All published articles of this journal are available on ScienceDirect.

Cell Biocompatibility, Antimicrobial, Antibiofilm, and Mechanical Properties of Dental Glass Ionomer Cement Containing Silver-loaded Silica Nanoparticles
Authors Info & Affiliations
Abstract
Introduction
Reducing the risk of bacterial colonization of dental materials can potentially decrease the need for systemic antibiotic therapies, thus minimizing the risks of antibiotic resistance and adverse drug reactions. Furthermore, the antimicrobial and anti-biofilm properties of these materials contribute to enhanced patient safety by lowering the likelihood of post-operative infections. The aim of this in vitro study was to investigate the effect of adding mesoporous silica nanoparticles containing silver on the safety, antimicrobial, and mechanical properties of glass ionomer cement.
Materials and Methods
Glass ionomer cement was mixed with mesoporous silica nanoparticles containing silver until completely blended. The MTT method was used to assess the safety of the material. The microbroth dilution method was used to investigate the antibacterial effect of the nanoparticles and determine the MIC and Minimum Bactericidal Concentration (MBC). The disk diffusion method was also used to evaluate the microbial activity of the nanoparticle-containing cements. For the solubility test, materials were prepared according to ISO 4049, and the dissolution test was performed. The Shapiro-Wilk test was used to assess the normality of the data. The t-test was used to compare the results between groups. GraphPad software was used to analyze the data. A probability value of less than 0.05 was considered significant.
Results
Significant differences were observed in the growth inhibition zones among the groups (p=0.001), with the cement containing 5% Nanoparticles Showing Superior Results Compared To Those With 3% (p=0.03) And 1% (p=0.01). Similarly, the Minimum Inhibitory Concentration (MIC) analysis revealed a notable difference between groups (p=0.0001), where the 5% nanoparticle cement outperformed the 3% (p=0.001) and 1% (p=0.02) formulations. For Minimum Bactericidal Concentration (MBC), the 5% nanoparticle group again demonstrated significantly better results (p=0.0001) compared to the 3% (p=0.001) and 1% (p=0.0001) groups. The Minimum Biofilm Inhibitory Concentration (MBIC) followed a similar trend (p=0.0001), with the 5% nanoparticle cement yielding better outcomes than the 3% (p=0.001) and 1% (p=0.0001) formulations. Solubility tests indicated no significant difference between cements with and without nanoparticles (p=0.4). However, water absorption measurements showed a significant increase in the nanoparticle-containing cement compared to the control (p=0.02). Lastly, flexural strength assessments found no statistically significant difference between nanoparticle-containing and nanoparticle-free cements (p=0.7).
Discussion
These findings highlight the potential of Ag-MSN-enriched GICs in clinical use, where antimicrobial effects are critical, such as in high-caries-risk patients or under crowns and bridges.
Conclusion
The findings of this study demonstrate that incorporating 5% nanoparticles into cement formulations significantly enhances their antimicrobial properties, as evidenced by improved growth inhibition zones, MIC, MBC, and MBIC values compared to lower nanoparticle concentrations (3% and 1%). While the inclusion of nanoparticles increases water absorption, it does not negatively affect the solubility or flexural strength of the cement. These results suggest that nanoparticle-enriched cement, particularly at a 5% concentration, holds potential for applications requiring enhanced antimicrobial activity without compromising structural integrity.
1. INTRODUCTION
It has been reported that the main cause of treatment failures in fixed prostheses is secondary caries. Therefore, cements can play an important role in caries prevention, and the presence of antibacterial properties in these materials can be beneficial [1]. It has been established that bacteria remaining in the carious lesion may increase pulp sensitivity, inflammation, and secondary caries. The antibacterial activity of dental cements is of particular clinical importance during and after setting, as this property may help to eliminate or reduce bacteria remaining during wall preparation or bacteria that access the cavity through microleakage [2]. Studies have suggested that residual carious lesions in the abutment can be sterilized by covering the abutment with a temporary dressing and antibacterial cements [1].
