaluation) of a single canal tooth. The scoring of the assessed three parameters was as follows:
| Steps | Level of Achievement (Criteria) | Rating | Obtained Score |
|---|---|---|---|
| Examination and diagnosis | |||
| Case History and Clinical Examination | 1. Chief complaint, 2. History of present illness, 3. Past dental and medical history, 4. An accurately interpret radiographs. | Excellent (4) | |
| When the participant reaches 75% out of all criteria | Good (3) | ||
| When the participant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the participant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Diagnosis and Treatment Plan | 1. Accurately perform the diagnostic tests, 2. Make a proper differential and final diagnosis, 3. An assess etiology and prognosis, 4. Make a correct treatment plan. | Excellent (4) | |
| When the applicant reaches 75% out of all criteria | Good (3) | ||
| When the applicant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the applicant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Total grade gained | 8 points | ||
| Root canal treatment and instrumentation | |||
| Patient / Operator Positioning and Instrument | 1. Proper dentist and patient's chair site, 2. Proper instrument setup, arrangement, and management, 3. Measures taken for the safety of the patient, 4. Proper infection control and disposal of waste. | Excellent (4) | |
| The student achieves up to 75% out of all criteria | Good (3) | ||
| The student achieves up to 50% out of all criteria | Satisfactory (2) | ||
| The student achieves up to 25% out of all criteria | Unsatisfactory (1) | ||
| Isolation and Local Anesthesia | 1. Proper and effective local anesthesia injection, 2. Proper rubber dam clamp selection, 3. Proper site for hole and frame, 4. Achieve a perfect rubber dam seal. | Excellent (4) | |
| When the participant reaches 75% out of all criteria | Good (3) | ||
| When the participant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the participant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Access Cavity Preparation | 1. Remove all caries and build the crown if required, 2. use a proper outline form, 3. de-roof the pulp chamber, and 4. achieve straight-line access to all canals without any iatrogenic error. | Excellent (4) | |
| When the applicant reaches 75% out of all criteria | Good (3) | ||
| When the applicant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the applicant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Working Length Determination | 1. estimate proper Wl from preoperative radiographs, 2. select the properly fitting initial file, 3. determine Wl with apex locater, and 4. finalize the Wl with proper Wl radiographs. | Excellent (4) | |
| When the applicant reaches 75% out of all criteria | Good (3) | ||
| When the applicant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the applicant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Shaping and Cleaning | 1. Determine an accurate master apical file, 2. achieve smooth canal walls and proper canal taper, 3. canal shape reflects natural anatomy with proper apical stop, and 4. proper canal disinfection by proper irrigation protocol. | Excellent (4) | |
| When the participant reaches 75% out of all criteria | Good (3) | ||
| When the participant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the participant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Preparation for Obturation | 1. Select the master cone with proper tug back and length 2. proper master cone radiograph 3. properly mix and handle the sealer 4. Correctly select the spreader, 1-2mm short of Wl., and the accessory cones correspond to the size of the spreader. |
Excellent (4) | |
| When the participant reaches 75% out of all criteria | Good (3) | ||
| When the participant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the participant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Obturation | 1. Students perform obturation at the proper Working length, 2. Homogenous obturation without any voids by using a post-obturation radiograph, and 3. An excess gutta-percha and sealer removal from the pulp chamber, 4. Proper sealing of the coronal part of the root canal with restoration. |
Excellent (4) | |
| When the applicant reaches 75% out of all criteria | Good (3) | ||
