All published articles of this journal are available on ScienceDirect.

Assessment of Maxillofacial Prosthesis Knowledge and Practice Among Dental Professionals in Saudi Arabia
Authors Info & Affiliations
Abstract
Aim
This 18-item online closed questionnaire-based study aimed to evaluate and assess the level of knowledge and practices of maxillofacial prosthesis (MFP) among different dental professionals in Saudi Arabia (SA).
Methods
An Electronic investigation was directed to dental professionals (final-year students, interns, general practitioners, MFP residents, and specialists). Participants were invited to respond to the online forms based on their knowledge and MFP practice. The collected answers were evaluated employing descriptive statistics as values and percentages. The association among participants, knowledge, and practice was analyzed using Chi-square, with a P-value of ≤0.05 indicating statistical significance.
Results
336 participants were included, with only 20 patients receiving MFP, those were 12, 3, and 5 patients who received MFP for the mandible, maxilla, and nasal MFPs, respectively. A significant difference was found between dental professional participants and MFP knowledge questions with p < 0.001, except for questions like ‘’Do you know that there is more than one type of maxillofacial prosthesis?”, ‘’How many maxillofacial specialists or consultants are in the place that you work?” and ‘’Is there interest to support and develop MFP from the Ministry of Health in the city?” with p-values of 0.104, 0.081, and 0.134, respectively. Also, a significant difference was detected between participants and their answers to most of the practice questions, with p < 0.001, except for the question related to the type of MFP they practice (p = 0.0125).
Conclusions
Dental practitioners have good knowledge, but the practice of MFP is still fair. Referrals and multidisciplinary approaches for managing these patients remain poor.
1. BACKGROUND
Maxillofacial prosthesis (MFP) is a branch of prosthodontics concerned with the reconstruction and/or support of oral, maxillofacial, craniofacial, and/or oral structures through prostheses that may or may not be removable [1]. It is the subspecialty of prosthodontics that deals with the creation of appliances for structures beyond the immediate dental and alveolar region [2-4].
Maxillofacial burdens are facemask deformities consequential after congenital deformities, surgical removal of tumors, osteoradionecrosis, and infections; the resulting disfigurement may have lifelong consequences due to difficulty in recovery, causing physical disability and mental disorders [5, 6]. Patients who have previously been involved in an accident or have undergone surgical excision of unhealthy tissue need to restore function and aesthetics, so reconstruction procedures in these cases would be performed to minimize psychological disturbance [5-7].
Gupta et al., 2017 and Vladimir, 2022 stated that types of MFP are either intraoral prosthesis, extraoral prosthesis, or their combination [8, 9]. An example of an extraoral prosthesis is an ocular prosthesis after the loss of an eye, which leads to physical challenges in an individual’s life. In such cases, careful preoperative, surgical, and prosthetic scheduling engaging a multidisciplinary approach is critical for effective rehabilitation [10]. Objectives of prosthetic treatment include aesthetics, comfort, function, and patient satisfaction, which could result in confidence and improved quality of life for patients [11-13].
The maxillofacial prosthodontist is an essential member of the multidisciplinary team that works together to treat the patient. He monitors the patient closely for hospital protocols and medical health. He assists the surgeon by manufacturing facial moulages and operating stents to help recovery and improve prosthesis retention, support, and stability [12-14].
Dentistry in the current century mostly comprises aesthetics because of the increased awareness of patients concerning their physical appearance [15, 16]. After surgery, patients are not referred to prosthodontists for recreation of the lost part, possibly due to a lack of awareness about a particular field, namely, the rehabilitation of maxillofacial defects. Hence, appropriate knowledge of the reasons and probable action modalities of maxillofacial defects is essential among different dental professionals because they are a part of the future of dentistry [5].
Dahane et al., assessed the information about the awareness and knowledge of practitioners in and around Wardha City towards the MFP. They reported that the commonest source of information was a dentist acquaintance (39.7%), followed by a friend (38.8%) and books (31.5%) [17]. Singh et al., surveyed the institutional and private medical practitioners; they stated that maxillofacial prosthodontics, as a subdivision of dental medicine, deals with the rehabilitation of lost facial structures, and up to 75.4% awareness was detected among the medical fraternity; most of the participants became aware of it from their dentists, friends, or any other media [18]. Elastomeric impression materials (Silicones) are the most commonly used material for the fabrication of MFP, and other materials are acrylic resins or copolymers [5, 17, 19, 20].
