All published articles of this journal are available on ScienceDirect.

An In-Vitro Evaluation of Antifungal Efficacy and Tensile Strength of Denture Tissue Conditioner with Indian Turmeric Oil
Authors Info & Affiliations
Abstract
Introduction
Denture tissue conditioners are frequently colonised by Candida albicans, leading to denture stomatitis, because conventional materials lack antifungal activity. Turmeric oil, rich in curcumin, exhibits antifungal activity. This study investigated the effect of turmeric oil on the antifungal activity and tensile strength of denture tissue conditioners.
Methods
The minimum inhibitory concentration (MIC) of turmeric oil against C. albicans was determined using a microbroth dilution assay with each concentration tested in triplicate. Tissue-conditioner samples were prepared with turmeric oil concentrations ranging from 2% to 20% (w/w). A 10% nystatin solution served as the positive control, and the unmodified tissue conditioner as the negative control. Antifungal activity was assessed by agar diffusion on days 1, 7, and 14, and tensile strength was measured using a universal testing machine. Statistical analyses included Friedman, Kruskal-Wallis, and Mann-Whitney U tests, with p < 0.05 considered significant.
Results
The MIC of turmeric oil against C. albicans was 12.5 µg/mL, with antifungal activity increasing at higher concentrations. On day 1, the 20% formulation produced inhibition zones comparable to those of nystatin (23.05 ± 0.12 mm versus 27.04 ± 0.11 mm; p = 0.001). Although antifungal activity persisted for 14 days, activity declined after day 7. Tensile strength in the 20% group rose significantly from 0.086 ± 0.013 MPa on day 1 to 0.191 ± 0.038 MPa on day 14 (p = 0.001), in both control groups.
Discussion
Turmeric oil displayed stronger antifungal activity while maintaining acceptable tensile strength. However, its effectiveness declined over time, indicating that it may offer only short-term protection. As these findings are based on in vitro testing, clinical studies are required to assess the performance of this approach in clinical practice.
Conclusion
A denture tissue conditioner with 20% turmeric oil effectively inhibited C. albicans compared to nystatin. It also maintained good tensile strength, suggesting it could help reduce denture stomatitis.
1. INTRODUCTION
Denture tissue conditioners are placed between the denture base and the supporting oral mucosa to improve the comfort in complete denture wearers, particularly in cases of severe ridge resorption or sensitive mucosa. However, their porous structure facilitates water absorption and microbial colonisation, particularly by Candida albicans, thereby increasing the risk of denture stomatitis [1]. Conventional tissue conditioners offer minimal inherent antifungal protection [2]. To address this, researchers have explored incorporating antifungal agents into conventional materials to limit fungal growth and thereby improve oral health [3].
Several antifungal drugs, including nystatin, chlorhexidine diacetate, itraconazole, miconazole, and ketoconazole, have been incorporated into tissue conditioners. At the minimum inhibitory concentration (MIC), these materials suppress C. albicans without significantly affecting their material properties. However, higher concentrations may compromise mechanical performance; for example, miconazole has been shown to increase surface hardness and reduce cushioning. Additionally, water-induced changes in porosity can weaken mechanical performance and promote microbial colonisation.
Nanoparticles have emerged as a promising alternative to conventional antifungal agents. Metal and metal oxide nanoparticles can disrupt fungal cell membranes, thereby reducing adhesion and biofilm formation [4]. Their effectiveness depends heavily on concentration, as excessive concentrations may adversely affect implant stability and biocompatibility. For example, elevated silver content has led to increased water absorption; conversely, silicon dioxide nanoparticles may increase surface roughness, thereby promoting microbial attachment [5, 6]. Combining functionalized nanoparticles with reinforcing fillers, such as graphene oxide or nano-hydroxyapatite, improves antifungal activity while maintaining mechanical integrity; however, long-term clinical outcomes remain limited [4].
Due to limitations associated with synthetic antifungal and nanoparticles, attention has now shifted toward natural bioactive additives. Essential oils incorporated into tissue conditioners have demonstrated antimicrobial effects against oral pathogens. Several plant-derived oils have been shown to inhibit fungal growth on soft liners, with the additional benefit of lower toxicity and a reduced risk of drug resistance. Compounds such as carvacrol have also been shown to suppress bacterial activity and improve mucosal compatibility [8].
