All published articles of this journal are available on ScienceDirect.

Examining Dentists' Awareness, Perspectives, and Integration of Artificial Intelligence in Dental Practice: A Cross-Sectional Study in Saudi Arabia
Abstract
Introduction
As Artificial Intelligence (AI) continues to transform patient care and the overall healthcare sector, assessing dentists’ awareness and utilization of these technologies is essential to understanding the current landscape of integration in dental practice in Saudi Arabia.
Methods
A cross-sectional quantitative research was conducted, utilizing a structured, 37-item validated questionnaire, distributed to 375 practicing dentists in Saudi Arabia. Proportionate stratified sampling was employed to ensure that the sample size for each region (North, South, East, West, and Central) was proportional to its population relative to the total population.
Results
Majority of dentists (66.9%) are partially aware of the basic principles of AI, while 10.1% reported no awareness. AI Knowledge acquisition was primarily gained through self-learning, according to 38.4%. Dentists utilize AI mostly in research (15.92%); however, the main concern regarding AI integration, according to 31.5%, is cost. Statistically significant regional differences were observed in participants’ knowledge and experience (p = 0.017) and for perceptions and attitudes towards AI (p = 0.008). There were no significant differences based on other parameters such as age, gender, specialty, and employment history.
Discussion
The findings indicate moderate AI awareness among dentists, with most knowledge gained through self-learning and limited formal training. AI use remains primarily research-oriented, reflecting early integration stages and cost-related barriers. Significant regional variations suggest uneven access to AI resources and education, while demographic factors showed no notable influence. These results highlight the need for structured AI curricula and continuing education to enhance competency and promote equitable integration of AI technologies in dental practice across Saudi Arabia.
Conclusion
Dentists' knowledge, application, perceptions, and attitudes toward AI in Saudi Arabia were generally consistent across factors such as age, gender, education level, specialty, occupation, and experience. However, significant regional differences were observed.
1. INTRODUCTION
In 1959, Professor John McCarthy envisioned designing a computer program capable of receiving, processing, reasoning, and learning from data to identify logical patterns [1, 2]. The evolution of AI continued over the years, transitioning from an idea and a vision to an independent discipline with numerous applications across various sectors. According to current standards, AI is a machine-based system that analyzes input to generate outputs such as decisions, recommendations, and content, with varying degrees of autonomy [3]. It encompasses various areas, including machine learning, deep learning, natural language processing, knowledge representation, computer vision, cognitive computing, and reasoning [4, 5].
Machine learning is the process of learning through data input by algorithms capable of identifying statistical patterns and structures, while deep learning is a more complex machine learning technique utilizing deep neural networks capable of learning complex data [4, 6, 7]. Deep neural networks can perform function approximation and input mapping of dental radiographs, for example, to generate outputs where oral diseases and findings are accurately identified. Presently, AI models can identify and diagnose dental caries, root fractures, periodontal disease, peri-apical lesions, maxillofacial cysts, osteoporosis, oral cancer, predict orthodontic extractions, and determine age and gender [8].
Dentists diagnose and treat oral diseases based on visual, tactile, and radiographic assessments combined with patients’ histories. This subjective assessment method relies on the dentists’ experience and knowledge and is subject to bias and misdiagnosis, leading to compromised clinical outcomes. Incorporating AI into oral disease detection, diagnosis, treatment planning, and prognosis can significantly improve the efficiency of the overall journey and provide dentists with supplementary evaluation, offering assistance and personalized recommendations to each patient [4, 9]. A recently published systematic review revealed that the precision and accuracy of dental AI systems were comparable to those of trained specialists, as reported in some studies [8]. Moreover, the authors noted that in other studies, these AI systems surpassed specialists in terms of accuracy and proficiency. Predictive analytics is an additional valuable feature in AI, using algorithms that can predict treatment outcomes in addition to patients’ risk of developing oral diseases such as caries, periodontal diseases, and oral cancer [10].
Processing big data using AI can help identify patterns related to oral health, aiding researchers in understanding disease cycles on a global scale, their impact, and associated risks and treatment options [9]. However, it is essential to remain mindful of the ethical and legal issues that users of these developing technologies still encounter. These challenges encompass data privacy, algorithmic bias, maintaining data quality, integration difficulties, and data enhancement [5, 9]. The Academy of Medical Sciences emphasizes that AI in medicine and dentistry must achieve a certain level of efficiency to improve the quality of services offered [11].
Facilitating access and utilization of AI within dental care can be accomplished through educational institutions and organizations by implementing educational programs and specialized courses. However, it is important to promote adherence to ethical guidelines related to AI, as the integration of such technology must be approached with caution. Although challenges remain, the potential benefits of AI are substantial, thereby requiring a collective effort to bridge the gap between technology and practice.
Recent surveys on AI in dentistry consistently report high interest and perceived value in diagnosis and treatment planning, alongside barriers such as cost, training needs, and data privacy concerns; willingness to adopt is generally strong across countries [6, 12, 13]. However, much of this literature samples students, interns, or mixed learner cohorts, offering limited insight into practicing dentists [14-16], and minimal region-level comparisons within Saudi Arabia Published work from Saudi Arabia has largely focused on students and provides few data on dentists’ AI literacy stratified by specialty, experience, age, gender, or region, leaving a gap in profession-level, regionally representative evidence [14, 17].
To address this gap, the present cross-sectional study aims to assess dentists’ awareness, perception, and utilization of AI in clinical practice. Using proportionate stratified sampling across all five regions, it aims to highlight the variation by demographic and professional characteristics and to establish an evidence-based view of AI adoption in everyday dental practice.
2. MATERIALS AND METHODS
This study utilized a cross-sectional quantitative research design to assess the perceptions, knowledge, attitudes, and applications of AI among practicing dentists in Saudi Arabia. A structured questionnaire was developed and distributed to participants, covering various topics related to AI awareness, application, and perceived challenges. The survey focused on understanding how AI is currently used in dental practices and identifying the areas where it has the greatest potential. The study received approval from the Institutional Review Board (IRB) at Princess Nourah bint Abdulrahman University (IRB approval number: 24-0686).