Other surveys assessed the knowledge and practice of MFP worldwide. Dahane et al. reported poor knowledge about maxillofacial prosthodontics as a subject in India [17]. In the USA, MFPs and appliances are not commonly seen in the general dental population, so primary care dentists and physicians are often unaware of the variety and possibilities of these prostheses, and many patients go years without adequate treatment [9]. Also, fair knowledge and awareness about MFP among medical and dental physicians has improved knowledge about prosthetic rehabilitation [20].
The undergraduate program for dentistry is a 6-year program, and followed by a one-year dental internship program. MFP is presented as a few lectures in the teaching courses at all colleges of SA. Although, to our knowledge and during our literature search, MFP has not been studied among dentists yet, and insufficient information is available about MFP in SA. Hence, this study was conducted to evaluate knowledge and practices concerning maxillofacial diseases and defects and their prosthetic rehabilitation among different dental professionals in SA. The null hypothesis is that no significant differences between participants in the knowledge and practice of MFPs.
2. PARTICIPANTS AND METHODS
2.1. Study Design and Ethical Consideration
A cross-sectional, web-based online form study was conducted for different dental professionals as 6th-year dental students, dental interns, general practitioners, and maxillofacial residents and specialists, through an e-survey using Google Forms between November 2023 and April 2024. This study was conducted in accordance with the ethics of the Helsinki Declaration [21]. The study was approved by the Institutional Ethical Review Board Committee of the College of Applied Medical Sciences, King Khalid University, Saudi Arabia (ECM#2024-3102). All participants had signed a consent form before enrollment in the study, and it was included in the Google form.
2.2. Study Setting and Inclusion Criteria
Copies of questionnaires were sent through WhatsApp to different groups in different cities of dental professionals in Saudi Arabia. The study population was stratified to include 6th-year dental students (final-year undergraduates), dental interns (recent graduates completing the mandatory one-year internship), general practitioners (licensed dentists with up to three years of experience and not in a specialty program), maxillofacial residents (those in postgraduate training for oral surgery or prosthodontics with maxillofacial exposure), and maxillofacial specialists (clinicians with completed specialist training).
2.3. Population Size Calculation
Using G*Power software (version 3.1.9.4, University of Dusseldorf). The effect size (d), α, and1-β (power) were 0.2, 0.05, and 0.80, respectively. A survey sample of 316 participants was essential to realize statistically valid outcomes, and this figure was increased to 336 to make up for nonresponse through WhatsApp [22, 23].
2.4. Instrument Development, Validity, and Reliability
A panel of two maxillofacial prosthodontics and two consultants of maxillofacial surgeons evaluated the content validity of the questionnaire. Importance, significance, clarity, and simplicity for each question were evaluated from a scale of 1 to 4, with 4 being the highest and 1 being the lowest [24]. The content validity index was 0.85, representing that the questionnaires were valid. Reliability was measured and determined by testing internal consistency, and the Cronbach’s alpha was 0.839.
2.5. Study Tools and Data Collection
In addition to participant characteristics, an 18-item closed questionnaire that includes the information and understanding in relation to MFP was adopted from previous global studies [5, 9, 17, 18, 20] with some changes. The survey form was translated into Arabic through the support of a native Arabic speaker; the queries were then forward and backward translated into English [22, 23].
2.6. Questionnaire Parts
The questionnaire’s validity was adjudicated by a board of ten-member experts committed. Reliability was recognized by conducting a test-retest amongst 15 volunteers from different dental clinics. The kappa value was 0.85, which indicated high consistency. The test-retest was trailed by a pilot exploring amongst 15 volunteers who were asked to respond to the survey and offer comments on its clarity, content, and brevity. The time between the test and retest pilot study was 3 weeks. Spaces as boxes for answers were designed, and dentists from selected professional levels and cities ticked on a single choice for each query. A contributor can only reply to the survey once, and inquiries need to be responded. The responses were directly recognized and composed through Google Forms. Informed consent was also in the Google Form, along with the questionnaire copies through WhatsApp.
An English questionnaire type was sent by WhatsApp web-based and divided into three portions was distributed by different type of social media. The form consists of a brief explanation of the purpose of the study, the method of data collection, and close-ended questions. The questionnaire has two other parts in addition to age, gender, and professional level.
The first part of the survey includes questions regarding gender, age, and professional level (6th or Final Year Dental Student, Dental Intern, General Practitioner, and Maxillofacial Resident and Specialist). The second part consists of 12 questions with general knowledge of MFP as ‘’MFP can be made by Prosthodontist, General Practitioner, Oral Surgeon, Any specialist, Others”, ‘’The most common cause for the need for MFP can be patients with functional and/or aesthetic problem”, ‘’The material(s) used for construction of MFP is (are) Acrylic, Elastomeric Impression Materials, Wax, All of them”, ‘’Which of the following prosthesis type of MFP are you aware as maxilla, mandible, ear, eye, and nasal with midfacial prosthesis”. The third part of the questionnaire consists of six questions concerning the practice of MFP and the answers can be yes or no. Those are ‘’Did you face a patient who needs MFP?”, ‘’Do you work with MFP?”, ‘’At the undergraduate level have you received training on MFP?”, and ‘’During your undergraduate studies, have you fabricated an MFP?”. The participants knowledge and practice scores were calculated on the percentage achieved for the proper and accurate answers divided by the total number of questions. A copy of questionair is presented at the end of the maunscript.
