All published articles of this journal are available on ScienceDirect.

Buccal Space Collection of Ozonized Sunflower Oil Following Off-Label Injection: A Case Report
Authors Info & Affiliations
Abstract
Introduction
Ozonized sunflower oil is increasingly employed in the management of oral conditions due to its antimicrobial and immunostimulating properties. While topical use is generally considered safe, off-label applications, such as intrasulcular or periapical injections, may pose unexpected clinical risks. The aim of the present report was to describe an unusual complication due to an improper use of ozonated oil and its management.
Case Description
We, herein, report the case of a 67-year-old female presenting with facial swelling unresponsive to antibiotics and corticosteroids. Initial evaluation suggested an odontogenic abscess; however, ultrasonography revealed an irregular, avascular intramuscular collection with a surrounding hypoechoic halo. The patient disclosed prior treatment involving ozonized sunflower oil, raising suspicion of an inadvertent submucosal injection. Surgical drainage yielded brownish fluid, with microbiological analysis proving negative. A second aspiration was required due to residual swelling. The patient reported near-complete symptom resolution following the second intervention. This case highlighted the potential adverse outcomes of non-topical administration of ozonized oil, which is non-resorbable and may induce a foreign body inflammatory response. Ultrasonography played a key role in differential diagnosis and guided therapeutic intervention, which was successfully managed with needle aspiration.
Conclusion
Off-label injections of ozonized oil should be avoided. Ultrasound assessment is instrumental in diagnosis, and needle-driven aspiration may offer an effective, minimally invasive treatment.
1. INTRODUCTION
Ozone (O3) is a triatomic allotrope of oxygen naturally present in the Earth’s stratosphere, where it plays a critical role in shielding the planet from ultraviolet radiation. In medical applications, ozone is generated by passing pure oxygen through an electrical discharge, a process that produces a mixture of ozone and oxygen in various concentrations. Although ozone is highly reactive and thus challenging to store and stabilize, its potent biological properties have attracted increasing interest in the biomedical field [1, 2].
Medically, ozone exhibits a broad spectrum of activity, including antimicrobial, antiviral, antifungal, and immunomodulatory effects. These effects are primarily attributed to its ability to generate reactive oxygen species (ROS) and lipid oxidation products, which can disrupt microbial membranes and stimulate host immune responses [3-5]. Ozone therapy is considered a form of oxidative preconditioning, inducing mild oxidative stress that activates endogenous antioxidant pathways and modulates inflammatory processes [6, 7]. At controlled doses, this mechanism is exploited to promote wound healing, modulate local immune responses, and reduce microbial burden in infected tissues. However, the use of ozone is not without potential adverse effects. According to the World Federation of Ozone Therapy’s Review on Evidence-Based Ozone Therapy, a safe concentration of 5–10 µg/mL is recommended for intralesional injections or irrigation procedures in order to minimize the risk of toxicity. Prolonged or excessive exposure to gaseous ozone may result in systemic symptoms, such as nausea, headache, and irritation of the upper respiratory tract [8-10].
In the dental field, ozone has gained recognition as an adjunctive treatment modality across a range of specialties. It has been used in the management of dental caries, endodontic disinfection, periodontal disease, alveolar osteitis, and mucosal lesions, such as recurrent aphthous stomatitis and oral lichen planus [11-14]. Its versatility is enhanced by the ability to deliver it in various forms, including ozone gas, ozonated water, and ozonized oils, allowing tailored application based on the clinical condition. Ozone therapy is also being explored as a complementary treatment for premalignant and malignant oral lesions due to its potential antimicrobial, anti-inflammatory, and immune-modulating properties, although scientific evidence on its effectiveness remains limited [15].
Ozonized oils, typically derived from sunflower or olive oil, are produced by reacting ozone with unsaturated fatty acids, forming stable ozonides. These compounds preserve the antimicrobial and anti-inflammatory properties of ozone while enabling safer and more controlled topical application [16, 17]. Ozonized sunflower oil, in particular, has emerged as a popular vehicle due to its higher linoleic acid content, offering a greater number of reactive sites for ozone binding, and demonstrating comparable germicidal effects to ozonized olive oil [18]. In periodontal therapy, the topical application of ozonized oil has been associated with reductions in clinical indices of inflammation and enhanced post-surgical healing. However, studies have also reported adverse outcomes, such as increased dentinal hypersensitivity, when ozonized oils have been introduced into periodontal pockets in certain contexts [19-22].
Despite the increasing adoption of ozonized oil in dental practice, its safety profile is well-established primarily for topical application. There is a paucity of data regarding its behavior when administered via off-label routes, particularly intratissue injection [23]. Ozonized oils are not water-soluble and, unlike gaseous ozone or ozonated water, are not readily metabolized or resorbed by host tissues. Consequently, inadvertent injection into the soft tissues or submucosal planes may result in foreign body-type granulomatous reactions, chronic inflammation, or persistent localized swelling due to the accumulation of non-resorbable material. In this context, herbal treatments, such as aloe vera, turmeric, and green tea extracts, may offer antimicrobial and anti-inflammatory effects and may serve as safer alternatives to ozonized oil in managing localized oral lesions. Their biocompatibility and ability to support oral homeostasis make them promising options, though further clinical validation is needed [24].
This report presents a rare and previously undocumented complication arising from the off-label submucosal injection of ozonized sunflower oil, resulting in an intramuscular collection in the buccal space. The case underscores the diagnostic challenges posed by such presentations, which may mimic odontogenic infections, and emphasizes the role of imaging, particularly ultrasound, in guiding diagnosis and management. Moreover, it highlights the importance of recognizing the limitations of off-label therapeutic interventions with biologically active compounds, such as ozonized oils, which, despite their biocompatibility, may induce unintended tissue responses when used beyond approved indications.
2. CASE DESCRIPTION
A 67-year-old female patient with no significant medical history presented to the Maxillofacial and Stomatology Clinic at Trieste University Hospital, reporting swelling and pain on the left side of her face that began 14 days earlier (Fig. 1). The symptoms followed an unspecified treatment by her dentist, involving the topical application of an unknown substance around the upper left first molar. Subsequently, she underwent antibiotic (amoxicillin and clavulanic acid 1 gram three times a day for 2 weeks) and corticosteroid therapies, with no improvement in signs and symptoms. Extra-orally, the left middle-third region of the face resulted in swelling and presented a parenchymatous consistency, tenderness, and pain upon superficial palpation. On the intra-oral examination, the first superior left molar showed a 5 mm gingival recession on the palatal root, together with purulent drainage on gentle sulcular probing. Furthermore, no alteration in saliva quality and quantity from the Stensen duct was noted.

