All published articles of this journal are available on ScienceDirect.

Forehead Anthropometrics of Jazan Population, Saudi Arabia: A Prospective Analytical Study
Authors Info & Affiliations
Abstract
Introduction
Forehead morphology plays a critical role in craniofacial analysis, with variations influenced by factors such as gender, age, and ethnicity. Understanding these differences is essential for applications in forensic science, anthropology, and aesthetic surgery. This study aimed to analyze variations in forehead measurements across gender, age, occupation, and geographical locations.
Methods
A total of 297 participants (148 males, 149 females) were included in this study. Forehead measurements (M1–M7), superior forehead width (SFH), and lower forehead width (LFH) were recorded as described in previously published studies. Descriptive statistics, one-way ANOVA, and post-hoc Bonferroni tests were conducted to assess associations. The p-value was set to 0.05.
Results
Significant differences were observed in forehead dimensions between males and females (p < .001), with males generally exhibiting larger measurements except for SFH and LFH. A significant difference between the groups for forehead M1, forehead M2, forehead M3, forehead M4, forehead M5, forehead M6, forehead M7, SFH width, and LFH width in relation to gender was observed (p=<.001).
Discussion
This study confirms significant gender-based differences in forehead dimensions, with males exhibiting larger vertical measurements. These findings hold potential applications in forensic identification, cosmetic surgery, and anthropological research.
Conclusion
The analysis demonstrated that males have statistically longer foreheads compared to females. Additionally, these findings provide a foundation for forensic identification, anthropological studies, cosmetic surgeries, and clinical applications in craniofacial analysis.
1. INTRODUCTION
The forehead serves as a critical aesthetic and functional component of the face. It plays an essential role in conveying emotion, establishing age and gender perception, and defining facial harmony. From a clinical standpoint, precise forehead measurements are fundamental in maxillofacial and craniofacial surgery, particularly in gender affirmation surgeries, treatment planning for craniosynostosis, and reconstructive procedures after trauma or congenital anomalies [1]. In recent years, there has been a growing demand for aesthetic procedures involving the forehead, such as augmentation, botulinum toxin injections, and forehead contouring, all of which necessitate accurate knowledge of regional anthropometric norms [2, 3].
The primary characteristics of the female forehead are the lack of a well-defined brow ridge, a more vertical and rounder shape, higher positioned eyebrows, and usually a shorter forehead length, while the male’s forehead is flat and steep, with prominent and robust supraorbital ridges, deep-set orbits, and a high frontal and M-shaped hairline [4]. There are studies across the globe demonstrating the forehead measurement and differences among the gender [4, 5]. Moreover, forehead morphology is highly variable among different ethnic groups, influenced by both genetic ancestry and environmental adaptations. Studies conducted in Western, African, and East Asian populations have demonstrated significant variations in forehead height, width, and curvature [3, 6-10]. Schendel et al. (1995) observed that East Asian populations typically exhibit a broader, flatter forehead than their Caucasian counterparts [11]. However, anthropometric standards developed from European or North American populations may not be suitable for other ethnicities due to inherent or ethnic differences. The Middle Eastern population, which is ethnically diverse and shaped by millennia of migration and admixture, has received relatively limited attention in the field of craniofacial anthropometry [6, 12-14].
There is growing evidence suggesting that craniofacial measurements, including forehead dimensions, can differ significantly within subpopulations in the Middle East due to genetic diversity, tribal endogamy, and regional isolation [14]. Despite this, most existing anthropometric databases used in clinical and forensic settings continue to be based on Western populations. Consequently, the reliance on such data may lead to inaccurate assessments, suboptimal clinical outcomes, or misidentification in forensic cases when applied to Middle Eastern individuals. Establishing region-specific anthropometric norms is thus a scientific imperative.
Previous studies in the Middle East have focused on general craniofacial indices, such as the cephalic index, facial index, or nasal index [6, 12-14]. However, few have isolated the forehead as a primary subject of anthropometric investigation. A recent study by Bayat et al. (2020) on Iranian adults demonstrated sex-based differences in forehead height and inter-frontal breadth, highlighting the need for further population-specific studies [15]. A recent anthropometric study conducted in Riyadh focused on measuring facial and forehead dimensions of Saudi Arabian females [14]. Data on anthropometric measurements by age and gender are limited in Saudi Arabia. Moreover, to date, no study has evaluated forehead measurement differences between males and females, which could help surgeons plan cosmetic surgeries in the Jazan region of Saudi Arabia. Hence, this study aimed to analyze variations in forehead measurements across variables such as gender and age. Moreover, to bridge the gap by conducting a prospective analytical study of forehead anthropometry among the Jazan population, stratified by gender and age group. The specific objectives of this research are threefold: (1) to establish normative data for key forehead dimensions such as forehead height and forehead width; (2) to assess sexual dimorphism in forehead morphology; and (3) to explore correlations between forehead dimensions, gender, and age groups.