| When the applicant reaches 50% out of all criteria | Satisfactory (2) | ||
| When the applicant reaches 25% or less of all criteria | Unsatisfactory (1) | ||
| Total grade gained | 28 points | ||
| Chairside oral evaluation | |||
| Clarity and Fluency | Participant answers and communications for RCTs were clear and comprehensible. | Excellent (5) | |
| Applicant answers and communications for RCTs were sometimes awkward but always understandable. | Good (4) | ||
| Participants' answers and communications in RCTs were awkward and sometimes incomprehensible. | Average (3) | ||
| All answers and communications for RCTs were awkward and incomprehensible. | Poor (2) | ||
| All answers were unclear. | Unsatisfactory (1) | ||
| Evidence and structure | Presents evidence and ideas that are relevant and accurate to RCT steps and ideas with logic behind it. | Excellent (5) | |
| Presents evidence that is relevant primarily and/or mostly accurate to RCT steps, and ideas that mostly have logic | Good (4) | ||
| Presents somewhat inaccurate and/or irrelevant evidence to RCT steps, but corrects when prompted. Ideas do not always flow logically, making them difficult to follow. | Average (3) | ||
| Presents much inaccurate and/or irrelevant evidence related to RCT steps. Ideas do not flow logically. Hence, the argument is complicated to follow. | Poor (2) | ||
| All answers related to RCT steps were without evidence | Unsatisfactory (1) | ||
| Comprehension and overall understanding | The participant fully understood the questions about the steps performed and answered correctly. Student shows a deep/vigorous, and thoughtful of topic with a completely developed argument. | Excellent (5) | |
| The applicant understood most of the questions related to the steps performed and was asked about them. The applicant shows a limited understanding of the RCT and does not quite have a fully developed argument. | Good (4) | ||
| The participant showed little comprehension of questions about the RCT steps performed. The participant shows a superficial understanding of the subject; the argument is not developed enough. | Average (3) | ||
| The student might not understand the questions about the RCT steps performed, so the questions had to be repetitive. The student shows no understanding of the subject and no argument. | Poor (2) | ||
| No comprehension or understanding of the questions about the steps accomplished was observed. | Unsatisfactory (1) | ||
| Total grade gained | 15 points | ||
Abbreviation: RCT- root canal treatment.
The parameters of examination and diagnosis included case history, clinical examination, diagnosis, and treatment plan. Performance was graded as excellent (4), good (3), satisfactory (2), or unsatisfactory (1), with a maximum total score of 8 points.
The parameters of clinical RCT steps included patient, operator position, and instrument setup, anesthesia and isolation, access, cavity preparation, working length determination, cleaning and shaping, preparation for obturation, and obturation. Performance was graded as excellent (4), good (3), satisfactory (2), or unsatisfactory (1), with a maximum total score of 28 points.
The chairside oral evaluation parameters included clarity and fluency, evidence and structure, comprehension, and overall understanding of all clinical steps concerning RCT. The chairside oral evaluation was conducted using a structured set of questions directly related to the RCT procedure the student had just performed, with scoring guided by the predefined anchors in the rubric. The grading was excellent, good, average, poor, and unsatisfactory, scoring 5, 4, 3, 2, and 1, respectively. The sum (15 points) was calculated for each student.
The analytic rubric was a grid with parameters in the left column, performance levels as numbers, and descriptive tags across the top. The different parameters and related queries were graded independently, and the scores were recorded in the rightmost column. The total of all scores for every parameter was taken as the total score for each undergraduate (Table 1). Printed logbook sheets were used for each undergraduate's clinical case assessment, and the recorded copies were arranged for data processing.
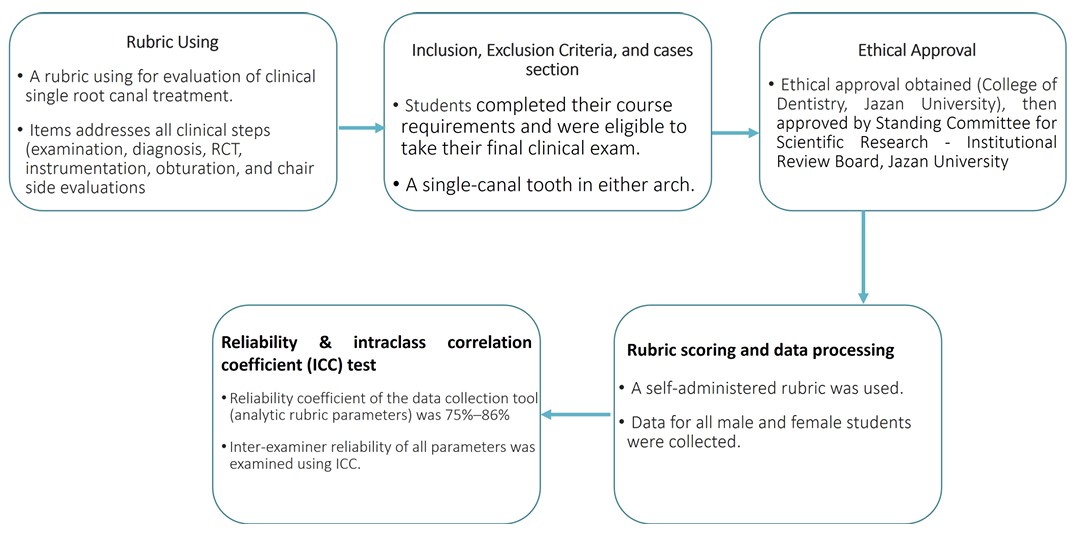
Steps involved in the rubric using and data collections.