2.7. Statical Analysis
Data were analyzed using the statistical package for the Social Sciences (SPSS) program (version 26) and Microsoft Excel. The acquired data were analyzed using descriptive statistics, which included numerical values and percentages. The association among dental professionals, knowledge, and practice was analyzed using Chi-square. P < 0.05 indicated statistical significance.
3. RESULTS
3.1. Characteristics of the Participants
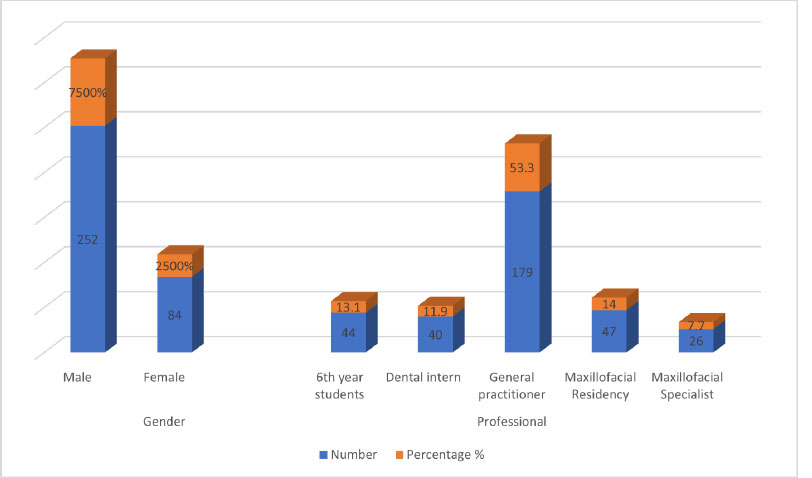
A total number of 38 questionnaires were not included in the results due to incomplete answers and lack of some information’s. The number of participants who filled out and returned the questionnaire was 336 of which 252 (75%) were males. The participants were aged between 20 and 53 years old, with a mean age and standard deviation of 32.31± 7.3675 years. According to profession, the participants were 44 (13.1%) 6th-year dental students, 40 (11.9%) dental interns, 179 (53.3%) general practitioners, and 47 (14%) maxillofacial residents and 26 (7.7%) specialists (Fig. 1).
3.2. Dental Professional Participants based on their Maxillofacial Prosthesis Knowledge
Table 1 presents the feedback of different professionals in relation to knowledge of MFP. A 272 (81%) of the participants heard about MFPs, and 225 (67.0%) know that there is more than one type of maxillofacial prosthesis. About 188 (56.0%) of the respondents stated that MFP was used to restore function and aesthetics, but those who said that they recognized MFP from college were 160 (47.6%). Prosthodontists are responsible for the construction of MFP, accounting for 204 (60.7%). However, 189 (56.3%) stated that a combination of congenital abnormalities, surgical resection of tumors, and trauma was the cause for the need for MFP. Concerning the material used for MFP, elastomeric impression material was recorded 104 (31.0%), which is higher than other choices as acrylic and waxes. MFP was used to replace part of the maxilla and/or mandibula and/or both, ear, eye, and nasal cavity, and counted as 78 (23.2%), 57 (17.0%), 12 (3.6%), 189 (56.3%), respectively.
Distribution of the participants by gender and professional level.