Turmeric has long been used in traditional Asian medicine, and its active compound, curcumin, possesses both antimicrobial and anti-inflammatory properties. Curcumin disrupts fungal cell membranes and reduces C. albicans biofilm formation [9]. It also downregulates HSP90 and Cdr1 activity, further limiting antifungal resistance [10].
Turmeric oil exhibits similar antifungal activity; however, its efficacy when incorporated into tissue conditioners remains unclear. Higher concentrations may increase water absorption and alter elasticity, while lower concentrations may not provide adequate antifungal protection. Therefore, this study aimed to evaluate the effectiveness of tissue conditioners infused with Indian turmeric oil, focusing on antifungal activity against C. albicans and on their physical properties.
The null hypothesis was that the tissue conditioner containing Indian Turmeric oil would show no significant differences in antifungal activity against C. albicans or in physical properties compared with conventional denture tissue conditioners.
2. MATERIALS AND METHODS
2.1. Study Design
This in vitro experimental study was conducted after obtaining ethical approval from the Institutional Ethical Committee (IDS/IEC/2024/PR-134). Although the study did not involve human or animal participants, per institutional mandate, all laboratory work also requires ethical committee approval. This study was performed at the Department of Prosthodontics, Institute of Dental Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Odisha, India, in collaboration with the Centre for Biotechnology (CBT), SOA.
2.2. Sample Size Calculation
The sample size was determined a priori using a standard two-sided two-sample t-test approach. The significance level was set at α = 0.05, and the statistical power was set at 80% (β = 0.20). Based on previously published findings and pilot observations, group sizes of 19 specimens were chosen for tensile strength comparisons (control versus 20% turmeric oil), 5–6 specimens for nystatin comparisons, and 6–8 specimens for antifungal activity testing. Under these parameters, the minimum detectable standardised effect sizes (Cohen’s d) were approximately 0.91 for tensile strength (n = 19 per group), 1.62–1.77 for nystatin (n = 5–6 per group), and 1.40–1.62 for antifungal activity (n = 6–8 per group). By measuring specimens on days 1, 7, and 14, the precision improved while reducing the need for additional samples. Because repeated measures were not incorporated into the calculation, the estimated sample size remained conservative.
2.3. Materials
The materials used in this study included a denture soft liner (GC Soft Liner TM), Sabouraud Dextrose Agar and broth for fungal culture, C. albicans (ATCC strain), and antifungal agents. Nystatin was used at 10% as a pharmacological control, while turmeric oil was tested at concentrations of 2–20% (2%, 4%, 6%, 8%, 10%, 12%, 14%, 16%, 18%, and 20%) as a plant-derived antifungal. Turmeric oil was obtained from 100 g of Curcuma longa rhizomes collected from Kandhamal, Odisha, by hydrodistillation using a Clevenger apparatus for 4 h. The oil yield was calculated on a dry-weight (v/w) basis, and residual moisture was removed using anhydrous sodium sulfate (Na2SO4). The oil was stored at 4°C until use in the preparation of tissue conditioner and in antifungal testing [11, 12].
2.4. Determination of Minimum Inhibitory Concentration
The minimum inhibitory concentration (MIC) of turmeric oil against C. albicans was determined by the broth microdilution method according to CLSI M27-A3 guidelines. A stock solution of turmeric oil (100 mg/mL in DMSO) was prepared and diluted in SDB to obtain concentrations ranging from 25 to 0.048 μg/mL, corresponding to 2–20% w/w. The assay was conducted in 96-well microtiter plates, with each plate receiving 100 μL of sterile SDB, followed by 100 μL of fungal inoculum (estimated 10 x CFU/ml). The test concentration was then added to the same volume. All experiments were performed thrice. Nystatin served as the positive control, while sterile broth served as the negative control. The plates were incubated at 27°C for 48 h, after which 5 μL of 0.5 M 2,3,5-triphenyl tetrazolium chloride (TTC) was added to each well and incubated at 37°C for 30 min. The MIC was defined as the lowest concentration of turmeric oil that showed no visible colour change, indicating inhibition of TTC reduction. It corresponded to ≥90% inhibition of growth relative to the positive control. Spectrophotometric confirmation of MIC was performed at 600 nm [13, 14].