2.6. Accumulative Grade Point Average for Students
The students' final CGPAs were obtained from the college's student affairs department. The CODJU uses a 5-point scale for CGPA calculation, represented as 5 (A+), 4.75 (A), 4.5 (B+), 4.0 (B), 3.5 (C+), 3.0 (C), 2.5 (D+), and 2.0 (D) [27-30]. For reporting and correlation analysis, the CGPAs were used as a continuous variable on this 5-point scale.
2.7. Reliability and Intraclass Correlation Coefficient Test
Reliability was calculated using Cronbach's α coefficient, developed by Cronbach in 1951. The results displayed that the overall scale demonstrated internal consistency. The reliability coefficient of the data collection tool (analytic rubric parameters) was 75%–86%, indicating that the RCT items assessed in the analytic rubric (examination and diagnosis, RCT and instrumentation, and chairside oral evaluation) were internally consistent. The inter-examiner reliability of all parameters was examined using the ICC. A two-way random-effects model for absolute agreement ICC (2,1) was used.
Figure 1 shows the flow chart involved in the case selection and clinical RCT steps. The collected rubric data were received from the participants, then numbered and arranged in an Excel sheet for statistical analysis.
2.8. Statistical Analysis
SPSS version 26.0 (SPSS, Inc., Chicago, IL, USA) was used for statistical analysis. The Shapiro-Wilk test indicated no significant deviation from normality (p ≥ 0.05). Parametric tests (t-tests, Pearson correlation) were applied as the data approximated a normal distribution and were treated as continuous for enhanced analytical power. Descriptive statistics included means and standard deviations for scores from two examiners and the different parameters of a single RCT. An Independent T-test examined gender differences in rubric scores, while Pearson correlation analysis was used to assess the association between CGPA and the outcome of a single RCT and between CGPA and overall rubric scores calculated by the two examiners. Interobserver reliability was tested using ICC (2,1). Although multiple comparisons raise Type I error concerns, p-values are reported without adjustment to allow for transparency in interpretation, with significance set at P<0.05.
3. RESULTS
This study analyzed the parameters of the analytic rubric for a single RCT. In a clinical endodontics course, two male examiners assessed three parameters for a total of 74 fifth-year dental students (31 males and 43 females). Concerning the CGPA of the students, for males (n=31), there were 4 A’s, 17 B+’s, 8 B, and 2 C+, respectively, while it was 10 A’s, 23 B+’s, 9 B, and 1 C+, respectively, for females.
The ICC was over 0.70, which is considered good and high according to the ICC criteria. The rubric parameters of examination and diagnosis, RCT and instrumentation, and chairside oral evaluation had ICC values of 0.75 (95% CI: 0.63--0.83), 0.86 (95% CI: 0.79--0.91), and 0.77 (95% CI: 0.66--0.85), respectively. All three parameters exhibited excellent interexaminer reliability.
Descriptive statistics for the scores are presented in Table 2. The mean and SD for males and females were similar, receiving a good (3/4) rating from the two examiners. For the examination and diagnosis step, the mean scores for values were 3.612 (0.558) and 3.372 (0.489) for case history with clinical examination and 3.741 (0.514) and 3.558 (0.665) for diagnosis with the treatment plan, with no significant differences (p-values 0.561 and 0.485) (Table 2).