| Question | Answer Choices | (n) | % |
|---|---|---|---|
| Have you heard about maxillofacial prostheses? | Yes | 272 | 81.0 |
| No | 64 | 19.0 | |
| Maxillofacial prosthesis is used for ….… | Patients with functional problem | 32 | 9.5 |
| Patients with aesthetic problem | 88 | 26.2 | |
| Both | 188 | 56.0 | |
| I Don’t Know | 28 | 8.3 | |
| From where do you know about this type of prosthesis? | College | 160 | 47.6 |
| Media | 84 | 25.0 | |
| Friends | 56 | 16.7 | |
| Books | 12 | 3.6 | |
| Workplace | 24 | 7.1 | |
| Do you know that there is more than one type of maxillofacial prosthesis? | Yes | 225 | 67.0 |
| No | 111 | 33.0 | |
| MFP can be made by …… | Prosthodontist | 204 | 60.7 |
| General Practitioner | 24 | 7.1 | |
| Oral Surgeon | 72 | 21.4 | |
| Any specialist | 32 | 9.5 | |
| Others | 4 | 1.2 | |
| The primary cause for the need of MFP can be …. | Congenital abnormalities | 78 | 23.2 |
| Surgical resection of tumors | 57 | 17.0 | |
| Trauma | 12 | 3.6 | |
| Combination of those | 189 | 56.3 | |
| The material(s) used for the construction of MFP is (are) …. | Alginate | 48 | 14.3 |
| Acrylic | 56 | 16.7 | |
| Elastomeric Impression Materials | 104 | 31.0 | |
| Wax | 16 | 4.8 | |
| All of them | 160 | 47.6 | |
| Which of the following types of MFP are you aware of? | Prosthesis for maxilla and mandible | 78 | 23.2 |
| Ear | 57 | 17.0 | |
| Eye | 12 | 3.6 | |
| Nasal and midfacial prosthesis | 189 | 56.3 | |
| How many maxillofacial specialists or consultants are in the place where you work? | 1 | 260 | 77.4 |
| 2 | 64 | 19.0 | |
| More than 2 | 12 | 3.6 | |
| Is there is interest in supporting and developing MFP from the Ministry of Health in the city? | YES | 264 | 78.6 |
| NO | 72 | 21.4 | |
| Are the materials used in the MFP are available and according to good standards? | YES | 260 | 77.4 |
| NO | 76 | 22.6 | |
| The main cause of MFP failure is? | Unacceptable quality of material used. | 28 | 8.3 |
| Incorrect Impression Material | 52 | 15.5 | |
| Unacceptable aesthetic result | 52 | 15.5 | |
| All of above. | 204 | 60.7 |
The number of maxillofacial specialists in the place where they work was 260 (77.4%), 64 (19.0%), and 12 (3.6%) of 1, 2, and 3 specialists, respectively. Both questions, “Are the materials used in the MFP available and according to good standards?” and “Is there interest to support and develop MFP from the ministry of health in the city?” recorded almost equal percentages for yes (more than 77%, Table 1).
To objectively interpret the knowledge level of the participants, a benchmark of correct answers was established based on current literature and standard prosthodontic textbooks [1-4, 8, 9, 17, 19]. The correct answers for the knowledge-based questions are presented in Supplementary Table S1.
3.3. Dental Professional Participants based on their Maxillofacial Prosthesis Practice
With regard to the practice of MFP among participants, 161 (47.9%) respondents stated that they faced patients who needed MFP. Among the respondents, only 20 reported having personally provided an MFP for a patient. Of these 12 (60.0%), 3 (15.0%), 5 (25.0%), those provide MFP for mandible, maxilla, and nasal cavity MFPs, respectively. A 240 (71.4%), did not work with a MFP team, and 224 (66.7%), of participants have received training on MFP, and 252 (75.0%) of have fabricated a MFPs during undergraduate studies, while 260 (77.4%) of participants have not handled patients' needs for MFP at their dental office Table 2.
3.4. Association between Dental Professional Participants and Maxillofacial Prosthesis Knowledge
Table 3 shows the association of MFP knowledge with dental professionals, with the highest number and percentages recorded among general practitioners and dental interns. The total number [27 (8%)] of maxillofacial residents stated that they heard about MFP. Most dental professionals stated that MFP was used to restore functional and aesthetic problems, with the highest number and percentage (98, 29.2%) recorded for general practitioners. A combination of congenital abnormalities, surgical tumor resection, and trauma caused MFP construction. Most respondents stated that all materials can be used in MFP impression, but the highest was recorded for elastomers, especially among all maxillofacial residents. Most types of MFP were fabricated for patients, even in small numbers. All the above questions recorded significant differences among dental professionals participants and MFP knowledge questions using the Chi-square test (p < 0.001).
The answers to the questions “Do you know that there is more than one type of maxillofacial prosthesis?” “How many maxillofacial specialists or consultants are in the place where you work?” and “Is there interest in supporting and developing MFP from the Ministry of Health in the city?” were not significantly different among dental professionals (p = 0.104, p = 0.081, and p = 0.134, respectively; Table 3).