2.5. Assessment of Antifungal Activity
For the antifungal assay, C. albicans was cultured in SDB at 37°C for 8 h, and the resulting suspension was adjusted to a 1.0 McFarland standard (approximately 1.5 × 108 CFU/mL) with sterile saline. Sabouraud Dextrose Agar was poured into Petri dishes to a uniform depth of 4 mm, and 100 μL of the fungal suspension was spread onto the surface to create a lawn culture. Once the agar surface had dried, three wells, 6 mm in diameter and 5 mm deep, were created using a sterile cork borer. The test group consisted of denture soft liners containing turmeric oil at concentrations of 2%- 20%.
A pure denture tissue conditioner was used as the negative control, whereas the positive control consisted of a denture tissue conditioner infused with 10% nystatin. Three wells were prepared: one for the test sample, and the remaining two served as positive and negative controls. Eighty plates(n=80) were prepared, resulting in a total of 240 wells with equal distributions among groups. Incubation was performed at 37°C for 14 days. Antifungal activity was assessed by measuring the mean inhibition zone (MIZ) on day 1, with subsequent measurements on days 7 and 14. Clear zones surrounding the wells were measured using a calibrated digital Vernier calliper in millimetres. All procedures were conducted in a laminar airflow biosafety cabinet under aseptic conditions [13, 14].
2.6. Preparation of Specimens and Tensile Strength Testing
Dumbbell-shaped specimens (33 × 6 × 3 mm) were fabricated using aluminium moulds for tensile strength testing in accordance with ASTM D412 for rubber-like materials. The test groups were prepared as follows: the negative control used a pure denture tissue conditioner; the positive control used a 10% nystatin-infused conditioner; and the test group used a denture tissue conditioner containing the MIC-determined turmeric oil concentration.
After preparation, the mixture was poured into moulds and compressed between glass plates to achieve a uniform thickness. The material was allowed to set for 30 minutes under standardised conditions. A total of seventy-two specimens (n=72) were prepared and eventually allocated across the experimental groups. Any surface irregularities were carefully trimmed, after which the samples were stored in distilled water at 37 °C until further testing. Tensile strength testing was carried out on day 1, with follow-up measurements on days 7 and 14. All tests were performed using a universal testing machine (Instron Model 3366, Instron Corp., UK) equipped with Bluehill software (v2.18.713). Each specimen was mounted in tensile grips and subjected to loading at a crosshead speed of 40mm/min. The maximum load at fracture, recorded in Newtons, was used to calculate tensile strength.
2.7. Statistical Analysis
The data were analysed using SPSS Statistics (version 27.0; IBM Corp., Armonk, NY). Normality was assessed using the Shapiro–Wilk test; however, the data did not meet the normality assumptions. Therefore, non-parametric methods were applied. Antifungal measurements across days 1, 7, and 14 were analysed using Friedman’s test; intergroup differences were examined with the Mann–Whitney U test after Bonferroni correction. The tensile strength data were evaluated over time using Friedman’s test. Group-level comparisons were performed using the Kruskal–Wallis test, with p < 0.05 considered significant.
3. RESULTS
A minimum inhibitory concentration of 12.5 µg/mL was obtained for turmeric oil against C. albicans. Fungal growth decreased with increasing concentrations of turmeric oil in the tissue conditioner (2-20%). No inhibition was observed with the plain tissue conditioner.
3.1. Antifungal Efficacy of Turmeric Oil
In contrast, the positive control (10% nystatin) demonstrated the highest inhibition on Day 1, with a mean zone of 27.04 ± 0.11 mm (Table 1, Fig. 1). Even at 2% turmeric oil, the material produced a measurable zone (9.05 ± 0.119 mm), which was statistically significant compared with the negative control (p = 0.001). Higher concentrations produced proportionally larger inhibition zones, with the 20% turmeric oil group approaching the efficacy of the nystatin group over the observation period (p = 0.001).