2.1. Participants and Sampling
The sample consisted of dental professionals selected using a stratified random sampling method, ensuring diverse representation across various geographical regions. Participants' demographic and professional characteristics, including age, gender, level of education, specialty, and years of experience, were analyzed to provide a comprehensive overview of the study population. The survey targeted professionals from all regions of Saudi Arabia (North, South, East, West, and Central) (Table 1), with varying levels of experience in both private and public sectors, as well as academic institutions. These variables were included to allow comparisons across commonly studied factors that may influence AI adoption in healthcare settings.
| Region | Population | Sample |
|---|---|---|
| Central Region | 10785 | 166 |
| Eastern Region | 3252 | 57 |
| Northern Region | 943 | 30 |
| Southern Region | 2455 | 36 |
| Western Region | 7159 | 86 |
| Total | 24594 | 375 |
A representative sample size was calculated based on the reported population size [18], using Steven Thompson’s finite-population formula for a single proportion, with a 95% confidence level (Z = 1.96), assumed proportion p = 0.50, and margin of error = ±5.0%. This yielded a required sample size of n = 375. Per region, sample sizes were then calculated and stratified from the national total using proportional allocation from the regional population. This enabled regional-level comparisons of dental professionals across Saudi Arabia.
2.2. Data Collection
A self-administered online questionnaire was used as the primary data collection tool. The inclusion criteria comprised all practicing dentists in Saudi Arabia. Major universities across all regions of Saudi Arabia were formally contacted and requested to assist in disseminating the questionnaire through their faculty, student, and alumni networks. In addition, the survey link was circulated through professional dental groups via email and online platforms to ensure broad coverage. This strategy aimed to achieve responses from all geographic regions and across demographic groups, including age, gender, years of experience, and type of practice.
A cover page was included in the questionnaire, providing participants with information about the study's objectives and informed consent to access and complete the survey. Those who declined or failed to complete the questionnaire, as well as non-practicing dentists, were excluded from the study.
The questionnaire was developed by the author based on a targeted review of surveys on AI in dentistry and informatics. The questionnaire consisted of 37 items, including close-ended questions and statements, structured into three sections. The first section collected demographic information such as age, gender, level of education, specialty, years of experience, occupation, geographical region of employment, and past experiences. The second section focused on knowledge and experience with AI, asking participants about their awareness of basic AI principles, learning methods, and areas of application within their practice. Following this, participants responded to nine statements, indicating their level of agreement using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The third section gathered data related to attitudes and perceptions about AI, to evaluate participants' attitudes towards AI’s role in clinical practice, education, and research, as well as its potential to add value to their work. Participants responded to 15 statements, indicating their level of agreement using a Likert scale.
2.3. Validity and Reliability of the Study Measures
Face and content validation were assessed through a pilot study in which ten practicing dentists completed the questionnaire and provided feedback on clarity, grammar, logic, flow, and syntax to ensure the reliability and validity of the questionnaire. Based on this feedback, a few items were rephrased for clarity, and some were rearranged for better flow. Data collection took place from April 2024 to August 2024.
The correlation coefficient between the statements and the total scale in the questionnaire ranges from 0.535 to 0.904, indicating a positive direct relationship between each item on the scale and the total scale. This suggests a high level of internal consistency, confirming that the results obtained are statistically reliable. Cronbach's alpha for the total items of the questionnaire was 0.966, which indicates a high level of reliability for the questionnaire items. Full reliability testing was not repeated, as the post-revision modifications did not affect the structure or meaning of the questionnaire items.
2.4. Statistical Analysis
Analyses were performed using IBM SPSS Statistics (Version 21). Descriptive statistics (frequencies, percentages, means, and standard deviations) were calculated. Differences across statements regarding knowledge and experience, as well as perceptions and attitudes, were examined using the Friedman test, with Kendall’s W reported as the effect size. When significant, Wilcoxon signed-rank tests with Holm–Bonferroni correction were conducted for pairwise comparisons. Between-group differences (e.g., gender, age, region, specialty) were assessed using the Mann–Whitney U test for two-group variables and the Kruskal–Wallis test for variables with three or more groups.
Mean scores for each item were also ranked descriptively to illustrate relative priorities across AI applications and challenges. Composite mean scores were calculated to summarize overall knowledge, perceptions, and attitudes toward AI.
In addition, multiple linear regression analyses were conducted using composite knowledge and attitude scores as dependent variables, with gender, age, region, specialty, level of education, years of experience, occupation, and past employment entered simultaneously as predictors to adjust for potential confounding.
3. RESULTS
3.1. Demographic Data
The sample is nearly evenly split (Fig. 1), with females accounting for 52.3% and males for 47.7%. The majority of participants fall between the ages of 41 and 50, representing 33.6% of the sample, followed by 26.9% who are aged 51-60. A smaller group, 20.8%, belongs to the 30-40 age range, while 13.3% are over 60 years old. Participants under the age of 30 make up the smallest portion, comprising only 5.3% of the total sample.
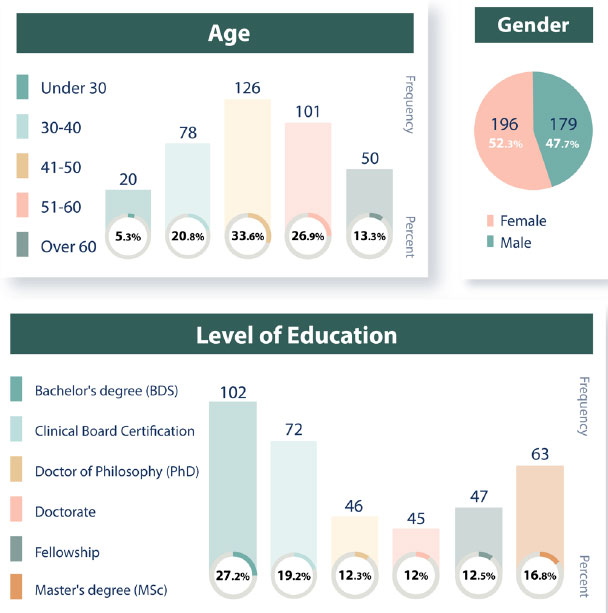
Demographic profile of the study sample, including age, gender, and level of education.