However, it should be noted that most restorative materials and crowns used in dentistry today do not form a permanent and complete seal with the cavity walls or the remaining tooth structure. In fact, it has been shown that microleakage is not completely prevented in most bonding systems used [3]. Cements, such as glass ionomer cements, are commonly used to fill gaps and act as a sealant between the prepared tooth and the crown. Unfortunately, although cements are used to seal the crown margins, there is still the possibility of bacterial microleakage, which can cause secondary caries and thus compromise the longevity of the restoration.
The antimicrobial properties of glass ionomer cements used in fixed dental prostheses are due to the release of fluoride; however, the fluoride in glass ionomer cements is released only for a short period of time, and the antimicrobial properties of the cement decrease over time [4]. Microleakage is a common clinical phenomenon in which oral fluids, ions, molecules, and bacteria penetrate the restoration-tooth interface and gain access to dentinal tubules and pulp [2]. As mentioned, restoration margins provide a potential route for the leakage of pathogenic microorganisms present in the natural salivary flora [1].
Streptococcus mutans is a major microorganism that initiates caries [5]. Cariogenic bacteria, such as Streptococcus mutans, convert fermentable carbohydrates into acids, which can destroy tooth tissue [2]. Streptococcus mutans is a gram-positive bacterium that is more common in dental plaque than other Streptococcal bacteria. Due to its high tolerance for acidic environments, this bacterium is the dominant species in dental plaque and can quickly cover the tooth surface and, by metabolizing carbohydrates consumed, create an acidic environment that can cause oral and dental diseases, including dental caries. Streptococcus mutans is considered the most important cause of dental caries [6, 7].
The ideal cement has suitable mechanical properties such as high compressive strength, minimal microleakage, low solubility in oral fluids, adhesion, flowability, appropriate film thickness, and sufficient working time. Although a wide range of luting cements is available, there is no luting cement material that possesses all the ideal mechanical properties [8].
Nanotechnology represents the ability to image, manipulate, and model functions at the nanometer scale [9]. Their reduced size boosts the surface area-to-volume ratio, intensifying their environmental interactions and leading to superior antibacterial performance compared to conventional medications [10]. The gradual release of these materials is one of the important properties for their long-term use in cements. In recent years, the incorporation of nanoparticles into dental materials has gained significant attention due to their potential to enhance antimicrobial activity, mechanical strength, and fluoride release [11]. Silver nanoparticles are often associated with their antimicrobial and antioxidant activities [12]. The effect of silver nanoparticles against several microorganisms, including bacteria, fungi, and viruses, has been previously described, indicating their therapeutic potential [13]. Several studies have highlighted the promising role of silver nanoparticles in improving the antibacterial properties of dental materials [14, 15].
Furthermore, the addition of nano-fluorapatite to conventional glass ionomer cement has been shown to improve microhardness and fluoride release while maintaining acceptable biocompatibility [16]. Other investigations have explored the influence of thermo-light curing on the performance of glass ionomer cements, indicating notable improvements in microhardness and material stability [17, 18]. Collectively, these findings support the development of nanoparticle-enhanced cements as a viable strategy for addressing the limitations of traditional materials in preventive and restorative dentistry.
On the other hand, silica nanoparticles have many biological applications due to their excellent biocompatibility, low toxicity, suitable cross-sectional area, and availability [19-21]. In these nanoparticles, properties such as particle size, crystallinity, porosity, and shape are changed with high precision, and this ability has led to these nanoparticles having many uses [22-24]. These nanoparticles are made by the condensation of silanes, which creates an amorphous network of silicon and oxygen. These nanoparticles are used in various fields of medical science [25, 26]. In addition to being nanometric in size, these nanoparticles are also porous, and their pore size is meso (2 to 50 nm), which has multiplied their ability and capability in drug loading and controlled and slow drug release [26]. The incorporation of silver-silica nanoparticles into dental glass materials offers a promising strategy to mitigate microbial infections and biofilm formation, which are common challenges in dental restorations. By reducing the risk of bacterial colonization, these materials can potentially decrease the need for systemic antibiotic therapies, thus minimizing the risks of antibiotic resistance and adverse drug reactions. Furthermore, the antimicrobial and anti-biofilm properties of these nanoparticles contribute to enhanced patient safety by lowering the likelihood of post-operative infections. In this context, understanding the biocompatibility and mechanical stability of these materials is critical to ensuring their safe and effective clinical application.