Concerning RCT and instrumentation steps (patient, operator position, and instrument; anesthesia and isolation; access cavity preparation; working length determination; cleaning and shaping, preparation for obturation, and obturation) for both genders, there are no statistically significant differences in all parameters between evaluator 1 and 2 (all p-values > 0.05) (Table 2). Similarly, between the two evaluators, the chairside oral evaluation parameters (comprehension and overall understanding, evidence and structure, clarity and fluency) recorded no gender significant differences (p-values > 0.05) (Table 2).
Between genders, an independent t-test of the different rubric parameters of the clinical performance for a single RCT (examination and diagnosis, root canal treatment and instrumentation, and chairside oral evaluation) revealed that there are no statistically significant differences in all rubric steps with all p-values > 0.05 (Table 3).
| Rubric Steps | Parameter | Gender | Evaluator (1) Mean ±SD | Evaluator (2) Mean ±SD | P-value |
|---|---|---|---|---|---|
| Examination and diagnosis | Case history and clinical examination | Male | 3.548 (0.623) | 3.612 (0.558) | 0.561 |
| Female | 3.465 (0.591) | 3.372 (0.489) | |||
| Diagnosis and treatment plan | Male | 3.741 (0.514) | 3.613 (0.667) | 0.485 | |
| Female | 3.651 (0.572) | 3.558 (0.665) | |||
| Root canal treatment and instrumentation | Patient, operator position, and instruments set up | Male | 3.355 (0.608) | 3.354 (0.709) | 0.270 |
| Female | 3.512 (0.592) | 3.372 (0.578) | |||
| Anesthesia and isolation | Male | 3.516 (0.570) | 3.452 (0.723) | 0.975 | |
| Female | 3.512 (0.631) | 3.395 (0.660) | |||
| Access cavity preparation | Male | 3.355 (0.755) | 3.290 (0.864) | 0.972 | |
| Female | 3.348 (0.663) | 3.419 (0.663) | |||
| Working length determination | Male | 3.516 (0.570) | 3.548 (0.568) | 0.107 | |
| Female | 3.721 (0.503) | 3.674 (0.522) | |||
| Cleaning and shaping | Male | 3.581 (0.501) | 3.677 (0.475) | 0.196 | |
| Female | 3.419 (0.548) | 3.372 (0.535) | |||
| Preparation for obturation | Male | 3.581 (0.512) | 3.581 (0.564) | 0.110 | |
| Female | 3.372 (0.578) | 3.325 (0.558) | |||
| Obturation | Male | 3.354 (0.660) | 3.419 (0.564) | 0.328 | |
| Female | 3.488 (0.505) | 3.488 (0.551) | |||
| Chairside oral evaluation | Comprehension and overall understanding | Male | 4.161 (0.522) | 4.162 (0.432) | 0.709 |
| Female | 4.209 (0.559) | 4.225 (0.425) | |||
| Evidence and structure | Male | 3.801 (0.401) | 3.605 (0.497) | 0.057 | |
| Female | 3.604 (0.495) | 3.806 (0.402) | |||
| Clarity and Fluency | Male | 3.709 (0.461) | 3.651 (0.482) | 0.746 | |
| Female | 3.744 (0.441) | 3.774 (0.425) |
| Rubric Step | Gender | Evaluator (1) Mean ±SD | Evaluator (2) Mean ±SD | Overall Average Mean ±SD | Effect Size (Cohen's d) |
|---|---|---|---|---|---|
| Examination and diagnosis | Male | 7.28 (0.851) | 7.22 (0.871) | 7.250 (0.803) | 0.26 |
| Female | 7.12 (1.005) | 6.93 (0.961) | 7.023 (0.919) | ||
| P-value | 0.456 | 0.185 | 0.269 | ||
| Root canal treatment and instrumentation | Male | 24.344 (2.719) | 24.375 (3.149) | 24.359 (2.883) | 0.06 |
| Female | 24.372 (2.299) | 24.046 (2.340) | 24.209 (2.196) | ||
| P-value | 0.961 | 0.606 | 0.799 | ||
| Chairside oral evaluation | Male | 11.72 (1.054) | 11.81 (0.896) | 11.766 (0.924) | 0.30 |
| Female | 11.56 (0.983) | 11.42 (0.982) | 11.488 (0.922) | ||
| P-value | 0.504 | 0.079 | 0.202 |
Regarding the correlations between CGPA, evaluators and students, substantial correlations with CGPA were detected for the chairside oral scores from the second examiner and both examiners (r = 0.772, 0.944, 938 with p = <0.001), the total rubric scores from the first, second, and both examiners (r = 0.747, 0.934, 0.935, and p = <0.001), and the average rubric scores from the first, second, and both examiners (r = 0.863, 0.962, 0.968 and p = <0.001) (Table 4).