A significant proportion of participants hold a Bachelor's degree (BDS), representing 27.2% of the total, with 19.2% holding Clinical Board Certification and 12.5% having completed a Fellowship. Additionally, 16.8% have earned a Master's degree (MSc), and participants with a Doctorate (12.0%) and PhD (12.3%) form nearly equal groups.
Aside from general dentistry, which accounts for 30.7% of participants, notable specialties include Pedodontics (11.5%), Orthodontics (10.9%), and Periodontics (8.5%) (Fig. 2). Less common fields, such as Oral and Maxillofacial Surgery (OMFS), Endodontics, and Oral Pathology, represent 2.4%, 3.5%, and 3.5% of participants, respectively.
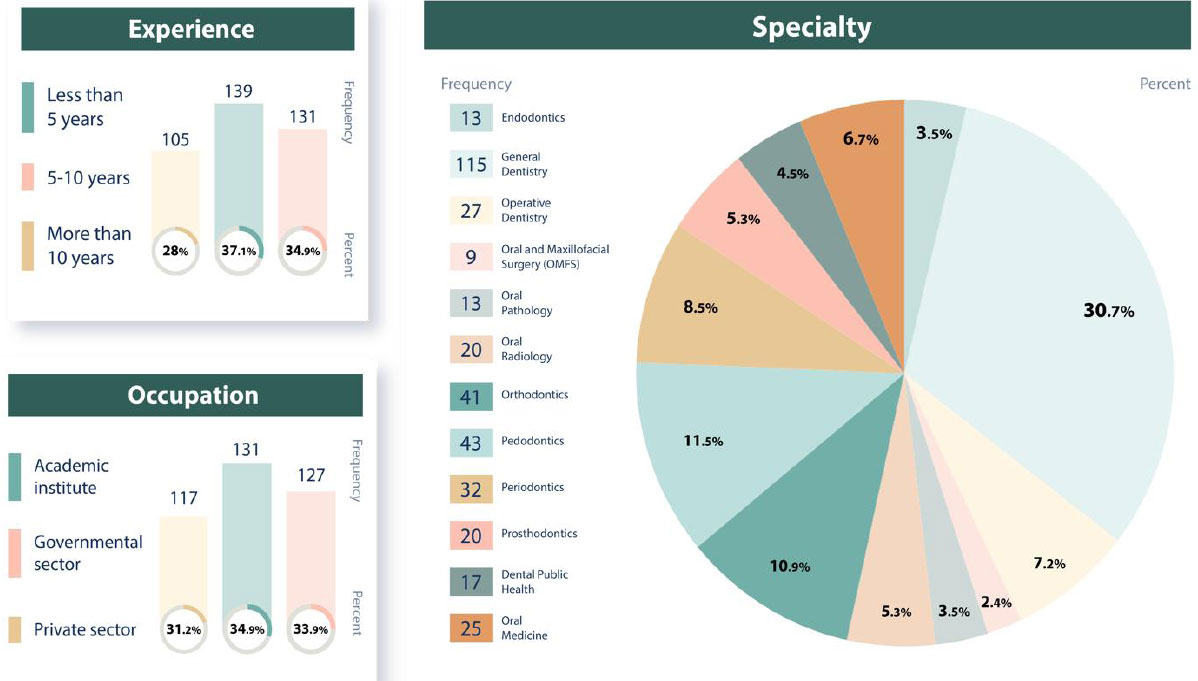
Demographic profile of the study sample, including occupation, experience, and specialty.
Participants working in academic institutions comprised 34.9% of participants, followed closely by those in the governmental sector (33.9%). A smaller proportion, 31.2%, is employed in the private sector. In terms of years of practicing dentistry, 37.1% of participants have less than 5 years of experience, while 34.9% have been practicing for 5-10 years. The remaining 28.0% have been practicing for more than 10 years.
Geographically, 44.3% of participants are from the Central Region (Fig. 3). The Western Region is home to 22.9% of participants, while the Eastern Region comprises 15.2%. The Southern Region (9.6%) and Northern Region (8.0%) have smaller representations. This regional distribution is representative of practicing dental professionals relative to each region's overall population.
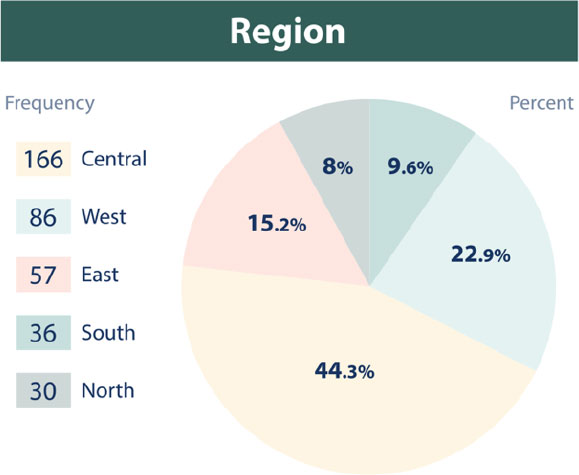
Regional distribution of the study sample.
Regarding participants' employment history (Fig. 4), the majority of participants (57.1%) have previously worked in 1-2 institutions or organizations, the majority (57.1%) reported having worked in 1-2 institutions, while 19.2% indicated no prior work experience. A smaller portion (5.6%) was affiliated with 5 or more institutions, and 18.1% have worked in 3-4 institutions. The majority had previous employment in Saudi Arabia (59.90%). Additionally, 11.02% of participants worked in other parts of the Middle East, while 10.15% had experience in Asia. Europe accounts for 6.20% of past employment, followed by North America with 3.79% and Africa with 3.10%. A small portion (4.65%) reported no prior work experience, and minimal representation is seen in South America (0.69%) and Australia (0.52%).

History of previous employment of the study sample.