The aim of the present study is to investigate the effect of adding mesoporous silica nanoparticles containing silver on the safety, antimicrobial, and mechanical properties of glass ionomer cement.
2. MATERIALS AND METHODS
2.1. Sample Size
The sample size for each group, calculated using G*Power software (version 3), was determined to be n = 12 for flexural strength, n = 26 for antimicrobial property tests, and n = 15 for solubility and water absorption tests, based on a significance level of 0.05 and a power of 0.8 [27].
2.2. Inclusion and Exclusion Criteria
All samples without fractures and structural defects were included in the tests. Any sample with any structural defect or failure was excluded.
2.3. Nanoparticles Preparation
To prepare mesoporous silica nanoparticles containing silver, a surfactant mixture (CTAB), distilled water, and sodium hydroxide (NaOH) were stirred at 80°C for 30 minutes on a stirrer. Then, the pH of the solution was adjusted to 12.2. In the next step, tetraethyl orthosilica was added to the solution instantaneously under a 550 rpm stirrer. A white precipitate was obtained, which was mesoporous silica nanoparticles. The prepared nanoparticles were kept at 80°C for two h at room temperature. The silver nanoparticle suspension was prepared separately. The prepared silica nanoparticle powder was added to this material. The resulting mixture was stirred gently on a stirrer for 24 h in a dark place. Transmission Electron Microscopy (TEM) was used to confirm the size and morphology of nanoparticles (JEM-2100F; JEOL, Tokyo, Japan). Enough low electron density was used so as not to destroy the structure.
2.4. Safety of Formulation
Human Foreskin Fibroblast Cells (HFFF2) were used in this study. The cells are normal diploid fibroblasts derived from human foreskin tissue. Characterized cells were purchased from Shahid Beheshti University, Tehran, Iran, and used at passage number 5. Evaluation of cytotoxicity was done by the MTT method at 24, 48, and 72 hrs.
In this test, cells were seeded into 96-well plates and allowed to adhere for 24 h. Subsequently, the material extract was prepared and added to the wells. After 24 h of incubation, the MTT reagent was added to each well and incubated for an additional 4 hours at 37°C. The resulting formazan crystals were dissolved using Dimethyl Sulfoxide (DMSO), and the absorbance was measured at 570 nm using a microplate reader. The percentage of viable cells in the cytotoxicity study was calculated based on the following Eq. (1):
Percentage of viable cells = (Average absorbance of control samples/Average absorbance of treated samples) ×100....(1)
2.5. Antimicrobial and Antibiofilm Properties
The standard strain Streptococcus mutans (ATCC 25175) was acquired from the Pasteur Institute of Iran, located in Tehran. The microbroth dilution approach was employed to assess the antibacterial capability of the nanoparticles by determining both the MIC and the MBC. A nanoparticle suspension was first prepared in distilled water. This suspension was serially diluted and combined with Mueller-Hinton Broth (MHB) in 96-well microtiter plates. The bacterial strain was cultured in MHB and adjusted to a final inoculum of ~1×106 CFU/mL in each well. The plates were incubated at 37 °C for 18–24 hours under aerobic conditions [28].
To test the antimicrobial effect of the cement infused with nanoparticles, the disc diffusion technique was adopted. Cement samples, with and without nanoparticle integration (as negative controls), were molded into 7 mm diameter discs. Mueller Hinton Agar plates were inoculated using a sterile swab dipped into a bacterial suspension standardized to 0.5 McFarland (1.5×10^8 CFU/mL). Swabbing was done in three directions at 60° angles, and the swab was rotated along the plate’s inner circumference to ensure even distribution. Discs made with cement containing 1%, 3%, and 5% nanoparticles and those without nanoparticles were placed on the surface. After a 24-hour incubation at 35°C, the inhibition zones were measured.