2. MATERIALS AND METHODS
After obtaining ethical clearance from Jazan University, College of Dentistry (Ref. No. REC-46/09/1393; Dated on: 04 March 2025) and written informed consent, a total of 297 volunteers (148 males and 149 females) aged 17-35 years were included. The exclusion criteria were facial injuries, congenital facial defects, pre- or post-orthodontic treatment, obvious baldness, and age group below 17 years. The frontal hairline of volunteers was assessed visually and considered acceptable if it was intact and measurable relative to standard anatomical landmarks (Fig. 1). Only participants meeting these criteria were included in the study. The SAGER checklist was used to support the inclusion of gender-based eligibility criteria [16].
The sample size was calculated using G*Power software (Version 3.1.9.7, Universität Düsseldorf, Germany) to ensure adequate statistical power. A priori analysis for a one-way ANOVA (or independent t-test, as appropriate) was performed, with the following assumptions: a medium effect size (f = 0.25), α = 0.05 (two-tailed), and power (1 – β) = 0.80. The analysis indicated that at least 100 participants per group were required to detect statistically significant differences between groups. To account for potential dropouts or missing data, the final sample size was increased by 10%, resulting in a total of 297 participants. The samples were collected for 3 months, from 10th March 2025 to 15th June 2025.
2.1. Anthropometric Measurements
Anthropometry is the measurement of the human body using various instruments. Forehead anthropometric measurements for the current study were conducted in a clinical setting using a non-stretchable, disposable paper ruler (accuracy ±1 mm). Participants included males and females aged 17 to 35 years and older, seated upright with the head in the Frankfurt horizontal plane during assessment. All measurements were carried out under uniform lighting and ambient conditions to minimize variability.
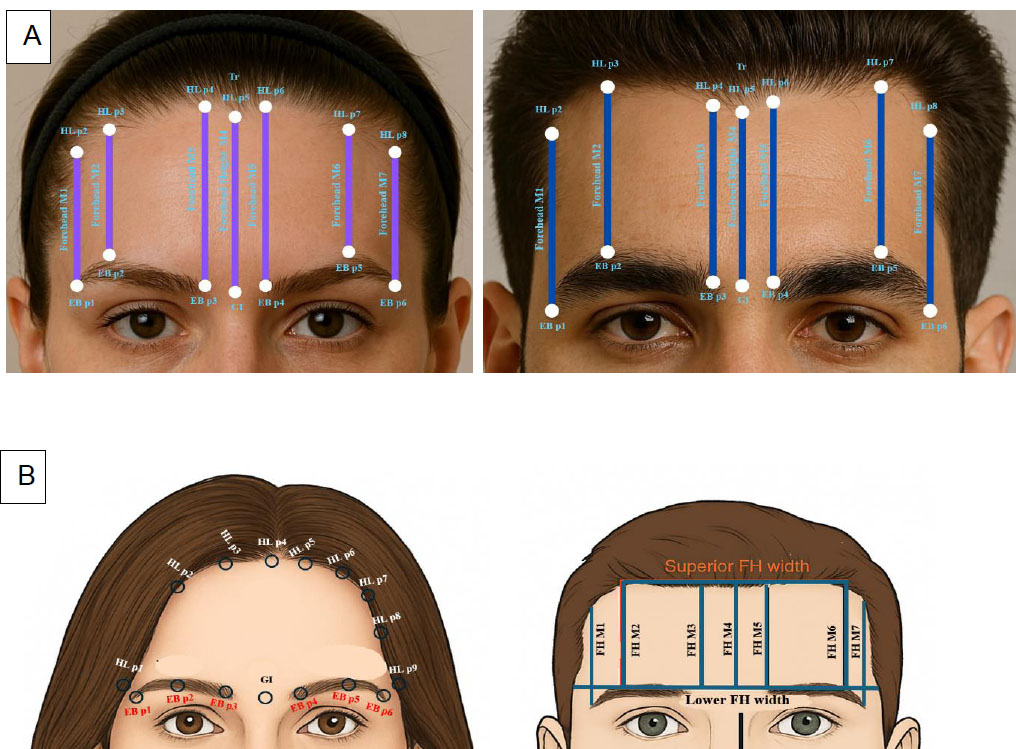
A. Forehead landmarks and measurements of interest. B. Representative frontal and schematic views showing the anthropometric landmarks and measurement points used for forehead height and width analysis in male and female subjects.