| Antifungal-Miz | Day 1 | Day 7 | Day 14 | Friedman's Test Statistic | p | |
|---|---|---|---|---|---|---|
| TC + Nystatin | Mean | 27.04±0.11a | 24.05±0.12 | 23.08±0.15a | 16 | <0.001 |
| Median | 27.05 | 24.05 | 23.05 | |||
| TC + 2% TO | Mean | 9.05±0.119a, b | 7.05±0.119a | 7.05±0.119b | 12.8 | 0.002 |
| Median | 9.05 | 7.05 | 7.05 | |||
| TC + 4% TO | Mean | 11.03±0.103a, b | 8.05±0.119a | 8.05±0.119b | 13.71 | 0.001 |
| Median | 11 | 8.05 | 8.05 | |||
| TC + 6% TO | Mean | 12.03±0.103a, b | 10.05±0.119a | 10.05±0.119b | 13.31 | 0.001 |
| Median | 12 | 10.05 | 10.05 | |||
| TC + + 8% TO | Mean | 13.05±0.119a, b | 11.05±0.119a | 11.05±0.119b | 13.31 | 0.001 |
| Median | 13.05 | 11.05 | 11.05 | |||
| TC + 10% TO | Mean | 15.03±0.118a | 13.05±0.119 | 12.05±0.119a | 16 | <0.001 |
| Median | 15 | 13.05 | 12.05 | |||
| TC + 12% TO | Mean | 17.05±0.119a, b | 16.05±0.119a | 16.05±0.119b | 13.71 | 0.001 |
| Median | 17.05 | 16.05 | 16.05 | |||
| TC + 14% TO | Mean | 18.05±0.119a, b | 17.05±0.119a | 17.07±0.104b | 13.71 | 0.001 |
| Median | 18.05 | 17.05 | 17.1 | |||
| TC + 16% TO | Mean | 20.05±0.093a, b | 18.05±0.119a | 18.05±0.119b | 13.06 | 0.001 |
| Median | 20.05 | 18.05 | 18.05 | |||
| TC + 18% TO | Mean | 21.06±0.119a | 19.05±0.119 | 18.06±0.13a | 16 | <0.001 |
| Median | 21.05 | 19.05 | 18.05 | |||
| TC + 20% TO | Mean | 23.05±0.119a | 20.06±0.13 | 19.05±0.119a | 16 | <0.001 |
| Median | 23.05 | 20.05 | 19.05 | |||
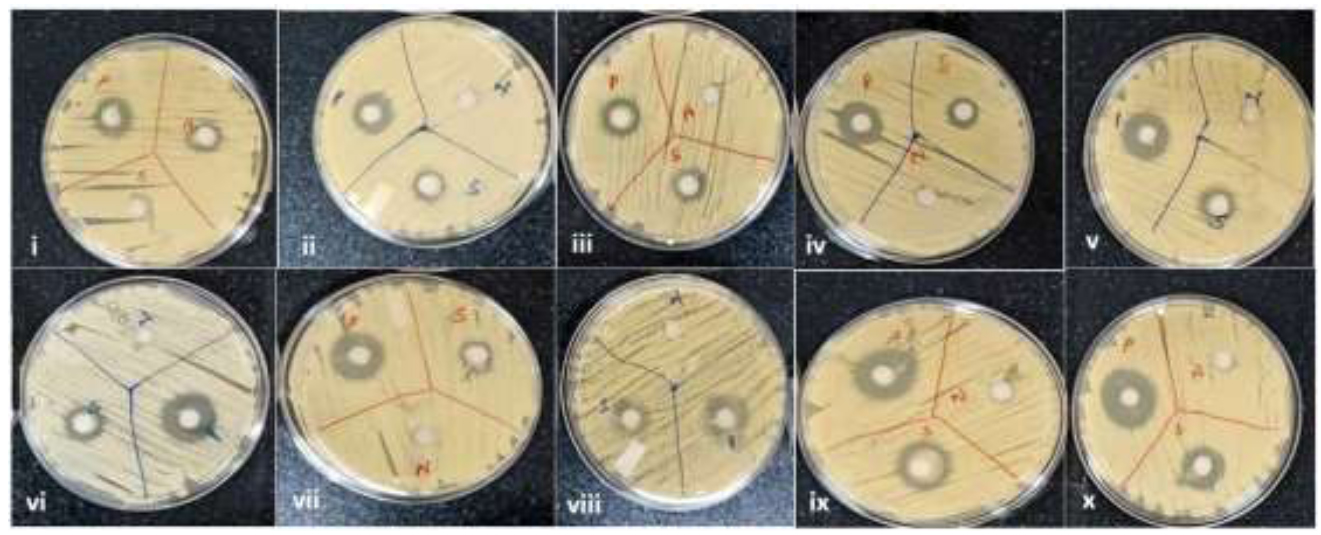
Agar diffusion plates after 24 h showing antifungal activity of turmeric-oil-incorporated tissue conditioner (2–20% w/w) against Candida albicans. Inhibition zones were observed in the test and positive control groups.