Next, the microbroth dilution method was used to determine the minimum inhibitory concentration. Thus, first, 100 μl of Mueller-Hinton Broth culture medium was poured into the wells of a 96-well plate, and 100 μl of the supernatant of the discs was added to the first well of each row, and a dilution (1/2 ratio) was performed in the subsequent wells. For comparison, ciprofloxacin antibiotic discs served as the positive control. Additionally, 100 µL of the bacterial culture was added to each microplate well, with wells containing only water acting as negative controls. Post-incubation at 35°C for 24 hours, wells were inspected for turbidity, indicating microbial growth.
To determine the MBC, the contents of the wells that showed no turbidity (from the MIC test) were transferred to nutrient agar plates and evenly spread on the plates. After incubating the plates at 35°C for 24 hours, the lowest concentration showing no bacterial colonies was recorded as the MBC.
Before examining the anti-biofilm effects of the substance, the biofilm formation ability of the studied bacteria was examined. To examine biofilm formation, a semi-quantitative method for determining biofilm in 96-well microplates with a flat bottom was performed. Initially, a fresh bacterial culture suspension was prepared in TSB medium by overnight incubation, and its turbidity was adjusted to 107 CFU/mL using Optical Absorption (OA) at 600 nm. Biofilm inhibition was examined using the MBIC test. 100 µL of bacterial suspension was dispensed into each well of a 96-well plate and incubated at 37°C for 48 hours. After incubation, the wells were rinsed with phosphate-buffered saline (pH 7.4) and stained with 0.1% crystal violet at room temperature for 30 minutes. Excess stain was removed with water and fixed using 95% ethanol. Absorbance at 570 nm was measured using a spectrophotometer. Wells containing only TSB medium were the negative controls. The experiment was done in triplicate, and average absorbance values were recorded.
For MBIC evaluation, wells were inoculated with a 0.5 McFarland suspension and filled with Mueller-Hinton broth. After 20 hours of incubation at 37°C, the contents were discarded, and the wells were rinsed under sterile conditions. Then, serial concentrations of the test material were added and incubated again for 20 hours. After another wash, 200 µL of plain culture medium was added to each well. Optical Density (OD) readings were taken at 650 nm before and 6 hours after incubation. MBIC was defined as the lowest concentration that caused less than a 10% change in OD compared to the positive control.
2.6. The Solubility Properties and Water Absorption
For sample preparation, the cement specimens were placed in light-shielded containers for an hour, removed from molds, and polished to eliminate surface irregularities using #1 sandpaper in a circular motion. Residual particles were removed with compressed air. After polishing, sample diameters were checked to ensure they remained above 14.8 mm. Specimens were stored in a silica-gel-filled desiccator at 37°C for 22 hours, followed by 2 hours in a second desiccator at 23°C. Samples were weighed to 0.1 mg accuracy, and the drying continued until a constant weight (M1) was reached.
Sample volume was determined using known diameter and height measurements, averaged from perpendicular axes and five-point height checks. Specimens were immersed in distilled water at 37°C for seven days. Afterward, they were rinsed, air-shaken for 15 seconds, and weighed again (M2) one minute after removal from the incubator. After obtaining the M2 value, the drying cycle was repeated for 5 weeks in desiccators containing silica gel, as described, to reach the sample weight at M1. The final, fixed weight of the samples was measured. (M3)
The final volume of the samples was also measured after the samples reached M3 (V2).
The solubility and water absorption rates were obtained according to the formulas 1 and 2 described in the ISO 4049 standard.
Wsp=(M2-M3)/V2 Water absorption....(1)
Wsl=(M1-M3)/V2 Solubility....(2)
2.7. The Flexural Strength
First, samples containing nanoparticles and those without were prepared by mixing the cement powder and liquid according to the manufacturer’s instructions. Then, the samples were placed in an incubator at 37 degrees and 100% relative humidity for one day. After this period, the samples were tested to measure the flexural strength in a Universal testing machine at a speed of 0.5 mm/min. The flexural strength (σ) was calculated in megapascals (MPa) using the following Eqs. (2 and 3):
σ=3FL/2BH....(2)
E=(3FL/4BH)3d....(3)
Where F is the maximum load (N), L is the length of the sample (mm), B is the width of the sample (mm), H is the height of the sample (mm), and d is the deflection (mm) due to the force F [29].