2.2. Landmark Definitions and Measurement Technique [17, 18]
A total of six eyebrow (EB) reference points and nine hairline (HL) reference points were identified for the purpose of vertical and horizontal forehead measurement (Fig. 1A and B).
2.2.1. Eyebrow Landmarks
- EB p1 and EB p6 represent the lateral ends of the right and left eyebrows.
- EB p2 and EB p5 denoted the highest points (peaks) of the right and left eyebrows.
- EB p3 and EB p4 corresponded to the medial ends of the right and left eyebrows.
2.2.2. Hairline Landmarks
- HL p1 and HL p9 marked the most lateral points on the right and left sides of the hairline, respectively, aligned horizontally with the glabella and medial eyebrow points (EB p3 and EB p4).
- HL p2 and HL p8 were positioned vertically above the lateral ends of the eyebrows (EB p1 and EB p6).
- HL p3 and HL p7 were aligned vertically above the eyebrow peaks (EB p2 and EB p5).
- HL p4 and HL p6 were vertically aligned with the medial eyebrow ends (EB p3 and EB p4).
- HL p5, also referred to as the trichion, was vertically aligned with the glabella, representing the midpoint of the anterior hairline.
2.3. Forehead Vertical Measurements
Seven vertical forehead heights (FH M1–M7) were measured from the hairline to corresponding eyebrow landmarks (Fig. 1A and B):
- FH M1 and FH M7: Distance from HL p2 to EB p1 and from HL p8 to EB p6, respectively, representing forehead height above the lateral ends of the eyebrows.
- FH M2 and FH M6: Distance from HL p3 to EB p2 and from HL p7 to EB p5, representing forehead height above the eyebrow peaks.
- FH M3 and FH M5: Distance from HL p4 to EB p3 and from HL p6 to EB p4, indicating forehead height above the medial ends of the eyebrows.
- FH M4: Distance from the trichion (HL p5) to the glabella, representing the central forehead height.
2.4. Forehead Width Measurements
- Superior Forehead Width: Distance between HL p3 and HL p7, located above the eyebrow peaks.
- Lower Forehead Width: Distance between HL p1 and HL p9, aligned horizontally with the glabella and medial eyebrow points (EB p3 and EB p4).
2.5. Forehead Region Classification
- Median and Paramedian Forehead Heights: Defined by FH M3, M4, and M5.
- Lateral Forehead Heights: Defined by FH M1, M2, M6, and M7.
Mean values of forehead heights (FH M1 to FH M7) were separately calculated for male and female participants. These values were then applied to standardized eyebrow illustrations to generate average hairline contours for each sex, delineating hairline points above the lateral brow, brow peak, medial brow, and glabellar regions.
2.6. Standardization and Hygiene
Due to the time-consuming nature and precision required for the measurements, an experienced oral and maxillofacial surgeon trained three operators. During the training sessions, each operator was asked to measure their peers' foreheads. Intra- and inter-observer reliability assessments were conducted for all measurements. Initially, during the training period, intra-observer reliability ranged from 0.50 to 0.64, indicating suboptimal consistency. However, after the third training session, both intra- and inter-observer reliability improved significantly, with values ranging from 0.73 to 0.88. Following this improvement, the trained operators performed measurements on the study volunteers. Each measurement was taken three times, and the average value was recorded for analysis. Paper rulers were either single-use or disinfected with 70% isopropyl alcohol among participants to maintain hygiene standards.
2.7. Statistical Analysis
All collected data were entered into a Microsoft Excel spreadsheet and subsequently imported into IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY) for analysis. Descriptive statistics, including means and standard deviations, were computed for all forehead measurements. To assess the distribution and variability of the measurements, Kernel Density Estimation (KDE) curves were generated. To evaluate the association between forehead measurements and demographic variables such as gender, an independent t-test was performed. A p-value of less than 0.05 was considered indicative of statistical significance.