3.5. Association between Dental Professional Participants and Maxillofacial Prosthesis Practice
In relation to the practice of MFP, the Chi-square test displayed significant differences in the answers of dental professionals to the question “Did you face a patient who needed MFP?” “Do you work with a maxillofacial prostheses team?” “At the undergraduate level, have you received training on MFP?” “During your undergraduate studies, have you fabricated a maxillofacial prosthesis?” and “At your dental clinic, have you fabricated a maxillofacial prosthesis?” (p < 0.001 for all questions). No significant difference was recorded in the question “What type of MFP do you practice?” (p = 0.125, Table 4).
| Question | Answer Choices | (n) | % |
|---|---|---|---|
| Did you face a patient who needs MFP? | Yes | 161 | 47.9 |
| No | 175 | 52.1 | |
| Do you work with the maxillofacial prostheses team? | Yes | 96 | 28.6 |
| No | 240 | 71.4 | |
| If yes. What type of MFP do you practice? | Prosthesis for mandible | 12 | 60.0 |
| Prosthesis for maxilla | 3 | 15.0 | |
| Nasal prosthesis | 5 | 25.0 | |
| At the undergraduate level have you received training on MFP? | Yes | 112 | 33.3 |
| No | 224 | 66.7 | |
| During your undergraduate studies, have you fabricated Maxillofacial Prostheses? | Yes | 84 | 25.0 |
| No | 252 | 75.0 | |
| At your dental clinic, have you fabricated a maxillofacial prosthesis? | Yes | 76 | 22.6 |
| No | 260 | 77.4 |
| Question | Subcategory |
6th Year Student N (%) |
Dental Intern N (%) |
General Practitioner N (%) |
Maxillofacial Residency N (%) |
Maxillofacial Specialist N (%) |
P-value |
|---|---|---|---|---|---|---|---|
| Have you heard about maxillofacial prostheses? | Yes | 44(13.1) | 28(8.3) | 151(44.9) | 27(8.0) | 22(6.5) | < 0.001 |
| No | 0(0.0) | 12(3.6) | 28(8.3) | 20(6.0) | 4(1.2) | ||
| Maxillofacial prostheses are used for ……… | Patients with functional problem | 16(4.8%) | 0(0.0%) | 16(4.8%) | 0(0.0%) | 0(0.0%) | < 0.001 |
| Patients with aesthetic problem | 8(2.4%) | 8(2.4%) | 49(14.6%) | 18(5.4%) | 5(1.5%) | ||
| Both | 16(4.8%) | 32(9.5%) | 98(29.2%) | 25(7.4%) | 17(5.1%) | ||
| I Don’t Know | 4(1.2%) | 0(0.0%) | 16(4.8%) | 4(1.2%) | 4(1.2%) | ||
| From where do you know about this type of prosthesis? | College | 24(7.1) | 16(4.8) | 100(29.8) | 8(2.4) | 12(3.6) | < 0.001 |
| Media | 16(4.8) | 12(3.6) | 46(13.7) | 5(1.5) | 5(1.5) | ||
| Friends | 4(1.2) | 12(3.6) | 20(6.0) | 16(4.8) | 4(1.2) | ||
| Books | 0(0.0) | 0(0.0) | 0(0.0) | 12(3.6) | 0(0.0) | ||
| Workplace | 0(0.0) | 0(0.0) | 13(3.9) | 6(1.8) | 5(1.5) | ||
| Do you know that there is more than one type of maxillofacial prosthesis? | Yes | 28(8.3) | 32(9.5) | 124(36.9) | 27(8.0) | 14(4.2) | 0.104 |
| No | 16(4.8) | 8(2.4) | 55(16.4) | 20(6.0) | 12(3.6) | ||
| MFP can be made by …… | Prosthodontist | 24(7.1) | 16(4.8) | 119(35.4) | 31(9.2) | 14(4.2) | < 0.001 |
| General Practitioner | 4(1.2) | 4(1.2) | 8(2.4) | 4(1.2) | 4(1.2) | ||
| Oral Surgeon | 8(2.4) | 12(3.6) | 40(11.9) | 4(1.2) | 8(2.4) | ||
| Any specialist | 8(2.4) | 4(1.2) | 12(3.6) | 8(2.4) | 0(0.0) | ||
| Others | 0(0.0) | 4(1.2) | 0(0.0) | 0(0.0) | 0(0.0) | ||
| The most common cause for the need for MFP can be …. | Congenital abnormalities | 20(6%) | 12(3.6%) | 32(9.5%) | 5(1.5%) | 9)2.7%) | < 0.001 |
| Surgical resection of tumors | 8(2.4%) | 8(2.4%) | 17(5.1%) | 20(6%) | 4(1.2%) | ||
| Trauma | 0(0.0%) | 4(1.2%) | 4(1.2%) | 0(0.0%) | 4(1.2%) | ||
| Combination of those | 16(4.8%) | 16(4.8%) | 126(37.5%) | 22(6.5%) | 9(2.7%) | ||
| The material(s) used for the construction of MFP is (are) …. | Alginate | 4(1.2) | 12(3.6) | 28(8.3) | 4(1.2) | 0(0.0) | < 0.001 |
| Acrylic | 24(7.1%) | 4(1.2%) | 21(6.3%) | 7(2.1%) | 0(0.0%) | ||
| Elastomeric Impression Materials | 12(3.6%) | 16(4.8%) | 44(13.1%) | 24(7.1%) | 8(2.4%) | ||
| Wax | 0(0.0%) | 8(2.4%) | 4(1.2%) | 0(0.0%) | 4(1.2%) | ||
| All of them | 8(2.4%) | 12(3.6%) | 110(32.7%) | 16(4.8%) | 14(4.2%) | ||