4. DISCUSSION
European guidelines emphasize that graduating students should be capable of performing high-quality RCT [36]. Given the technique-sensitive nature of endodontic procedures, comprehensive training and rigorous assessment are essential components of dental education [22]. Undergraduates trained with rubrics may experience enhanced learning, as a well-designed rubric provides a permanent reference for clinical performance guidelines [37]. This effect is attributed to the rubrics' ability to direct students' attention and guide them in recognizing essential steps in clinical procedures, ultimately improving their performance in a clinical setting [18]. This study used an analytic rubric to assess the single RCT performance of dental students at the clinical phase in the CODJU, SA.
The selection of an analytic rubric for this study was predicated on its potential to provide more detailed, criterion-specific feedback and enhance grading consistency compared to traditional checklists or global rating scales, thereby offering a more objective and instructive assessment tool for complex clinical procedures [17, 19]. Differences in raters' judgments can arise between raters (interrater reliability) or within a single rater across different occasions evaluating the same procedure (intrarater reliability) [38]. The results of the current study displayed that the two examiners demonstrated excellent interexaminer reliability for the tested parameters, with ICC values of 0.75, 0.86, and 0.77 for examination and diagnosis, RCT and instrumentation, and chairside oral evaluation, respectively. This value was higher than the 0.53 reported earlier [38, 39]. Meanwhile, the interexaminer reliability values above 0.70 were considered sufficient according to the criteria established prior [40]. However, the present study did not investigate intrarater reliability because the evaluation of the exam steps cannot be repeated after the treatment is completed. The distinct advantage of rubrics is that they offer performance explanations for each criterion at different success steps, points, and stages [3].
The interface between treatment and gender concerning rubric use remains unclear. Some studies found that using rubrics can affect males and females differently, with females reporting higher self-efficacy [26]. However, the results of the current study indicated no significant differences in the analytic rubric parameters concerning the students' gender and scores from the examiners (Tables 3 and 4). Hence, the null hypothesis was accepted for the first part of the study. This aligns with Liang et al.'s study involving Japanese dental students, which also found no significant gender-based differences in grading [23]. In addition, Panadero et al.'s meta-analysis revealed no such general effect of gender on student performance when utilizing analytic rubrics [37]. However, evidence from the US indicated that male students tend to overestimate their abilities compared to female counterparts, leading to more significant differences in grading scores between genders [25]. Recent studies documented that females performed slightly better than males in preclinical and clinical courses [27-30].
Rubric performance levels are characteristically described using qualitative adjectives that define the grade of achievement, offering consistent, aim assessment and response and reaction to undergraduates on their anticipated performance [31, 33]. The number of levels in a rubric can influence agreement among examiners, with fewer levels generally increasing inter-rater consensus. In the present study, the use of five distinct performance levels allows for a more comprehensive evaluation, moving beyond a simplistic pass/fail or good/poor distinction and aligning closely with the intended learning standards. Such clarity not only helps students grasp the criteria for success but also supports evaluators in delivering targeted, constructive feedback [18]. When learners are familiar with the rubric’s requirements, they are better equipped to self-assess and identify specific areas for improvement.