3.2. Dentists’ Knowledge and Experiences with AI
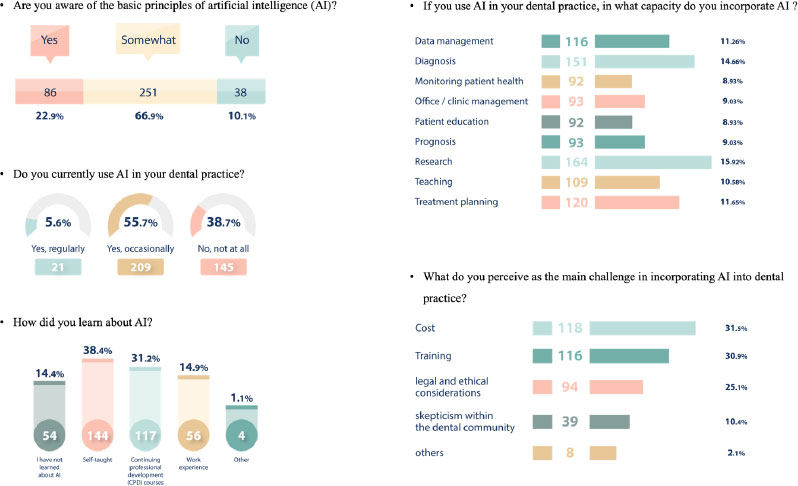
Regarding dental practitioners' knowledge and experience with AI (Fig. 5), the results show that the majority (66.9%) are somewhat aware of the basic principles of AI. However, only 22.9% of participants have a full understanding of AI principles, while 10.1% reported no awareness at all. In practice, 55.7% of participants use AI occasionally, indicating a moderate level of adoption. Conversely, 38.7% do not use AI at all. Only 5.6% of participants reported using AI regularly, demonstrating a relatively low rate of consistent AI use in dental practices.
Knowledge and experience of the study sample with AI.
Regarding how participants learned about AI, 38.4% gained knowledge through self-learning, indicating a strong inclination toward independent study. Meanwhile, 31.2% acquired their AI knowledge through Continuing Professional Development (CPD) courses. A smaller portion (14.9%) reported learning about AI through work experience, while 14.4% had not learned about AI at all.
Furthermore, research is the most common application of AI, accounting for 15.92%, followed by diagnosis at 14.7%, and treatment planning at 11.7%. Other notable capacities include data management (11.3%), teaching (10.6%), office/clinic management (9.0%), prognosis (9.0%), and monitoring patient health and patient education (both at 8.9%), demonstrating that AI is used in a broad range of clinical, administrative, and educational functions within dentistry.
The primary concern regarding the adoption of AI in dental practice, cited by 31.5% of participants, is cost. This is closely followed by concerns about training, reported by 30.9% of respondents, highlighting a substantial need for education and skill development in AI among dental professionals. Legal and ethical considerations were also significant, with 25.1% of respondents raising concerns around compliance, privacy, and the ethical use of AI. Additionally, skepticism within the dental community was noted by 10.4% of respondents, reflecting doubt or hesitation about the role and benefits of AI in dental practice. A smaller percentage (2.1%) cited “Other” challenges, which included issues such as competition, field-specific indications, reliability, and bureaucratic delays in accessing new technologies.
Participants' responses regarding their level of agreement on the various applications of AI in dental practice are illustrated in Table 2, with responses measured on a scale from 1 to 5. Rankings are presented descriptively to illustrate relative tendencies and patterns in responses. The statements cover different potential uses of AI, ranging from diagnostic tools to treatment planning and risk prediction. Each statement is rated based on its mean score, indicating the extent of agreement, along with its standard deviation and the ranking of importance for each application. This provides insight into how AI is perceived in terms of its practical utility in dentistry.
| S.No. | Statement | Mean | Std. Deviation | Importance |
|---|---|---|---|---|
| 1 | AI can be used in the automated interpretation of dental images, e.g., intra-oral radiographs, CBCT, and Cephalometry) | 3.87 A, C | 1.37 | 3 |
| 2 | AI can be used in early disease detection | 3.86 A, C, D | 1.36 | 4 |
| 3 | AI can be used in caries detection and diagnosis | 3.88A,C | 1.35 | 2 |
| 4 | AI can be used in the detection of periodontal disease | 3.72B | 1.32 | 8 |
| 5 | AI can be used in the detection of oral lesions, such as oral cancer | 3.7 B | 1.37 | 9 |
| 6 | AI can be used in treatment planning. (e.g., smile design and implant placement) | 3.95 A | 1.34 | 1 |
| 7 | AI can be used in forensic dentistry | 3.79 B, C | 1.33 | 5 |
| 8 | AI can be used as a prognostic tool | 3.73 B, D | 1.36 | 7 |
| 9 | AI can predict patient-specific risks (e.g., caries, periodontal disease, and oral cancer) | 3.74 B | 1.32 | 6 |
| General Tendency | 3.80 | 1.24 | ||
Note: different superscript letters indicate significant differences between statements, adj. p<0.01.
Mean scores for AI applications were generally consistent, but differences were observed (Friedman χ2(8)=72.47, p<0.001; Kendall’s W=0.024). The highest mean score is (3.95 out of 5), indicating that participants consider AI to be especially useful in treatment planning (e.g., smile design and implant placement), which was ranked as the most important use (rank 1). Following this, utilizing AI for caries detection and diagnosis was rated second in importance, with a mean of (3.88 out of 5). On the other hand, AI's role in detecting oral lesions such as oral cancer was rated the lowest in importance, with a mean of (3.7 out of 5).