(Top) Clinical photographs depicting the vertical reference lines drawn from eyebrow points (EB p1–p6) to corresponding hairline points (HL p1–p8), representing Forehead M1–M7 segments. The central glabella (Gl) and trichion (Tr) serve as midline reference points.
(Bottom) Illustrations demonstrating the distribution of measurement landmarks for standardized forehead height (FH M1–M7) and width parameters, including superior and lower forehead height widths. These reference points enable reproducible measurement of forehead dimensions for comparative morphometric and gender-based analysis. (Images taken from Photoshop 20.0).
3. RESULTS
Figure 2 presents histograms for each forehead measurement (M1-M7), with the x-axis denoting measurement values and the y-axis indicating frequency. Overlaid Kernel Density Estimation (KDE) curves provide smoothed estimates of the underlying probability density distributions. Measurements M1 to M3 and M7 exhibit moderately symmetric, near-normal distributions, characterized by bell-shaped curves with subtle variations in skewness and kurtosis, and central tendencies ranging between 50 and 70 units. In contrast, M4 displays a right-skewed distribution, with most values clustered between 60 and 80 units and a trailing extension toward higher values, reflecting anatomical variability. Measurements M5 and M6 exhibit leptokurtic distributions, with pronounced peaks and narrow distributions centered at 60–70 units, indicating lower variability and a high degree of consistency within the study population for these forehead dimensions.
Table 1 summarizes the descriptive statistics and p-values for forehead measurement parameters (M1–M7), Superior Forehead Width (SFH), and Lower Forehead Width (LFH), comparing male and female participants. Statistically significant gender differences (p < 0.05) were observed in six of seven forehead measurements: M1, M2, M3, M6, and M7 showed significantly higher mean values in males than in females, suggesting pronounced sexual dimorphism in these forehead parameters. An independent t-test showed a significant difference for M6 (p = 0.001), with male and female means of 62.79 mm and 50.75 mm, respectively. However, M4 and M5 did not show statistically significant sex differences (p = 0.23 and p = 0.18, respectively), indicating potential measurement similarity between sexes in these parameters.