| Which of the following types of MFP are you aware of? | Prosthesis for maxilla & mandible | 20(6%) | 12(3.6%) | 32(9.5%) | 5(1.5%) | 9)2.7%) | < 0.001 |
| Ear | 8(2.4%) | 8(2.4%) | 17(5.1%) | 20(6%) | 4(1.2%) | ||
| Eye | 0(0.0%) | 4(1.2%) | 4(1.2%) | 0(0.0%) | 4(1.2%) | ||
| Nasal and midfacial prosthesis | 16(4.8%) | 16(4.8%) | 126(37.5%) | 22(6.5%) | 9(2.7%) | ||
| How many maxillofacial specialists or consultants are in the place that you work? | 1 | 32(9.5%) | 28(8.3%) | 135(40.2%) | 43(12.8%) | 22(6.5%) | 0.081 |
| 2 | 12(3.6%) | 12(3.6%) | 44(13.1%) | 4)1.2%) | 4(1.2%) | ||
| More than 2 | 0(0.0%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | ||
| Is there is interest in supporting and developing MFP from the ministry of health in the city? | Yes | 32(9.5) | 32(9.5) | 139(41.4) | 43(12.8) | 18(5.4) | 0.134 |
| No | 12(3.6) | 8(2.4) | 40(11.9) | 4(1.2) | 8(2.4) | ||
| Are the materials used in the MFP available and according to good standards? | Yes | 28(8.3) | 24(7.1) | 142(42.3) | 40(11.9) | 26(7.7) | < 0.001 |
| No | 16(4.8) | 16(4.8) | 37(11.0) | 7(2.1) | 0(0.0) | ||
| The main cause of MFP failure is? | Unacceptable quality of material used. | 8(2.4) | 8(2.4) | 8(2.4) | 0(0.0) | 4(1.2) | < 0.001 |
| Incorrect Impression Material | 0(0.0) | 4(1.2) | 29(8.6) | 14(4.2) | 5(1.5) | ||
| Unacceptable aesthetic result | 16(4.8) | 4(1.2) | 12(3.6) | 12(3.6) | 8(2.4) | ||
| All of above. | 20(6.0) | 24(7.1) | 130(38.7) | 21(6.3) | 9(2.7) |
| Question | Subcategory |
6th Year Student N(%) |
Dental Intern N(%) |
General Practitioner N(%) |
Maxillofacial Residency N(%) |
Specialist N (%) |
P-value |
|---|---|---|---|---|---|---|---|
| Did you face a patient needs MFP? | Yes | 24(7.1) | 22(6.5) | 65(19.3) | 37(11.0) | 13(3.9) | < 0.001 |
| No | 20(6.0) | 18(5.4) | 114(33.9) | 10(3.0) | 13(13.9) | ||
| Do you work with maxillofacial prostheses team? | Yes | 20(6.0) | 20(6.0) | 20(6.0) | 20(6.0) | 16(4.8) | < 0.001 |
| No | 24(7.1) | 20(6.0) | 159(47.3) | 27(8.0) | 10(3.0) | ||
| If yes. What type of MFP do you practice? | 0.00 | 0.00 | 46 (47.9) | 38 (39.6) | 12 (12.5) | 0.125 | |
| At the undergraduate level have you received training on MFP? | Yes | 20(6.0) | 20(6.0) | 32(9.5) | 28(8.3) | 12(3.6) | < 0.001 |
| No | 24(7.1) | 20(6.0) | 147(43.8) | 19(5.7) | 14(4.2) | ||
| During your undergraduate studies have you fabricated a maxillofacial prosthesis? | Yes | 16(4.8) | 8(2.4) | 32(9.5) | 16(4.8) | 12(3.6) | 0.002 |
| No | 28(8.3) | 32(9.5) | 147(43.8) | 31(9.2) | 14(4.2) | ||
| At your dental clinic, have you fabricated a maxillofacial prosthesis? | Yes | 16(4.8) | 8(2.4) | 20(6.0) | 28(8.3) | 6 (1.2) | < 0.001 |
| No | 28(8.3) | 32(9.5) | 159(47.3) | 19(5.7) | 20(6.0) |
4. DISCUSSION
This study was carried out to assess and evaluate knowledge and practices concerning MF defects and their prosthetic therapy among different dental professionals in Saudi Arabia. According to the findings, dentists have favorable or high as mentioned in Table 1 knowledge about MFP at all levels (6th-year students, dental interns, general practitioners, maxillofacial residents, and maxillofacial specialists), while the knowledge level of general practitioners (44%) was slightly higher. This could be attributed to the fact that they received classes and course of MFP in their undergraduate program. The overall results revealed that they have slight knowledge, but most of them have never practiced MFP (71%), likely because many respondents were from non-specialized centers and had not encountered MFP cases. Additionally, MFP fabrication is typically conducted by certified Maxillofacial Prosthodontists, not general practitioners in Saudi Arabia. This result agrees with the study of Vladimir 2022, who found that MFPs and appliances are not commonly seen in general dental practitioners [9]. Also, Singh et al., 2023 found that knowledge and awareness about MFPs were fairly satisfactory [18], while Lee concluded that the capability of the general dental practitioners was barely acknowledged about MFP [25].