3.2. Changes in Antifungal Activity with Time
All groups showed a gradual reduction in antifungal activity over time, which was statistically significant (Friedman test, p < 0.001). On Day 1, both the nystatin and 20% turmeric oil groups showed the widest inhibition zones (Table 2). By Day 7, the zones were smaller, although the relative order of activity across groups remained unchanged (Fig. 2). By Day 14, antifungal effects had further declined, consistent with reduced drug release from the material (Fig. 3). Notably, the 20% turmeric oil group retained activity comparable to that of nystatin even on day 14, whereas lower concentrations (2% and 5%) exhibited a marked loss of efficacy by the second week (Table 1). The MIC assay results that established the inhibitory concentration of turmeric oil (12.5 µg/mL) are shown in Fig. (4).
| Tensile Strength | Day 1 | Day 7 | Day 14 | Friedman's Test Statistic | p | |
|---|---|---|---|---|---|---|
| Tissue conditioner | Mean | 0.061±0.036 | 0.06±0.017 | 0.071±0.018 | 2.86 | 0.24 |
| Median | 0.05 | 0.06 | 0.07 | |||
| Tissue conditioner + turmeric oil |
Mean | 0.086±0.013a, b | 0.168±0.032a | 0.191±0.038b | 13.86 | 0.001 |
| Median | 0.085 | 0.18 | 0.185 | |||
| Tissue conditioner + nystatin |
Mean | 0.175±0.043a | 0.076±0.021a, b | 0.156±0.046b | 9.25 | 0.01 |
| Median | 0.16 | 0.08 | 0.165 | |||
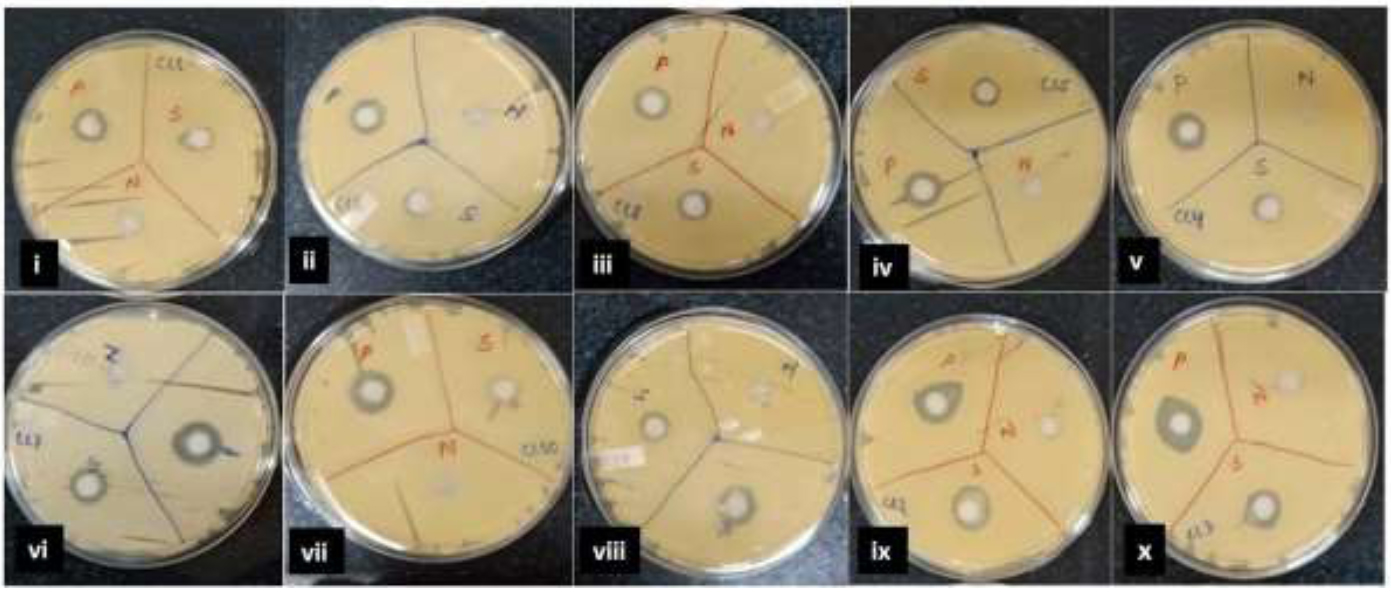
Agar diffusion plates after 7 days showing antifungal zones of turmeric oil-incorporated tissue conditioner (2–20% w/w).