3.1. Forehead Width Measurements
Lower Forehead Width (LFH) showed a statistically significant difference between sexes (p = 0.001), with males having broader lower foreheads (mean = 148.91 mm) than females (mean = 135.97 mm). Superior Forehead Width (SFH) did not differ significantly between sexes (p = 0.223), although females had a slightly higher mean (104.42 mm) compared to males (100.28 mm).
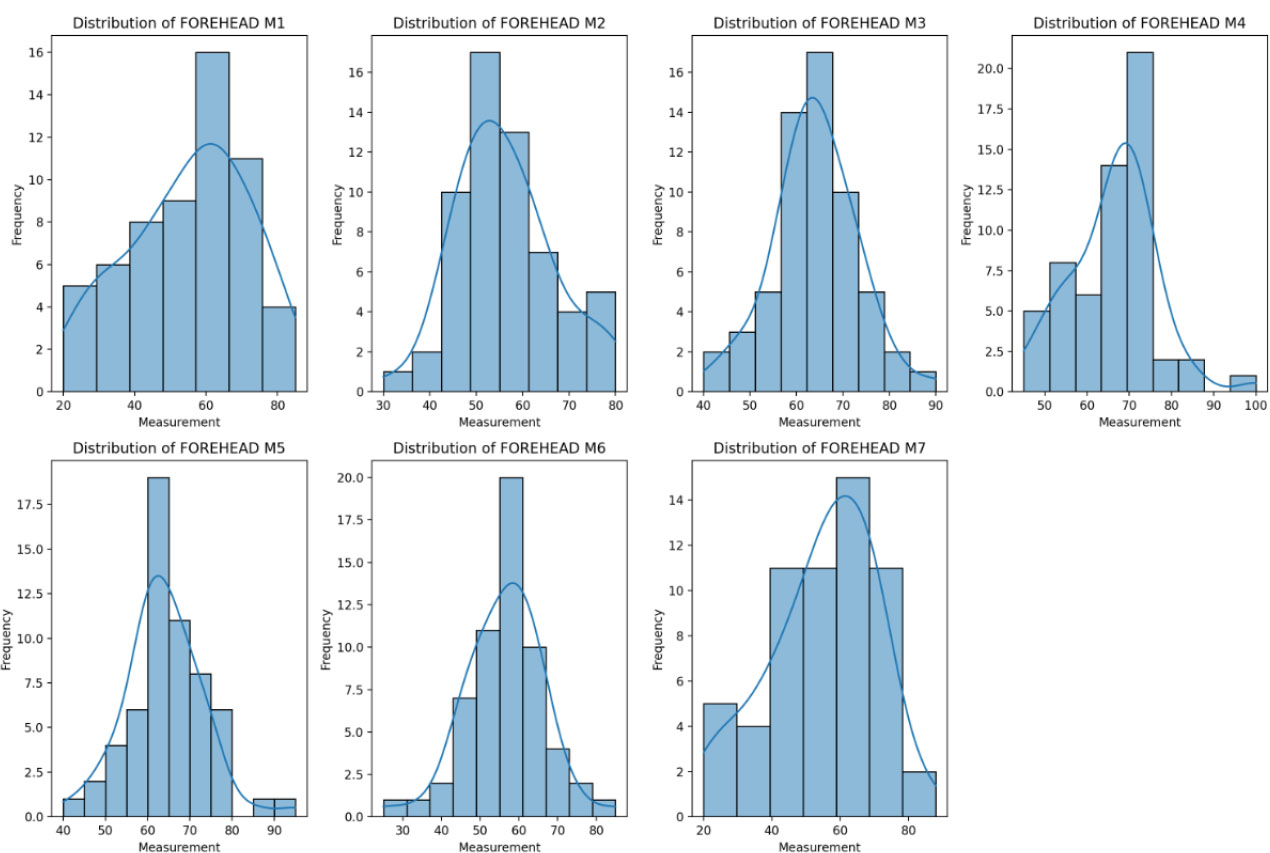
A set of histograms displaying the distribution of measurements for different
| - | - | Number | Mean | Std. Deviation | t-test p-value |
|---|---|---|---|---|---|
| FOREHEAD M1 | Male | 149 | 71.39 | 8.57 | 0.005* |
| - | Female | 148 | 42.59 | 17.11 | |
| FOREHEAD M2 | Male | 149 | 62.88 | 8.08 | 0.002* |
| - | Female | 148 | 50.98 | 12.17 | |
| FOREHEAD M3 | Male | 149 | 67.25 | 7.84 | 0.032 |
| - | Female | 148 | 60.21 | 9.86 | |
| FOREHEAD M4 | Male | 149 | 63.64 | 7.88 | 0.23 |
| - | Female | 148 | 63.27 | 10.25 | |
| FOREHEAD M5 | Male | 149 | 66.61 | 7.87 | 0.18 |
| - | Female | 148 | 59.99 | 9.46 | |
| FOREHEAD M6 | Male | 149 | 62.79 | 8.06 | 0.001* |
| - | Female | 148 | 50.75 | 12.33 | |
| FOREHEAD M7 | Male | 149 | 71.55 | 8.57 | 0.000* |
| - | Female | 148 | 42.78 | 16.53 | |
| SFH WIDTH | Male | 149 | 100.28 | 10.09 | 0.223 |
| - | Female | 148 | 104.42 | 12.78 | |
| LFH WIDTH | Male | 149 | 148.91 | 11.94 | 0.001* |
| - | Female | 148 | 135.97 | 9.92 |
4. DISCUSSION
The present study aimed to establish normative data for forehead anthropometric measurements in the Jazan population of Saudi Arabia, with particular attention to gender and age-related differences. Despite the increasing use of facial anthropometry in clinical, forensic, and aesthetic contexts, the forehead region remains relatively understudied, especially in Middle Eastern populations. Our findings help bridge this gap and provide a foundational reference for clinicians and researchers involved in craniofacial diagnostics and plastic surgery.