3.3. Dentists’ Perceptions and Attitudes Towards AI
An overview of dental professionals' attitudes and perceptions regarding the role and value of AI in dentistry is shown in Table 3, with responses measured on a scale from 1 to 5. Rankings are presented descriptively to illustrate relative tendencies and patterns in responses. Mean scores for attitudes and perceptions were closely clustered (3.38-3.86), but differences were observed (Friedman χ2(14)=143.9, p<0.001; Kendall’s W=0.027). The highest mean score (3.86 out of 5) indicates that participants are most keen to learn and apply AI in their practice (rank 1). This demonstrates a strong professional interest in adopting AI technology. Participants closely agree that AI should be included in postgraduate training (mean 3.84 out of 5, rank 2), underscoring the importance of formal AI education for advanced professionals.
| S.No. | Statement | Mean | Std. Deviation | Importance |
|---|---|---|---|---|
| 1 | AI plays an important role in dental practice | 3.67A, B, C, D | 1.29 | 9 |
| 2 | Dentists should rely more on AI in dental diagnosis | 3.62 A, B, C, D | 1.36 | 13 |
| 3 | Dentists should rely more on AI in dental treatment planning | 3.66 A, B, C, D | 1.37 | 10 |
| 4 | Dentists should rely more on AI as a prognostic tool | 3.63 A, B, C, D | 1.38 | 12 |
| 5 | Dentists should rely more on AI in knowledge acquisition | 3.66 A, B, C, D | 1.37 | 11 |
| 6 | Dentists should rely more on AI in research | 3.78B, C | 1.35 | 6 |
| 7 | AI must be used as a supplementary tool only | 3.83B, C | 1.33 | 3 |
| 8 | AI is superior to human intelligence and critical thought processes | 3.38A,D | 1.47 | 15 |
| 9 | AI should be an integral part of clinical dental practice | 3.69 A, B, C, D | 1.35 | 8 |
| 10 | AI should be included in undergrad training | 3.7 A, B, C, D | 1.35 | 7 |
| 11 | AI should be included in postgrad training | 3.84B, C | 1.35 | 2 |
| 12 | AI in the medical/dental fields violates ethical principles of confidentiality | 3.51D | 1.40 | 14 |
| 13 | AI will revolutionize dental practice. | 3.81B, C | 1.33 | 4 |
| 14 | I believe that AI will add value to my practice | 3.8B, C | 1.37 | 5 |
| 15 | I am keen to learn and apply AI in my practice. | 3.86B | 1.37 | 1 |
| General Tendency | 3.70 | 1.21 | ||
Note: different superscript letters indicate significant differences between statements, adj. p<0.01.
The third-highest score (3.83 out of 5) supports the notion that AI should be used as a supplementary tool only (rank 3), suggesting that participants view AI as an aid to, rather than a replacement for, human expertise. On the other hand, the statement that AI is superior to human intelligence received the lowest mean score of (3.38 out of 5) (rank 15), indicating that participants do not view AI as superior to human cognitive abilities.
3.4. Differences in Knowledge and Experiences in Addition to Attitudes and Perceptions Towards AI in Dental Practice
Knowledge and experience, in addition to perceptions and attitudes of dental practitioners towards AI, did not significantly differ based on age (p= 0.65 and 0.25) (Table 4). Upon assessing knowledge and experience, the highest mean score is observed for participants aged 51-60 (mean = 3.92 ± 1.21), followed by those aged over 60 (mean = 3.78 ± 1.3), indicating that older participants tend to apply AI more positively in their dental practices. Participants aged 41-50 have a mean score of 3.69 ± 1.15, and those aged 30-40 show a slightly lower mean of 3.55 ± 1.17. The youngest group, under 30, has the lowest mean score (3.02 ± 1.37), suggesting they may be less experienced or familiar with AI in dental practice. Dentists’ perceptions and attitudes vary across age groups, with participants aged 51-60 showing the highest mean (3.92 ± 1.21), indicating a stronger agreement on the value and role of AI in dentistry compared to other age groups. The 30-40 age group has a lower mean score of 3.55 ± 1.17, and the under 30 age group has the lowest mean score of 3.02 ± 1.37, suggesting a lower perception of AI’s role in their dental practices.
| - | - | Knowledge and Experience | Attitudes and Perceptions | ||
|---|---|---|---|---|---|
| - | Variable | Mean | Std. Deviation | Mean | Std. Deviation |
| Region | Central Region | 3.92 | 1.08 | 3.78 | 1.09 |
| Eastern Region | 3.64 | 1.22 | 3.47 | 1.17 | |
| Norther Region | 3.14 | 1.49 | 3.09 | 1.45 | |
| Southern Region | 3.79 | 1.44 | 3.6 | 1.35 | |
| Western Region | 3.93 | 1.29 | 3.93 | 1.25 | |
| Total | 3.80 | 1.24 | 3.70 | 1.21 | |
| - | - | f = 3.038 sig = 0.017 | f = 3.539 sig = 0.008 | ||
| Gender | Female | 3.80 | 1.26 | 3.69 | 1.19 |
| Male | 3.81 | 1.22 | 3.70 | 1.24 | |
| - | - | t = 0.093 sig = 0.926 | t = 0.105 sig = 0.916 | ||
| Age | Under 30 | 3.02 | 1.37 | 3.02 | 1.37 |
| 30-40 | 3.55 | 1.17 | 3.55 | 1.17 | |
| 41-50 | 3.69 | 1.15 | 3.69 | 1.15 | |
| 51-60 | 3.92 | 1.21 | 3.92 | 1.21 | |
| Over 60 | 3.78 | 1.30 | 3.78 | 1.30 | |
| Total | 3.70 | 1.21 | 3.70 | 1.21 | |
| - | - | f = 2.235 sig = 0.65 | f = 2.813 sig = 0.25 | ||
| - | Bachelor's degree (BDS) | 3.68 | 1.17 | 3.47 | 1.11 |
| Level of Education | Clinical Board Certification | 3.85 | 1.27 | 3.71 | 1.25 |
| Doctor of Philosophy (PhD) | 3.72 | 1.15 | 3.63 | 1.10 | |
| Doctorate | 3.93 | 1.11 | 3.80 | 1.11 | |
| Fellowship | 3.98 | 1.42 | 3.99 | 1.34 | |
| Master's degree (MSc) | 3.79 | 1.34 | 3.81 | 1.35 | |
| - | Total | 3.80 | 1.24 | 3.70 | 1.21 |
| - | - | f = 0.553 sig = 0.736 | f = 1.473 sig = 0.198 | ||
| Specialty | Endodontics | 4.23 | 0.72 | 3.83 | 0.84 |
| General Dentistry | 3.83 | 1.13 | 3.65 | 1.10 | |
| Operative Dentistry | 3.64 | 1.29 | 3.38 | 1.39 | |
| Oral and Maxillofacial Surgery | 3.72 | 1.13 | 3.66 | 1.17 | |