2.8. Statistical Analysis
Considering the normality of the data (obtained from the Schaefer-Wilk test), a one-way ANOVA test was used to compare the safety and antimicrobial effects of the study groups. Tukey's post hoc test was used following the ANOVA test. For the other tests, the t-test was used to compare the studied groups.
3. RESULTS
Figure 1 shows the TEM image of the silver-loaded silica nanoparticles. The size range is below 100 nm, and the quasi-spherical morphology is visible for them. It is also observed that the nanoparticles are relatively aggregated, which is one of the limitations of their use.
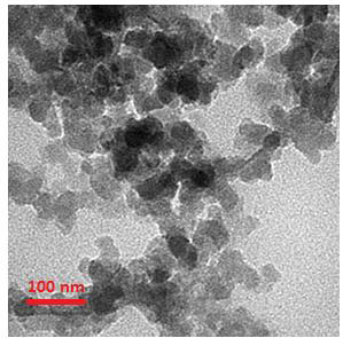
TEM image for the silver-loaded silica nanoparticles.
3.1. Safety of Formulation
Cytotoxicity results of the prepared cement containing silver-loaded silica nanoparticles on human fibroblast cells (HFFF2) showed no toxicity at 24, 48, and 72 hours (Fig. 2).
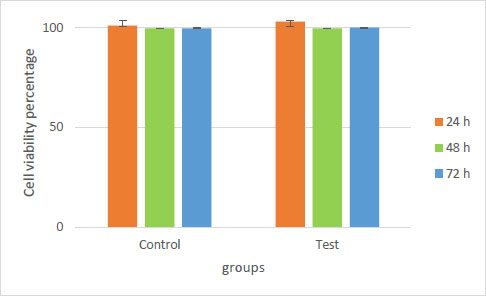
Cytotoxicity results of the cement containing silver-loaded silica nanoparticles on human fibroblast cells (HFFF2).
Statistical analysis showed that there was no significant difference between the groups at any time of 24, 48, and 72 hrs (p=0.5).
3.2. Disk Diffusion Method
The results for the growth inhibition zone, MIC, MBC, and MBIC are summarized in Table 1.
| Groups | Mean inhibition zone (mm)±SD | MIC (mg/ml) ±SD | MBC (mg/ml) ±SD | MBIC (mg/ml) ±SD |
|---|---|---|---|---|
| Glass ionomer cement (0% nanoparticles) | 3±0.81 | 0 | 0 | 0 |
| Glass ionomer cement (1% nanoparticles) | 4.66±1.24 | 341.33±120.67 | 1024 | 1040±11.31 |
| Glass ionomer cement (3% nanoparticles) | 10±1.63 | 170.66±60.33 | 512 | 682.66±241.35 |
| Glass ionomer cement (5% nanoparticles) | 20.33±1.24 | 64±0 | 128 | 512 |
| Ciprofloxacin (positive control) | 25±1.63 | 37.33±19.95 | 43.33±14.63 | 128 |
The results of the one-way ANOVA test showed that there was a significant difference between the growth inhibition zones (p=0.001), MICs (p=0.0001), MBCs (p=0.0001), and MBICs (p=0.0001) of the groups. Tukey's post hoc test showed that the cement group containing 5% nanoparticles had statistically more favorable results than the groups containing 3% and 1% nanoparticles across all four tests: growth inhibition (p = 0.03 and 0.01), MIC (p = 0.001 and 0.02), MBC (p = 0.001 and 0.0001), and MBIC (p = 0.001 and 0.0001), respectively.
The results of the biofilm formation assay in this study indicated that Streptococcus mutans bacteria were capable of forming a strong biofilm. The mean OD values obtained in three replicates and the OD of the negative control, which included a well containing the culture medium used without the presence of antibiotics was 0.678±0.03.