The strong positive correlations between CGPA and rubric scores (r ≈ 0.9) indicate that students with strong academic records tend to perform equally well in structured clinical evaluations. Importantly, this relationship remains intact despite the clinical assessment being a separate exercise that did not contribute to the students' CGPA, mitigating one source of direct contamination. This strong association underscores that the rubric may be measuring a general trait of academic/clinical competence rather than a completely independent skill set [41]. Therefore, the null hypothesis for the second part was rejected. This finding suggests that higher-performing students demonstrated better performance and more consistent grading across different examiners. This result contrasts with earlier research that found no significant correlation between instructors' grading and students' final course grades [34]. This discrepancy can be related to the rubric guidelines offered early so that the undergraduates can set their expectations and be guided through the preparation for specific procedures. The supplied rubric has served as an immediate feedback tool for students. Effective feedback encourages students to adopt a deeper approach to their learning and enhances their educational outcomes [42].
Gudipaneni et al. [43] found substantial gender differences in professional competence among dental undergraduates, with males being 91% less likely to demonstrate professionalism than females.
| CGPA | - | CGPA | Chairside Oral, Total Evaluator 1 | Chairside Oral, Total Evaluator 2 | Chairside Oral, Average Evaluator 1 and 2 | Examination & Diagnosis Total Evaluator 1 | Examination & Diagnosis Total Evaluator 2 | Examination & Diagnosis 1 & 2 Average Evaluators | RCT and Instrumentation, Total Evaluator 1 | RCT and Instrumentation, Total Evaluator 2 | RCT and Instrumentation, 1 & 2 Average Evaluators |
|---|---|---|---|---|---|---|---|---|---|---|---|
| - | Pearson Correlation | 1 | |||||||||
| Sig-(2-tails) | --------- | ||||||||||
| Chairside oral, Total Evaluator 1 | Pearson Correlation | 0.354** | 1 | ||||||||
| Sig-(2-tails) | 0.002 | ---------- | |||||||||
| Chairside oral, Total Evaluator 2 | Pearson Correlation | 0.359** | 0.772** | 1 | |||||||
| Sig-(2-tails) | 0.002 | <0.001 | ----------- | ||||||||
| Chairside oral, Total Evaluator 1 & 2 | Pearson Correlation | 0.378** | 0.944** | 0.938** | 1 | ||||||
| Sig-(2-tails) | <0.001 | <0.001 | <0.001 | --------- | |||||||
| Examination & diagnosis, Total Evaluator 1 | Pearson Correlation | 0.298** | 0.729** | 0.701** | 0.760** | 1 | |||||
| Sig-(2-tails) | 0.009 | <0.001 | <0.001 | <0.001 | ---------- | ||||||
| Examination & diagnosis, Total Evaluator 2 | Pearson Correlation | 0.203 | 0.526** | 0.616** | 0.605** | 0.747** | 1 | ||||
| Sig-(2-tails) | 0.081 | <0.001 | <0.001 | <0.001 | <0.001 | ---------- | |||||
| Examination & diagnosis, 1 & 2 Total Evaluators | Pearson Correlation | 0.268* | 0.672** | 0.705** | 0.731** | 0.935** | 0.934** | 1 | |||
| Sig-(2-tails) | 0.020 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | --------- | ||||
| RCT and instrumentation, Total Evaluator 1 | Pearson Correlation | 0.248* | 0.488** | 0.383** | 0.464** | 0.471** | 0.357** | 0.433** | 1 | ||
| Sig-(2-tails) | 0.032 | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ------- | |||
| RCT and instrumentation, Total Evaluator 2 | Pearson Correlation | 0.174 | 0.452** | 0.458** | 0.483** | 0.444** | 0.443** | 0.475** | 0.863** | 1 | |
| Sig-(2-tails) | 0.134 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ------- | ||
| RCT and instrumentation, 1 & 2 Total Evaluators | Pearson Correlation | 0.217 | 0.486** | 0.437** | 0.491** | 0.473** | 0.417** | 0.476** | 0.962** | 0.968** | 1 |
| Sig-(2-tails) | 0.061 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ------- |
Note: ** Correlation is significant at the 0.01 level (2-tailed). * Correlation is significant at the 0.05 level (2-tailed).
They also found that academic performance strongly predicted health promotion skills, with undergraduates with a high CGPA in their theoretical courses being 3.4 times more likely to show competence in this domain than those with a normal CGPA [42]. Similarly, Agou and Imam (2023) reported that final-year dental students with high CGPAs were more likely to achieve better marks and accumulate more points on the final case assessment. Furthermore, their study revealed that female dental undergraduates were more than twice as likely to outperform males in clinical evaluations [44].