| Oral Pathology | 3.60 | 1.46 | 3.50 | 1.35 | |
| Oral Radiology | 3.56 | 1.47 | 3.58 | 1.36 | |
| Orthodontics | 3.87 | 1.44 | 3.95 | 1.29 | |
| Pedodontics | 3.91 | 1.22 | 3.85 | 1.22 | |
| Periodontics | 3.72 | 1.32 | 3.68 | 1.29 | |
| Prosthodontics | 3.67 | 1.02 | 3.55 | 1.11 | |
| Dental Public Health | 3.65 | 1.41 | 3.60 | 1.39 | |
| Oral Medicine | 3.98 | 1.35 | 3.94 | 1.31 | |
| Total | 3.80 | 1.24 | 3.70 | 1.21 | |
| f = 0.440 sig = 0.938 | f = 0.594 sig = 0.834 | ||||
| Experience | Less than 5 years | 3.78 | 1.35 | 3.64 | 1.33 |
| From 5 to 10 years | 3.81 | 1.23 | 3.75 | 1.20 | |
| More than 10 years | 3.82 | 1.09 | 3.71 | 1.07 | |
| Total | 3.8 | 1.24 | 3.70 | 1.21 | |
| - | - | f = 0.048 sig = 0.953 | f = 0.249 sig = 0.780 | ||
| Occupation | Academic institute | 3.78 | 1.24 | 3.71 | 1.20 |
| Governmental sector | 3.81 | 1.27 | 3.67 | 1.25 | |
| Private sector | 3.82 | 1.21 | 3.71 | 1.19 | |
| Total | 3.80 | 1.24 | 3.70 | 1.21 | |
| - | - | f = 0.034 sig = 0.967 | f = 0.037 sig = 0.963 | ||
| Past work experience | 1-2 institutions or organizations | 3.90 | 1.22 | 3.82 | 1.19 |
| 3-4 institutions or organizations | 3.73 | 1.21 | 3.54 | 1.20 | |
| 5 or more institutions or organizations | 3.38 | 1.35 | 3.45 | 1.32 | |
| No prior work experiences | 3.71 | 1.28 | 3.55 | 1.23 | |
| Total | 3.80 | 1.24 | 3.70 | 1.21 | |
| - | - | f = 1.485 sig = 0.218 | f = 1.761 sig = 0.154 | ||
Results additionally indicate no significant differences based on gender (p = 0.926 and 0.916). The mean scores for both females (3.80 ± 1.26) and males (3.81 ± 1.22) are very close, indicating no significant difference in knowledge and application of AI in dental practice. Additionally, there are minimal differences between male and female attitudes and perceptions of the role and value of AI in dentistry. The mean score for females is 3.69 with a standard deviation of 1.19, while the mean score for males is 3.70 with a standard deviation of 1.24.
Regarding educational level, no significant differences were observed between sample groups (p = 0.74 and 0.19). Assessment based on AI knowledge and experience showed that participants holding a Fellowship had the highest mean score (3.98 ± 1.42), suggesting they perceive AI more positively in dental practices, followed closely by those with a Doctorate (3.93 ± 1.11). Participants with a Clinical Board Certification have a mean score of 3.85 ± 1.27, while those with a Master's degree (MSc) have a mean score of 3.79 ± 1.34. Participants with a PhD hold a mean score of 3.72 ± 1.15, and those with a Bachelor's degree (BDS) have the lowest mean score (3.68 ± 1.17).
The highest mean score (3.99 ± 1.34 out of 5) is observed among participants with a Fellowship upon assessing perceptions and attitudes of dental practitioners, suggesting that this group perceives AI as highly valuable in their practice. Those with a Master's degree (3.81 ± 1.35) and a Doctorate (3.80 ± 1.11) also show relatively high agreement on the importance of AI. Participants with Clinical Board Certification (3.71 ± 1.25) and a PhD (3.63 ± 1.10) have slightly lower perceptions of AI's value, but still generally positive. Participants with a Bachelor's degree (BDS) showed the lowest rating among all participants (3.47 ± 1.11).
Knowledge and experiences, in addition to perceptions and attitudes of dental practitioners towards AI, did not significantly differ based on specialty (p = 0.938 and 0.834). Upon investigating the knowledge and experience of participants, mean values indicate varying levels of agreement or usage of AI across different specialties. Endodontics has the highest mean score (4.23 ± 0.72), suggesting that participants in this specialty are more inclined to agree with or apply AI in their practice compared to others. Oral Medicine follows with a mean of 3.98 ± 1.35, indicating a similarly high level of engagement or positive perception of AI. On the other hand, specialties like Oral Radiology (mean 3.56 ± 1.47) and Oral Pathology (mean 3.60 ± 1.46) reflect a slightly lower level of agreement or application of AI. The overall mean score across all specialties is 3.80 ± 1.24, showing a general positive outlook toward AI usage in dentistry.
The highest mean scores reflecting perceptions and attitudes of dental practitioners are observed among participants in Orthodontics (3.95 ± 1.29 out of 5), followed closely by Oral Medicine (3.94 ± 1.31) and Pedodontics (3.85 ± 1.22), suggesting that these specialties see AI as particularly valuable in their practices. Endodontists also show a relatively high mean of (3.83 ± 0.84), indicating a positive perception of AI. On the other hand, Operative Dentists provided the lowest mean rating (3.38 ± 1.39), followed by Prosthodontists (3.55 ± 1.11) and Oral Pathologists (3.50 ± 1.35). These specialties seem to perceive AI as slightly less valuable.
The mean scores are similar across all experience levels (p = 0.953 and 0.780) and prior work experiences (p= 0.218 and 0.154). Assessment of knowledge and experience of dentists practicing for less than 5 years showed a mean score of (3.78 ± 1.35), while those with 5 to 10 years of experience scored (3.81 ± 1.23), and participants with more than 10 years of experience scored (3.82 ± 1.09). The standard deviations indicate relatively similar levels of variation in responses across the groups. Perception and attitude scores show that dentists with 5-10 years of experience have the highest mean score (3.75 ± 1.2), indicating a slightly higher perception of AI's value in their practice compared to those with more than 10 years of experience (3.71 ± 1.07) and those with less than 5 years of experience (3.64 ± 1.33).