OD ≤ ODc = No biofilm formation (-)
ODc < ODt ≤ 2×Odc = Weak biofilm formation ability (+)
2×ODc< ODt ≤ 4×ODc = Moderate biofilm formation ability (++)
4×ODt >ODc = Strong biofilm formation ability
3.3. The Solubility and Water Absorption Properties
Table 2 shows the results for solubility. The t-test showed that there was no significant difference between the solubility results of cement without nanoparticles and cement containing nanoparticles (p=0.4).
| Samples |
Solubility (The Cement Containing Nanoparticles) |
Mean± SD (The Cement Containing Nanoparticles) |
Solubility (The Cement without Nanoparticles) |
Mean± SD (The Cement without Nanoparticles) |
|---|---|---|---|---|
| 1 | 0.00007 | 0.0001460±0.000 | 0.00017 | 0.0000826±0.000 |
| 2 | 0.00008 | 0.0001 | ||
| 3 | 0.00009 | 0.000095 | ||
| 4 | 0.00005 | 0.000044 | ||
| 5 | 0.00005 | 0.00012 | ||
| 6 | 0.00005 | 0.00011 | ||
| 7 | 0.00006 | 0.00009 | ||
| 8 | 0.00004 | 0.00008 | ||
| 9 | 0.00001 | 0.00016 | ||
| 10 | 0.00006 | 0.00015 | ||
| 11 | 0.00004 | 0.00015 | ||
| 12 | 0.00006 | 0.00012 | ||
| 13 | 0.00008 | 0 | ||
| 14 | 0.00004 | 0 | ||
| 15 | 0.00006 | 0 |
Table 3 shows the results for water sorption. The t-test showed that there was a significant difference between the water absorption results of cement without nanoparticles and cement containing nanoparticles (p=0.02).
| Samples |
Water sorption (The Cement Containing Nanoparticles) |
Mean± SD (The Cement Containing Nanoparticles) |
Water sorption (The Cement without Nanoparticles) |
Mean± SD (The Cement without Nanoparticles) |
|---|---|---|---|---|
| 1 | 0 | 0.00000686±0.000 | 0 | 0.00000226±0.0001 |
| 2 | 0 | 0 | ||
| 3 | 0.000012 | 0 | ||
| 4 | 0.000013 | 0 | ||
| 5 | 0.000013 | 0 | ||
| 6 | 0 | 0.000011 | ||
| 7 | 0 | 0.000012 | ||
| 8 | 0.000012 | 0 | ||
| 9 | 0.000015 | 0 | ||
| 10 | 0.000013 | 0.000011 | ||
| 11 | 0 | 0 | ||
| 12 | 0.000012 | 0 | ||
| 13 | 0 | 0 | ||
| 14 | 0 | 0 | ||
| 15 | 0.000013 | 0 |
3.4. Flexural Strength Results
Tables 4 and 5 show the flexural strength results of cement containing nanoparticles and cement without nanoparticles, respectively. The t-test showed that there was no significant difference between the flexural strength results of cement without nanoparticles and cement containing nanoparticles (p=0.7).