4.1. Gender Differences in Forehead Dimensions
One of the most prominent findings of this study was the significant difference in forehead measurements between males and females. Males consistently demonstrated greater forehead heights across all vertical dimensions (M1 to M7) as well as broader horizontal widths both at the superior (SFH width) and lower forehead (LFH width) levels. These differences were statistically significant (p < 0.001), supporting existing evidence that craniofacial dimorphism is prominent in human anatomy. Vertical measurements showed a remarkable degree of gender-specific variation. Lateral forehead height (M1 and M7), paramedian heights (M2 and M6), and medial measurements (M3 and M5) were all significantly greater in males. This likely reflects the influence of hormonal and genetic factors on bone growth and frontal soft tissue thickness. The near-identical central forehead height (M4) between sexes (63.19 mm in females vs. 63.64 mm in males) suggests that while lateral forehead morphology is a strong indicator of sexual dimorphism, the central region remains relatively conserved. These findings are consistent with studies conducted in other ethnic populations. Previous published anthropometric investigations in East Asian and South Asian populations have similarly reported larger forehead dimensions in males, attributable to overall larger craniofacial dimensions and thicker musculocutaneous layers [1, 3, 9, 10, 18-22]. Similarly, a comparative study between American and Asian populations demonstrates higher forehead measurements in males [1]. However, the degree of difference observed in the Saudi cohort may reflect unique regional characteristics and reinforces the importance of population-specific anthropometric data.
The mean central forehead height (M4), measured from the trichion (Tr) to the glabella (Gl), was found to be 63.64 mm among females in the present study. This value closely aligns with previously reported data from studies conducted among female participants residing in Riyadh, indicating consistency in craniofacial dimensions within regional subgroups of the Saudi population. Moreover, a comparative analysis involving various ethnicities documented forehead heights among Middle Eastern females ranging between 60.54 mm and 63.67 mm, which further supports the validity of our findings [6]. These similar values suggest a degree of anatomical stability in central forehead height across the Middle Eastern female demographic, possibly influenced by shared genetic, environmental, and developmental factors.
4.2. Distribution Patterns and Measurement Reliability
The use of Kernel Density Estimation (KDE) curves added value to the analysis by highlighting the distribution of forehead measurements across the population. Most vertical measurements (M1–M3 and M7) followed symmetric, bell-shaped distributions, indicating a central tendency and low skewness. These patterns suggest that these measurements are relatively stable and had less outliers, making them reliable indicators in both clinical and research contexts. In contrast, measurements such as M4 showed right-skewed distributions, with a few participants presenting higher values that could represent anatomical variants or outliers. Similarly, M5 and M6 exhibited leptokurtic (peaked) distributions, reflecting tight clustering around the mean and low variability. These consistent measurements across participants lend themselves well to standardization in clinical applications, particularly in cosmetic planning and reconstructive procedures.
The high intra- and inter-observer reliability achieved following rigorous training sessions also underscores the method's repeatability and accuracy. The use of simple paper rulers, when standardized and appropriately calibrated, proved effective for linear anthropometric analysis in a clinical setting [23, 24]. This low-cost approach is especially advantageous in resource-limited environments and allows broader application in field studies and outreach programs.
4.3. Clinical and Surgical Relevance
Understanding forehead morphology has direct applications in various clinical domains. In craniofacial surgery, precise forehead measurements are crucial for planning procedures such as forehead reduction, contouring, and hairline reconstruction. For example, in gender-affirming facial surgeries, forehead dimensions, particularly height and contour, are key elements in achieving a masculine or feminine appearance [25, 26, 27]. The significantly broader and higher foreheads in males reported in this study provide a guideline for gender-specific surgical outcomes. Moreover, measuring forehead height from trichion to glabella (M4) and across the lateral brow points (M1 and M7) can help determine the ideal position of the anterior hairline during hair transplant procedures [27]. Given the prevalence of androgenic alopecia in the Saudi population, establishing normative forehead dimensions may help clinicians distinguish between natural variation and early signs of pathological recession.
The study’s findings also have value in forensic anthropology, where craniofacial metrics are increasingly used to estimate sex, age, and identity. Forehead dimensions, being relatively robust and less affected by postmortem changes, are ideal for such applications. The significant sexual dimorphism observed in this study can aid forensic experts in narrowing down identity markers during facial reconstruction or in population-specific databases used for biometric facial recognition.
Furthermore, forehead anthropometry can serve as an additional parameter in developing craniofacial models for virtual and augmented reality (VR/AR) applications, particularly for the design of customized headgear, facial interfaces, or ergonomic devices. With growing reliance on AI-powered facial recognition systems in security, healthcare, and personal technology, incorporating accurate, population-specific anthropometric data will enhance algorithmic precision and reduce racial or gender bias in identification.