Additionally, participants' knowledge and experiences with AI in dental practice, in addition to their perceptions and attitudes, are consistent regardless of whether they work in academic institutions, government sectors, or private sectors (p= 0.967 and 0.963). Knowledge and experience mean scores for participants in academic institutes (3.78 ± 1.24), governmental sectors (3.81 ± 1.27), and private sectors (3.82 ± 1.21) are very similar, with only minor differences. Additionally, evaluations of dentists’ perceptions and attitudes revealed that participants working in academic institutions and the private sector have the same mean score (3.71 ± 1.2), while those in the governmental sector have a slightly lower mean score (3.67 ± 1.25).
On the other hand, there are statistically significant differences between participants’ knowledge and experiences in addition to perceptions and attitudes based on their region of employment (p= 0.017 and 0.008). The Western Region has the highest mean score (3.93 ± 1.3), followed closely by the Central Region (3.92 ± 1.08 and 3.78 ± 1.09). The Southern Region has a slightly lower mean of 3.79 ± 1.44 and 3.60 ± 1.35, and the Eastern Region has a mean of 3.64 ± 1.22 and 3.47 ± 1.17. The Northern Region shows the lowest mean score at 3.14 ± 1.49 and 3.09 ± 1.45, indicating a potential difference in how AI is perceived or applied across different regions.
In multivariable regression analysis, region remained a significant predictor of both knowledge and experience scores (β = –0.71, p = 0.006) in addition to perception and attitude scores (β = –0.62, p = 0.013), with dentists in the Northern region scoring lower than those in the Central region (β = –0.71, p = 0.006). Other variables, including gender, specialty, education, experience, occupation, and past employment, were not significant predictors.
4. DISCUSSION
Technological advancements have been transforming various fields, especially in the medical and dental sectors, significantly enhancing patient care. The adoption of AI in dentistry has become increasingly evident, with algorithms able to detect a wide range of oral diseases through radiographs and photographs. These AI technologies have proven to be effective and cost-efficient [12].
Awareness of AI applications is essential for dentists’ professional development as they integrate these technologies into their practices. Assessing their knowledge and attitudes toward AI provides insight into the current state of dental practices, highlighting limitations and areas for improvement. Previous studies in the Kingdom of Saudi Arabia have targeted dental students, interns, and postgraduate dentists [19]. However, there is a scarcity of studies examining dentists' awareness, attitudes, and knowledge regarding AI in Saudi Arabia, particularly with respect to factors such as age, gender, years of experience, specialty, and region. This highlights the importance of our cross-sectional study, which aims to represent all regions of the Kingdom.
The sample includes a diverse mix of relatively new professionals and those with extensive experience, with balanced representation of both genders (Male = 47.7%, Female = 52.3%). It features a highly educated group with various specialties and advanced qualifications, providing a comprehensive overview of different areas of dental practice. Most have prior experience with a few organizations, primarily in Saudi Arabia, while smaller proportions have worked in other regions. Participants come from a broad range of employment settings, with strong representation from academia (34.9%), the public sector (33.4%), and the private sector (31.2%). While the distribution differed from the national workforce proportions (68% in private vs 32% in public sectors), the distribution in the current study strengthened the diversity and provided more balanced comparisons across institutional context [20].
While the majority of individuals (66.9%) possess some familiarity with AI, a significant proportion would benefit from further education or training to enhance their understanding and application of AI in clinical practice, as indicated by a mean score of 3.86 ± 1.37. Awareness of the basic principles of AI, however, varies across studies. For example, 82.5% of dentists in India reported a good understanding of AI [21], whereas only 42.5% of dentists in the United Arab Emirates (UAE) expressed knowledge of AI basics [13]. In contrast, a survey of dental students in Riyadh, Saudi Arabia, found that 50.1% had no knowledge of basic AI principles [14]. Consistent with previously reported literature [13, 15], self-directed learning was the predominant method for acquiring AI knowledge in our study (38.4%), with formal education and professional experience serving as supplementary sources (31.2%).
Although most participants utilize AI in some capacity (55.7%), its regular and widespread implementation in dental practice remains limited (5.6%), highlighting opportunities for greater integration within the field. According to our results, AI is applied across various tasks, with its greatest potential identified in research (15.9%), diagnosis (14.7%), and treatment planning (11.7%). Older age groups (51-60, >60) reported higher utilization of AI compared to younger dentists (<30). This may be attributed to their longer clinical experience and exposure to evolving technologies, which give them the confidence to adopt and integrate AI into their practice. Furthermore, data suggests that cost (31.5%), training (30.9%), in addition to skepticism (10.4%) and concerns about the security and privacy of patient data (25.1%), remain significant barriers to AI adoption in dental practices. Federated learning, which employs privacy-preserving techniques such as secure multi-party computation and differential privacy models, can help mitigate these concerns [22].
Both male and female participants demonstrated similar levels of understanding, approaches, and experiences regarding AI in dentistry. AI was perceived as most valuable in areas such as treatment planning, particularly in smile design and implant placement (No.1 ranking of importance and mean score of 3.95 ± 1.34), as well as in caries detection and diagnosis (No.2 ranking of importance and mean score of 3.88 ± 1.35). Similarly, 85% of dentists working in the UAE agreed that AI can be effectively utilized in the detection of caries and fractures [13]. Dentists in Brazil exhibited similar trends between genders in their views on AI applications in dentistry, except for the belief that AI will revolutionize the field, where female dentists expressed greater agreement [15].
Participants expressed a strong eagerness to learn about and incorporate AI into their practice (mean = 3.86 ± 1.37), indicating significant interest among dental professionals in adopting AI technology. Similarly, 81.2% of dentists in India [21] and 82.1% of dentists in the UAE [13] have expressed willingness to integrate AI into their practices. Despite this enthusiasm, our results show that the belief in AI playing a crucial role in dental practice received a relatively low mean score (3.67 ± 1.29), ranking 9th in importance. This skepticism may stem from participants' caution about AI's potential to surpass human intelligence or from concerns about its overreliance on AI for diagnosis, treatment planning, and prognosis. Surlari et al. argue that AI could never fully replace clinicians but emphasize its importance in areas ranging from prevention to treatment and diagnostics [7].