The maxillofacial area plays a central role in personal presence because it defines the individuality of the person. However, any minor modification can create a drastic variation in appearance and negatively affect the psychology of the patient [26]. Rehabilitation is considered a part of prosthodontics as MFP. However, the space of maxillofacial prosthodontics as a subject has not been recognized among multidisciplinary dental teams in dealing with maxillofacial defects; MFPs and appliances are not commonly seen in the general dental population, primary care dentists, and physicians who are often unaware of the variety and possibilities of these prostheses [27]. Many patients spent several years without adequate treatment. Advances in the prosthetic rebuilding of structural and functional defects can recover the outcomes if carefully planned, unbiased rehabilitation systems are created [17].
Most of the patients suffering from such defects were not referred to an MFP and remained untreated. The primary cause could be or may not be the deficiency of awareness among medical practitioners, such as surgeons, ophthalmologists, ENT specialists, and plastic physicians, to treat such patients for remaining defects after surgery [18]. The advantage of MFP is that it can be fabricated for any area of the face and the jaws or the cranium, regardless of the extent of the defect; the prosthesis also allows for regular inspection and monitoring of the defect site, thereby aiding in early identification of any recurrence [8, 9, 28-30].
The need to provide future dentists with basic knowledge about maxillofacial defects has increased, and these types of abnormality can be broadly classified as congenital and acquired defects; dentists should determine the source and propose an effective treatment style for the persistent [31]. In the present survey, a high level of knowledge about MFP was recorded (81%). Shreya and Ramish [5] also found that knowledge regarding MF defects among clinical and preclinical phase students was acceptable. Singh et al. 2023 reported that 75.4% of the participants were aware of MFPs as a division of dental specialty [18].
This study stated that a maximum of the participants had the thought that maxillofacial defects have multiple etiologies and necessitate a multidisciplinary system. Rehabilitation indicates to the restoration of former pleasure, which is the spirit of the deal provided by an MFP who is trained to make a prosthesis to restore aesthetic, functional, and psychological spaces related to the defect [17]. The present work showed that 56.3% of the participants said that MFP restored function and aesthetics.
The common foundation of data was a dentist colleague, then friends and books [17, 18]; this finding contradicted the previous report that the most common source of information was college (47.6%) followed by media (25%), friends (16.7%), and books (3.6%) [32]. More than half of the respondents in the current study were newly graduated general practitioners (53.3%). A maximum of the applicants was alert to the role of prosthodontists in the therapy of MFP defects, and the awareness concerning the measures reached 60.7% [33] as similar percentage in the current study. This finding agrees with most of the published papers [18, 20, 25, 34].
Regarding the material used for the construction of MFP, 47.6% of the participants used acrylic, elastomeric impression materials, and wax. In contrast to the findings of Dahane et al.,2021 [17], the participants said that the materials used for the fabrication of MFP were acrylic resin and silicone (26.9%). Kakkad et al., 2021 [20] showed that 74.3% of the participants used acrylic resins, acrylic copolymers, and silicone elastomers for the fabrication of facial prostheses. About 68.9% of the respondents in the study of Shreya and Ramish stated that the most used material for MFP fabricating was silicone [5]. Silicon is preferred by general practitioners of different levels for MFP fabrication [35]. About 47.6% of the survey participants specified that elastomers were the commonly used replica materials for maxillofacial defects. By contrast, Shreya and Ramish [5] reported that most participants stated that wax was the most commonly used impression material (57.7%). Singh et al., 2023 stated that 85% of the participants felt that congenital and acquired defects required rehabilitation, consistent with the present data, where 56.3% of the participants felt the same [18].