This study found significant differences concerning CGPA. Similar works documented significantly large differences between grading scores [25, 26]. Others found no significant difference in CGPA grades between males and females [23, 24]. Saudi female students demonstrated superior performance in clinical restorative courses and rubric presentations compared to males, leading to significant variations in their grades [27-30, 44]. These differences might be associated with potential variables such as self-confidence and motivation.
An analytic rubric usually evaluates the quality of RCT performance at each clinical step. It disperses a numerical grade for each step, allowing students to evaluate their clinical skills and aim for higher scores [45]. The structured nature of rubrics makes them practical tools for improving the accuracy of clinical performance assessments. They provide valuable feedback to male and female students regarding their presentations, facilitating improvement [46]. However, using rubrics can be time-demanding, potentially causing stress for both instructors and students, which may affect the examiner's decision-making and overall performance, ultimately hindering their ability to complete tasks effectively [47, 48].
Further investigation is highly recommended to better understand the relationship between dental students' gender, CGPA, and the application of rubrics as assessment tools. Future studies should explore how combining rubrics with self- and peer-assessment activities affects the quality of RCT performed by clinical undergraduates. Additionally, comparative analyses are suggested to assess the efficiency of analytic rubric parameters with comparison to other old-style evaluation systems, such as checklists [49], global rating scales [13], structured rating Scales [50], and enhanced personal protective equipment on the student–operator's experience and restorative procedure [51]. Additionally, it is recommended that similar research be conducted across multiple dental schools in Saudi Arabia, either by employing the current rubric or by developing institution-specific versions, with the ultimate goal of creating a standardized analytic rubric applicable to all dental colleges in SA.
Although this work's analytic rubric-based assessment criteria were designed to offer a comprehensive approach for developing and evaluating clinical phase skills in endodontics, certain limitations must be acknowledged. First, it requires specific expertise and resources, which may not be feasible for all mentors and institutions. Second, the study was conducted at a single dental school, limiting the generalizability of the results. Third, while examiners were blinded to students' CGPAs, knowing student identities could introduce bias. Fourth, although the rubric showed high inter-rater reliability, its criterion validity with independent measures of clinical success needs further investigation. Lastly, while high-difficulty cases were excluded, variations among single-canal teeth may confound results. Future research should replicate this study across various dental schools in Saudi Arabia to assess the tool's reliability and validity.
CONCLUSION
All dental students achieved similarly good performance ratings across the parameters of examination and diagnosis, RCT and instrumentation, and chairside oral evaluation for single-canal RCT. No significant differences were found between genders. The analytic rubric used in this study demonstrated high inter-rater reliability within this study's context. Furthermore, the students with higher CGPAs performed better than those with lower CGPAs. Further multi-institutional research is recommended to confirm the broader generalizability of these findings.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: A.J.: Contributed to data collection; A.A.A.M. and R.A.: Performed data analysis and interpretation; R.A.A.: Developed the methodology; A.S.A.: Prepared the original draft; A.A.A.: Contributed to conceptualization; M.M.A.M.: Contributed to writing the paper; and M.I.K.: was responsible for writing, reviewing, and editing. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| RCT | = Root Canal Treatment |
| CGPA | = Cumulative Grade Point Averages |
| ICC | = Intraclass Correlation Coefficient |
| CODJU | = College of Dentistry, Jazan University |
| SD | = Standard Deviation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The current study protocol was approved by the ethical committee of the College of Dentistry, Jazan University, with an ethical approval code CODJU-2321F. Additionally, this ethical approval was granted by the Standing Committee for Scientific Research - Institutional Review Board (IRB) at Jazan University (Approval No. REC-45/03/761).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
CONFLICT OF INTEREST
Dr. Mohammed M Al Moaleem is the Editorial Advisory Board and Dr. Mohmed Isaqali Karobari is the Co-EIC of the journal TODENTJ.
ACKNOWLEDGEMENTS
Declared none.