Interestingly, participants felt that AI should be more heavily integrated into postgraduate training than undergraduate education, with importance rankings of 2 and 7 and mean scores of 3.84 ± 1.35 and 3.70 ± 1.35, respectively. This underscores the perceived need for formal AI education at more advanced levels of professional training. Similar perceptions were reported among dental students in Riyadh, Saudi Arabia, and dentists in the UAE, with 82.2% and 76.1% agreeing that AI should be prioritized in postgraduate training over undergraduate education, respectively [13, 14].
Our results indicate that age does not have a significant impact on knowledge, perception, or application of AI in dental practices (p-values of 0.65 and 0.25). The length of time participants have been practicing dentistry (p = 0.95 and 0.8), their prior experiences (p = 0.22, 0.15), their educational level (p = 0.74 and 0.2), and their specialty (p = 0.94 and 0.83) do not significantly influence their views on the use of AI in dental practice. Similar trends were observed in South Korea, where perceptions and attitudes toward AI were consistent among dental students and dentists at varying levels of experience, regardless of gender, age, or region of residence [16]. Participants expressed a strong need for AI training and demonstrated eagerness to expand their knowledge on the subject. They generally viewed AI as a supplementary tool to aid in diagnosis and treatment decisions, rather than as a replacement for clinical judgment and expertise. This indicates that AI readiness relies more on the availability of a solid infrastructure than on individual attributes, which is in line with health informatics analysis that links AI literacy more to organizational policies than clinician demographics [4, 11].
Awareness and application of AI in dental practice significantly differed based on region (p = 0.02 and 0.008). These associations remained significant in multivariable regression models, confirming that regional effects persisted even after adjustment for other participant characteristics. Our findings contrast with a study targeting both dentists and dental students from 22 cities in Saudi Arabia that found no significant regional differences in participants' perceptions and utilization of AI [17]. Dental students were reported to account for 49.2% of participants, and the absence of practical clinical experience in this group may have contributed to the lack of significant regional differences. More importantly, the adoption of a convenience sampling technique, as opposed to the proportionate stratified sampling method used in the present study, has resulted in a skewed regional representation, with 66.1% of participants from the Western region and only 6.7% from the heavily populated Central region. Consequently, it is challenging to gauge regional differences with great precision.
Regional variations reported in the present study may be attributed to factors such as differing levels of exposure to emerging technologies, access to advanced training programs, and the availability of AI-related infrastructure- factors also highlighted in a multi-national multi-center study targeting both developed and developing countries [23]. For example, the Central and Western regions host a greater number of major universities offering graduate and postgraduate dental programs, in addition to specialized clinics and research centers, compared to other regions. As a result, AI technologies have been actively and extensively integrated and utilized in education, clinical care, and research. The exposure to various AI tools and hands-on experiences through educational and research institutions has likely raised awareness of their importance in providing state-of-the-art dental services.
A qualitative assessment of the reported regional differences would be greatly beneficial in examining this matter in greater depth. This will guide region-tailored approaches to AI education, and implementation is important, including integrating AI literacy into undergraduate and postgraduate curricula, CPD courses, and targeted research grants. This will provide dental professionals across all regions with the necessary knowledge and tools to effectively integrate AI into their practices.
5. LIMITATIONS AND RECOMMENDATIONS
The cross-sectional nature of the study did not allow for cause-and-effect relationships to be identified. Future work should include quantitative and qualitative longitudinal designs that follow dentists over time to assess AI awareness and adoption. Future studies could use qualitative interviews with dentists practicing in regions that demonstrated lower AI knowledge and utilization to explore region-specific barriers, such as access to training, institutional support, and availability of AI-related infrastructure. Additionally, qualitative case studies of dental clinics that have successfully implemented AI tools could provide practical insights into real-world integration processes.
Additionally, self-reported questionnaires are susceptible to recall and social desirability bias. This can, for example, overestimate awareness and underestimate reported challenges. Because invitations could not be individually tracked, the overall response rate could not be calculated, and the extent to which the sample proportions reflect the true distribution of the national dentist population cannot be guaranteed. This should be considered when generalizing the findings. However, dissemination through multiple academic institutions, professional networks, and national dental groups across all five regions of Saudi Arabia helped mitigate this limitation by broadening reach across diverse practice settings and geographic areas, thereby reducing the likelihood of systematic regional or institutional sampling bias.
The instrument presented great internal reliability with a 0.966 Cronbach's alpha for the total items of the questionnaire. This can also indicate partial overlap among closely related items, particularly within the attitudes and perceptions domain. Further studies should consider factor-analytic validation to further refine domain structure and reduce potential redundancy. Although multivariable models were applied to adjust for confounders, residual confounding cannot be fully excluded.
CONCLUSION
Within the limitations of this study, dentists' knowledge, application, perceptions, and attitudes toward AI in Saudi Arabia were generally consistent across factors such as age, gender, education level, specialty, occupation, and experience. However, significant regional differences were observed. Dentists in the central and western regions demonstrated higher levels of knowledge and experience with AI, while those in the northern region were less enthusiastic about its role in dental practice. Accordingly, these findings highlight the need for targeted educational efforts in regions with lower levels of awareness and utilization. Overall, dentists showed a generally positive outlook toward AI integration, particularly in diagnostics, treatment planning, and education, as reflected in the perceptions and attitudes.
AUTHOR’S CONTRIBUTION
The author confirms sole responsibility for the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
ABBREVIATION
| CPD | = Continuing Professional Development |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the IRB of Princess Nourah bint Abdulrahman University, Saudi Arabia (IRB Log Number: 24-0686 on 22 April 2024).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R490), Riyadh, Saudi Arabia.
ACKNOWLEDGEMENTS
The author would like to acknowledge the kind support received from Dr. Hadeel Basuhail, Dr. Jori Alahmadi, Dr. Rahaf Bin Salamah, and Dr. Obai Aldossary