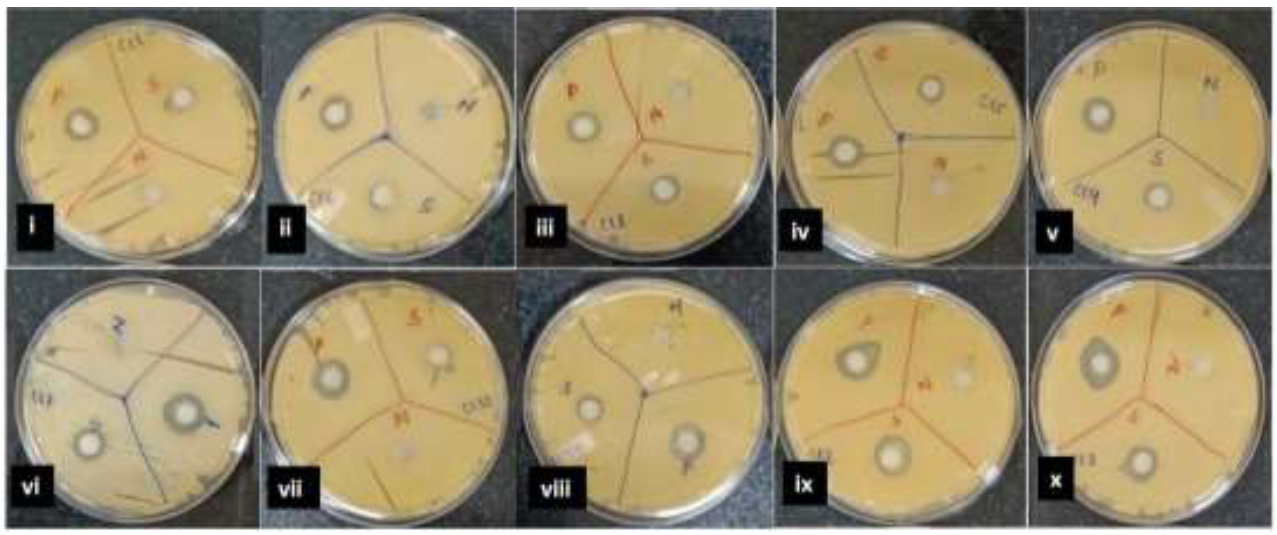
After 14 days, agar diffusion plates showed reduced zones at lower concentrations, and the 20% group retained activity.
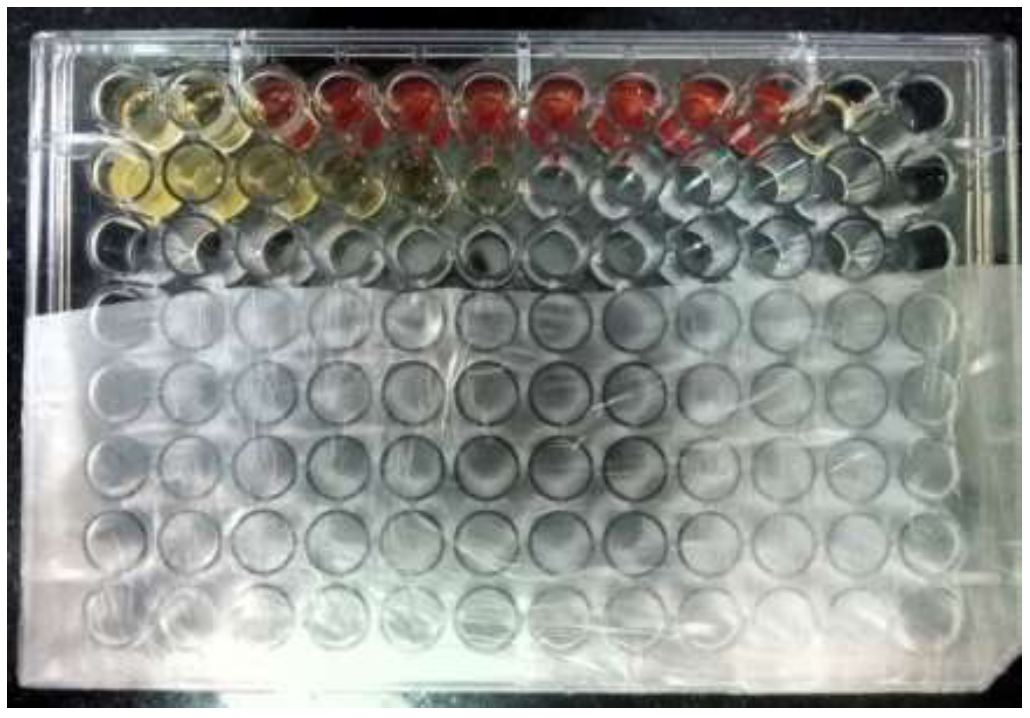
MIC assay of turmeric oil against Candida albicans by broth microdilution in a 96-well plate. Colour change indicates inhibition across serial dilutions.