Early referral of patients to MFPs may add preoperative and postoperative benefits, such as better outcomes of the prosthesis as well as improved quality of life of a patient requiring management of head and neck rehabilitation [14]. Nasal and midfacial prosthesis was the most familiar (56.3%), followed by maxillary and mandibular prosthesis (23.2% and 17%, respectively) and eye (3.6%) prosthesis [36]. Singh et al. 2023 reported 14.7% of participants for the same type of MFP who were aware that the prosthesis was dealt with by prosthodontists, including nasal and midfacial prosthesis, cranial prosthesis, eye, ear, and maxillary, mandibular, or figure prosthesis [18].
The rehabilitation of both intraoral and extraoral defects is a challenging characteristic of MFP. It involves continuous practice to increase confidence and expertise [8]. About 47.9% of the participants answered that they faced patients with MFP, similar to the report (49.2%) of Singh et al., 2023 [18]. In the present study, 52.1% of practitioners did not encounter patients who needed MFP, and 47.9% said they worked with the MFP team for prosthesis of mandible (60%), nasal cavity (25%), and maxilla (15%). Dahane et al., 2021 also found that 73.5%of the practitioners did not face patients with MF defects, and 24% encountered such participants, belonging generally to the division of ophthalmology and ENT related to educational societies [17]. Shreya and Ramesh, 2020 stated that approximately 50% of the undergraduates had not seen a single case of MFP defects [5]. Our participants who did not receive training in MFP were 66.7%, and those who did not fabricate MFP at the undergraduate level were 75% and 77.4%.
Most related studies published in Saudi Arabia were case reports. Mathar et al. described a rehabilitation of the nasal defect of a patient with a nasal prosthesis by using the donor method; the main advantages of MFP include non-invasiveness, cost-effectiveness, conservativeness, tissue tolerance, esthetics, ease of fabrication, and cleanness [37]. Surgeons and prosthetic specialists work together for the full rehabilitation of MFPs of patients. The prosthodontist involved should be aware of the situation so that a better service is rendered to the patient [38]. Different types of silicon materials used as MFP after 6 months showed a slight color pigmentation, indicating better color stability of this type of prostheses [39]. Other studies recommended that MFP should be selected based on the acceptable color change of the materials after immersion in different beverage solutions [40].
Most dental practitioners with their different working places stressed the importance of using MFP to restore different lost structures, as well as head and face structures [41]. The overall number of participants in the current study was good for the knowledge part, but poor for the practical part, which is parallel with the findings of the recent publication by Ahmed et al, (2024), who stated that among Sudanese dental practitioners, recorded good knowledge and poor in practice towered MFP [34].
The current survey study focused on a vital field of dentistry and investigated the need and the weakness of such a specialty; this can be considered as a strength of this study. A recommendation for future research is to include all regions within SA and to select specific groups, such as prosthodontists and maxillofacial surgeons, for a more detailed analysis. Also, the study noted that referrals and a multidisciplinary approach to managing these patients are lacking, resulting in affected patients not finding the right dental practitioners for proper treatment and comprehensive rehabilitation. An attention is to recommend including the MFP practice integration in the dental curriculum or healthcare system.
5. STUDY LIMITATIONS
This study has some limitations. This study was designed in the form of a questionnaire to indirectly collect evidence. Extra actual procedures include particular contacts and/or meetings. The sample size is small, and the study has a limited geographic coverage and self-reported data to offer a sound understanding of the knowledge and practice of prosthetic therapy of maxillofacial faults between different dental professionals. A large number of participant was be comprised of the various societies and colleges in the state, particularly all the maxillofacial and prosthodontic centers.
CONCLUSION
Overall, this study concluded that dental professionals and practitioners possess a good level of knowledge and a fair level of practice regarding the maxillofacial prosthetics specialty. However, it highlighted the need to join hands to form a multidisciplinary team, which will result in the improvement of the health-related quality of life of individuals with maxillofacial deficiency.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: A.O., M.M.A.: Study conception and design; F.A.A; B.M.A; M.D.A; F.A.A; M.M.A.: Data collection; A.A.D., G.M.A. . K.Y.M.A.: Analysis and interpretation of results; A.O. . M.M.A.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MFP | = Maxillofacial prosthesis |
| SA | = Saudi Arabia |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Institutional Ethical Review Board Committee of the College of Applied Medical Sciences, King Khalid University, Saudi Arabia (ECM#2024-3102).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
All participants had signed a consent form before enrollment in the study, and it was included in the Google form.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