| Samples | a0 | b0 | Stress Conversion Factor | FMax (N) | Max force (MPa) |
Mean± SD (Max force (MPa)) |
|---|---|---|---|---|---|---|
| 1 | 2 | 2 | 3.75 | 5.48 | 20.56 | 14.90±5.58 |
| 2 | 2 | 2 | 3.75 | 6.71 | 25.16 | |
| 3 | 2 | 2 | 3.75 | 5.16 | 19.34 | |
| 4 | 2 | 2 | 3.75 | 4.36 | 16.33 | |
| 5 | 2 | 2 | 3.75 | 4.25 | 15.94 | |
| 6 | 2 | 2 | 3.75 | 3 | 11.26 | |
| 7 | 2 | 2 | 3.75 | 3.43 | 12.87 | |
| 8 | 2 | 2 | 3.75 | 2.57 | 9.62 | |
| 9 | 2 | 2 | 3.75 | 1.99 | 7.47 | |
| 10 | 2 | 2 | 3.75 | 1.58 | 5.92 | |
| 11 | 2 | 2 | 3.75 | 3.69 | 13.82 | |
| 12 | 2 | 2 | 3.75 | 5.49 | 20.59 |
| Samples | a0 | b0 | Stress Conversion Factor | FMax (N) | Max force (MPa) |
Mean± SD (Max force (MPa)) |
|---|---|---|---|---|---|---|
| 1 | 2 | 2 | 3.75 | 5.48 | 48.02 | 17.14±12.86 |
| 2 | 2 | 2 | 3.75 | 6.71 | 23.38 | |
| 3 | 2 | 2 | 3.75 | 5.16 | 12.03 | |
| 4 | 2 | 2 | 3.75 | 4.36 | 6.50 | |
| 5 | 2 | 2 | 3.75 | 4.25 | 13.29 | |
| 6 | 2 | 2 | 3.75 | 3 | 35.20 | |
| 7 | 2 | 2 | 3.75 | 3.43 | 3.77 | |
| 8 | 2 | 2 | 3.75 | 2.57 | 4.12 | |
| 9 | 2 | 2 | 3.75 | 1.99 | 11.03 | |
| 10 | 2 | 2 | 3.75 | 1.58 | 13.64 | |
| 11 | 2 | 2 | 3.75 | 3.69 | 9.72 | |
| 12 | 2 | 2 | 3.75 | 5.49 | 24.98 |
4. DISCUSSION
Glass Ionomer Cements (GICs) are favored in restorative dentistry due to their biocompatibility, fluoride release, and ease of handling. However, their relatively weak antibacterial properties remain a limitation. This study investigated the impact of incorporating silver-loaded mesoporous silica nanoparticles (Ag-MSNs) into GIC and observed a concentration-dependent enhancement in antimicrobial performance, particularly at 5% wt.
The strength of cements is best evaluated by flexural strength testing. This test is the most appropriate measure of the strength of materials because the conventional measurement of compressive strength has no fundamental meaning, and a material can only be destroyed by separation (tensile failure) or sliding of atomic planes (shear failure). Compressive strength is only indirectly and in a complex way related to these failure modes. Therefore, tensile strength measurement is more valid but creates technical problems when applied to brittle materials, and tensile strength measurement by compressive diagonal loading is invalid and only valid if certain requirements are met: for example, the material must not flow plastically, otherwise the theory is not applicable [30].
The disc diffusion, MIC, MBC, and MBIC tests consistently showed that the 5% Ag-MSN group outperformed the 3% and 1% groups, aligning with findings from a study, which also reported significant antibacterial benefits of AgNP-modified GICs against S. aureus [31]. However, the study’s results are further supported by other studies using various nanoparticles. For instance, curcumin [32], zinc oxide [33], and chitosan [34] nanoparticles have all demonstrated antibacterial enhancement when incorporated into GICs or other cements. The inclusion of different types of nanoparticles in glass ionomer cements has been studied with mixed outcomes. For instance, in a study evaluating zinc oxide nanoparticles incorporated into both self-cured and resin-modified GICs, no significant antimicrobial activity was observed against S. mutans at 1% and 2% concentrations, even after extended biofilm maturation periods [33]. This contrasts with the study’s findings, which showed that silver-loaded mesoporous silica nanoparticles demonstrated a clear dose-dependent antibacterial and antibiofilm effect, particularly at 5% concentration. The discrepancy may be attributed to differences in nanoparticle composition, release kinetics, or the higher antimicrobial potency of silver ions compared to zinc. Additionally, alternative strategies such as the incorporation of chitosan into the polyacrylic acid component of GICs have shown promise in enhancing antibacterial efficacy without compromising dentin bond strength [34]. These findings support the notion that chemical modification of GIC formulations can yield antimicrobial benefits, although the underlying mechanisms, whether via ion release, pH alteration, or biofilm interference, vary significantly among additives [35]. In this study’s case, the encapsulation of silver within mesoporous silica may have enhanced ion-controlled release while minimizing aesthetic compromises and preserving mechanical properties. This broader context reinforces the validity of using nanostructures to improve the biological performance of dental materials.