3.3. Tensile Strength
The effect of incorporating turmeric oil on the mechanical properties was assessed by measuring tensile strength. On Day 1, the group treated with 20% turmeric oil showed a tensile strength of 0.086 ± 0.013 MPa, which was higher than that of the negative control (0.061 ± 0.036 MPa). The nystatin group demonstrated the highest tensile strength of 0.175 ± 0.043 MPa. Kruskal–Wallis analysis showed no significant differences between the turmeric oil groups and the negative control (p > 0.05), whereas the nystatin group showed significantly greater strength (p < 0.001) (Table 2). Over two weeks, all groups showed increased tensile strength (p = 0.001). Across all observation points, the turmeric oil-modified groups showed higher tensile strength values (Table 3). In the nystatin group, a significant increase was observed between days 7 and 14 (p =0.006). Changes in the negative control groups were limited.
| Tensile Strength | Tissue Conditioner |
Tissue Conditioner + Turmeric Oil |
Tissue Conditioner + Nystatin |
Kruskal-Wallis Test Statistic | P | |
|---|---|---|---|---|---|---|
| Day 1 | Mean | 0.061±0.036a | 0.086±0.013b | 0.175±0.043a,b | 17.85 | <0.001 |
| Median | 0.05 | 0.085 | 0.16 | |||
| Day 7 | Mean | 0.06±0.017a | 0.168±0.032a, b | 0.076±0.021b | 16.42 | <0.001 |
| Median | 0.06 | 0.18 | 0.08 | |||
| Day 14 | Mean | 0.071±0.008a | 0.191±0.038a | 0.156±0.046 | 13.58 | 0.001 |
| Median | 0.07 | 0.185 | 0.165 | |||
4. DISCUSSION
4.1. Rejection of Null Hypothesis and Key Findings
The present results did not support the null hypothesis. Incorporating turmeric oil increased antifungal activity against C. albicans without a measurable loss of tensile strength. Comparable responses have been documented for plant-based oils incorporated into denture tissue conditioners [7, 8, 15].
Curcumin is the main bioactive ingredient in turmeric oil. It disrupts the fungal membrane, thereby impairing cellular function. Earlier work showed reduced adhesion following downregulation of HSP90 and Cdr1 [8, 9, 16, 18]. These mechanisms were not assessed in this study; however, the observed inhibition pattern was consistent with earlier findings [19].
The antifungal efficacy observed with turmeric oil was comparable to that of nystatin- and azole-based denture tissue conditioners. Mechanical changes have been reported when azole antifungals are used at higher concentrations; however, no such alterations were observed for turmeric oil within the same tested dose range [2, 3]. To improve stability and prolong antifungal activity, nanoscale delivery systems—such as chitosan-based encapsulation—have been suggested as potential formulation strategies [20]. In this study, effective fungal inhibition was achieved only at concentrations above the minimum inhibitory concentration (MIC) of 12.5 µg/mL. Meaningful antifungal activity was observed only at a loading level of 20% w/w, while lower concentrations produced limited inhibition. Further increasing the concentration may compromise mechanical properties and increase the risk of adverse mucosal reactions, including contact dermatitis or urticaria [21].
In the disc diffusion assay, no inhibition zone was observed for the unmodified tissue conditioner. In contrast, a distinct inhibition zone was seen only in the sample containing 20% turmeric oil, with a diameter comparable to that of the positive control. Antifungal effectiveness declined over the 14 days, with the greatest reduction occurring after day 7. This trend is consistent with the gradual release and depletion of oil from the polymer matrix [21-24]. Controlled-release delivery systems have been proposed to minimise this loss of activity over time.
Curcumin has also demonstrated antifungal activity against nystatin-resistant Candida strains, with reported MIC values ranging from 7.8 to 32.25 µg/mL. These findings suggest potential resistance patterns among clinical isolates that remain susceptible to curcumin-based interventions [25].