4.4. Strengths and Limitations
A major strength of this study is the rigorous standardization and training process undertaken before data collection, which resulted in high intra- and inter-observer reliability. The use of a paper ruler-based method demonstrated that reliable anthropometric data can be obtained without expensive equipment, making the methodology replicable across different settings.
However, several limitations should be noted. First, the cross-sectional design limits our ability to assess changes over time or establish causality. Second, while the sample was representative in terms of age and gender, larger sample sizes from different regions of Saudi Arabia would enhance the generalizability of the findings. Third, the authors did not account for variables such as BMI, facial shape classification, or hairline recession status, which may influence forehead dimensions. Future studies incorporating 3D imaging and digital surface analysis may offer more precise insights into topographical features and curvature-based metrics.
4.5. Future Recommendations
Multicenter studies across Saudi Arabia and the broader Middle East can help establish a comprehensive normative database of forehead measurements. Such data can be stratified not only by age and gender but also by ethnicity, geographic origin, and hairline type, which would be valuable for both clinical and forensic applications. Longitudinal studies assessing the evolution of forehead morphology with age, disease, or surgical intervention would offer more dynamic insights. Additionally, future research may explore the relationship between forehead dimensions and psychological or social perception, particularly in cosmetic contexts where facial harmony and attractiveness are central concerns.
CONCLUSION
Forehead anthropometry remains an underexplored yet clinically and technologically significant domain, particularly within ethnically diverse populations such as those in Saudi Arabia. The present study demonstrated that males exhibited significantly greater forehead heights and widths compared to females. These findings underscore the potential utilization of forehead dimensions in various disciplines, including forensic identification, anthropological profiling, craniofacial diagnostics, and aesthetic surgical planning. Future multicenter studies across different regions of Saudi Arabia are recommended to establish normative reference values and to explore the role of forehead height as a predictive marker for frontal hairline recession and for the classification of alopecia subtypes.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: M.M.H.B.: was responsible for study conception and design; A.H.M.: Contributed to the methodology; A.A.Q. and A.H.S.: Carried out data collection; H.H.A. and S.A.J.: Performed the analysis and interpretation of the results; and Y.A.W. and S.E.A.: Prepared the draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| EB p1 and EB p6 | = represent the lateral ends of the right and left eyebrows |
| EB p2 and EB p5 | = denoted the highest points (peaks) of the right and left eyebrows |
| EB p3 and EB p4 | = corresponded to the medial ends of the right and left eyebrows |
| HL p1 and HL p9 | = marked the most lateral points on the right and left sides of the hairline respectively, aligned horizontally with the glabella and medial eyebrow points (EB p3 and EB p4). |
| HL p2 and HL p8 | = were positioned vertically above the lateral ends of the eyebrows (EB p1 and EB p6) |
| HL p3 and HL p7 | = were aligned vertically above the eyebrow peaks (EB p2 and EB p5) |
| HL p4 and HL p6 | = were vertically aligned with the medial eyebrow ends (EB p3 and EB p4) |
| HL p5 | = also referred to as the trichion, was vertically aligned with the glabella, representing the midpoint of the anterior hairline |
| FH M1 and FH M7 | = Distance from HL p2 to EB p1 and from HL p8 to EB p6, respectively, representing forehead height above the lateral ends of the eyebrows |
| FH M2 and FH M6 | = Distance from HL p3 to EB p2 and from HL p7 to EB p5, representing forehead height above the eyebrow peaks |
| FH M3 and FH M5 | = Distance from HL p4 to EB p3 and from HL p6 to EB p4, indicating forehead height above the medial ends of the eyebrows |
| FH M4 | = Distance from the trichion (HL p5) to the glabella, representing the central forehead height |
| SFW | = Superior Forehead Width |
| LFW | = Lower Forehead Width |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical clearance from Jazan University, College of Dentistry (Ref. No.REC-46/09/1393; Dated on: 04 March 2025) was obtained.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the participants and their guardians.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
Declared none.
DISCLOSURE
Patient Consent for Publication: Images used in Figure 1A are taken from the Photoshop mentioned of the models (which requires no copyright permission), and the forehead measurement points are created by the authors using MS PowerPoint.
Image Preparation and Editing: No contrasts or light illumination were used during the image formation.
Figure Legend Clarification: All the images and illustrations used in the study were created by the author.