Notably, the improved efficacy of the 5% group may be attributed to the optimized surface area and controlled silver release enabled by the mesoporous silica framework. The mesoporous structure provides a sustained antimicrobial effect by allowing gradual silver ion diffusion, which disrupts bacterial membranes, generates Reactive Oxygen Species (ROS), and inhibits enzymatic systems [34]. Further mechanistic studies using molecular techniques such as gene expression profiling or ROS quantification could better clarify this interaction.
Regarding physical properties, while solubility was not significantly affected by nanoparticle addition, water absorption was significantly increased in the modified groups. Although this result aligns with reports from other nanocomposite systems, the clinical implications of higher water uptake should be considered cautiously. Increased water sorption could lead to long-term degradation of the matrix, dimensional instability, or reduced durability. Further testing under thermocycling or long-term storage would be beneficial to simulate intraoral conditions.
One key consideration often overlooked is aesthetics. Silver nanoparticles are known to cause discoloration in restorative materials, potentially limiting their use in visible areas [31]. The study’s approach, which embeds silver within mesoporous silica, may reduce this drawback, as hypothesized. However, this benefit was not directly measured in this study. Future work should include colorimetric analysis to quantify any improvements in shade stability or translucency.
5. LIMITATIONS OF THE STUDY
This was an in vitro study, which does not fully replicate the complex conditions of the oral environment, so in vivo validation is needed. The long-term biocompatibility and potential toxicity of silver nanoparticles were not assessed beyond the MTT assay. Mechanically, only a few properties, such as water absorption and flexural strength, were evaluated, leaving out other critical parameters. Additionally, the antibacterial tests involved a limited number of microbial strains, which may not fully represent oral microbial diversity. The control group (cement without nanoparticles) showed a negligible growth inhibition zone, attributed to fluoride release, but this was not quantified, suggesting the need to test in future experiments.
CONCLUSION
This study demonstrates that incorporating 5% silver-loaded mesoporous silica nanoparticles into glass ionomer cement significantly enhances its antimicrobial and antibiofilm properties without adversely affecting mechanical strength or solubility. While water absorption increased with nanoparticle addition, it remained within manageable limits, though long-term effects warrant further study. The use of mesoporous silica as a delivery platform not only appears to preserve the aesthetic properties better than silver-only additives but also offers a controlled release mechanism for silver ions, potentially enhancing longevity and reducing bacterial resistance. These findings highlight the potential of Ag-MSN-enriched GICs in clinical settings where antimicrobial protection is critical, such as in high-caries-risk patients or under crowns and bridges. However, before clinical application, additional studies are necessary to confirm long-term biocompatibility, assess aesthetic outcomes, and evaluate performance under simulated oral conditions. Broader microbial testing and advanced imaging or molecular techniques may also provide deeper insights into the antimicrobial mechanisms and stability of the material. In conclusion, this nanoparticle-modified cement shows promise as a next-generation restorative material that addresses microbial challenges while maintaining key physical and mechanical properties. It offers a balanced approach toward safety, efficacy, and potentially improved patient outcomes in restorative dentistry.
RECOMMENDATIONS
Additional studies are needed to evaluate the biocompatibility and other properties of this cement with a large number of samples in the animal and clinical phases to prove the functionality of this new material.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: S.D.: Study conception and design; Y.R., S.B.: Data collection; A.K.: Data Analysis or Interpretation; R.N., S.S.: Methodology. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| OD | = Optical Density |
| GICs | = Glass Ionomer Cements |
| MIC | = Minimum Inhibitory Concentration |
| MHB | = Mueller-Hinton Broth |
ETHICAL STATEMENT
Ethics approval was obtained from Ethics Committee of Tabriz University of Medical Sciences, Iran (IR.TBZMED.DENTISTRY.REC.1403.013).
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [R.N], on a reasonable request.
FUNDING
The Vice Chancellor for Research at Tabriz University of Medical Sciences provided support with grant number: 73234.
CONFLICT OF INTEREST
Drs. Solmaz M. Dizaj and Simin Sharifi are the Editorial Board members of The Open Dentistry Journal.
ACKNOWLEDGEMENTS
The author greatly acknowledges support provided by Vice Chancellor for research at Tarbiz University of Medical Science.