4.2. Tensile Strength and Clinical Significance
Mechanical integrity is critical to the short-term clinical performance of denture tissue conditioners. The addition of 20% turmeric oil resulted in a lower tensile strength (0.086 ± 0.013 MPa) than that of the positive control (0.175 ± 0.043 MPa). However, a gradual recovery in strength was observed over the 14 days, and statistical analysis confirmed a substantial time-dependent increase (p = 0.001). These temporary changes are likely due to physicochemical interactions between turmeric oil components and the polymer matrix rather than permanent material degradation. Similar short-term mechanical variations have been reported in tissue conditioners modified with tea tree oil and conventional antifungal agents. Despite the initial reduction, the tensile strength values associated with 20% turmeric oil remained within an acceptable range for short-term clinical use. Previous studies also indicate that incorporating essential oils can preserve the functional properties of tissue conditioners, with plant-derived oils generally producing minimal mechanical alterations [14, 26-29]. As antifungal activity declines with time, denture tissue conditioners infused with turmeric oil require periodic replacement [30]. Nanomaterial-based strategies have been explored to enhance the durability of tissue conditioners. Silver nanoparticles exhibit antimicrobial activity, but their use at higher concentrations has been associated with reduced material hardness [31]. Similarly, silicon dioxide fillers raise concerns; an increased surface roughness may promote microbial adhesion. In contrast, studies involving chitosan or metal-oxide nanocomposites have reported controlled drug release and limited biofilm formation, supporting their potential for modifying tissue conditioners [32, 33]. Plant-derived formulations containing antifungal agents, however, have generally maintained material flexibility without compromising mechanical properties.
Encapsulation can enhance oil dispersion and control release, thereby extending turmeric oil retention in denture tissue conditioners. However, mucosal tolerance limits formulation, as concentrations above 20% (w/w) may irritate. Combining turmeric oil with a small dose of a synthetic antifungal may provide an effective and biocompatible alternative. This study was limited to a 14-day in vitro period and did not account for oral factors, such as saliva and functional loading, which may affect long-term clinical relevance [34, 35]. Only C. albicans ATCC® 10231 was tested, so the responses of other species and mixed biofilms remain unknown. The study did not assess turmeric oil release; chromatography could reveal release patterns and their impact on antifungal effectiveness.
More extended observation periods and in vivo testing are needed to assess clinical relevance. Randomised controlled trials could compare turmeric oil-infused tissue conditioners with other synthetic antifungal formulations; key outcomes include patient comfort and retention. Mucosal health and Candida colonisation should also be assessed over two to four weeks.
CONCLUSION
In this study, denture tissue conditioners containing 20% turmeric oil inhibited C. albicans while preserving mechanical strength. Short-term use is feasible and requires replacement after 1-2weeks. Turmeric oil showed good biocompatibility. Clinical studies are needed to verify its safety before routine use.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.M., M.G. and A.M.: Contributed to the conceptualisation, methodology, and data analysis; S.P. and A.Mo.: Assisted with data collection, resources, and manuscript drafting; M.G.: Supervised the project and critically revised the manuscript; S.R.: Performed the microbiological analysis and contributed to data interpretation. All authors have reviewed and approved the final manuscript.
LIST OF ABBREVIATIONS
| MIC | = Minimum Inhibitory Concentration |
| MIZ | = Mean Inhibitory Zone |
| MPa | = Megapascal (unit of tensile strength) |
| CFU | = Colony Forming Units |
| DMSO | = Dimethyl Sulfoxide |
| SDB | = Sabouraud Dextrose Broth |
| TTC | = 2,3,5-Triphenyl Tetrazolium Chloride |
| CLSI | = Clinical and Laboratory Standards Institute |
| HPLC | = High-Performance Liquid Chromatography |
| SEM | = Scanning Electron Microscopy (mentioned in discussion as future work) |
| SPSS | = Statistical Package for the Social Sciences |
| ASTM | = American Society for Testing and Materials |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This in vitro experimental study was conducted after obtaining ethical approval from the Institute of Dental Sciences, Siksha ‘O’ Anusandhan (Deemed to be University), Odisha, India (IDS/IEC/2024/PR-134).
AVAILABILITY OF DATA AND MATERIALS
All data and supporting material are available within the article.
ACKNOWLEDGEMENTS
The authors acknowledge the Department of Prosthodontics and the Centre for Biotechnology, Siksha ‘O’ Anusandhan, for their support during this research.