Extraoral image of the patient showing swelling and edema in the left cheek region.
With the patient’s consent, X-rays were performed. Orthopanoramic images showed no macroscopic alteration of the bony structures, whereas an intraoral radiograph revealed a radiolucent apical lesion on tooth 2.6, suggesting a possible diagnosis of odontogenic abscess (Fig. 2). Therefore, a new antibiotic therapy (clindamycin 900 mg a day for 6 days) was prescribed, and an echography was scheduled for a more detailed evaluation of the swelling. The patient was re-evaluated three days later, showing no signs of improvement. The ultrasound showed a profound alteration in the intramuscular portion of the left cheek (buccal space), with a 3x2 cm central inhomogeneous portion with irregular and blurred edges. This central area was surrounded by a hyperechoic halo, suggesting a granulomatous reaction (Fig. 3). After further investigating the medical history and conducting an additional interview with the patient, it was found out that she had previously undergone a treatment with ozonized sunflower oil (Ozosan Gel, Bioactiva, Vicenza, Italy) used locally, after the use of anesthesia. Thus, the possibility of an off-label periapical injection of ozonized oil was considered. Only an injection administered coronal to the upper insertion of the buccinator muscle could explain the accumulation in the cheek.
In agreement with the patient, a surgical drainage was performed. After outlining the area of the collection with a dermographic pencil (Fig. 4), a small incision (3 mm) was made in the mucosa anterior to the Stensen duct, and an 18-gauge needle was inserted. Compression of the cheek released a brownish liquid, which was aspirated (Fig. 5) and sent for microbiological analysis. Single interrupted resorbable stitches were applied [25]. Ten days later, due to the persistence of mild swelling, a second drainage was performed.

Pre-operative periapical radiograph revealing a radiolucent apical lesion on tooth 2.6, suggesting a possible diagnosis of odontogenic abscess.
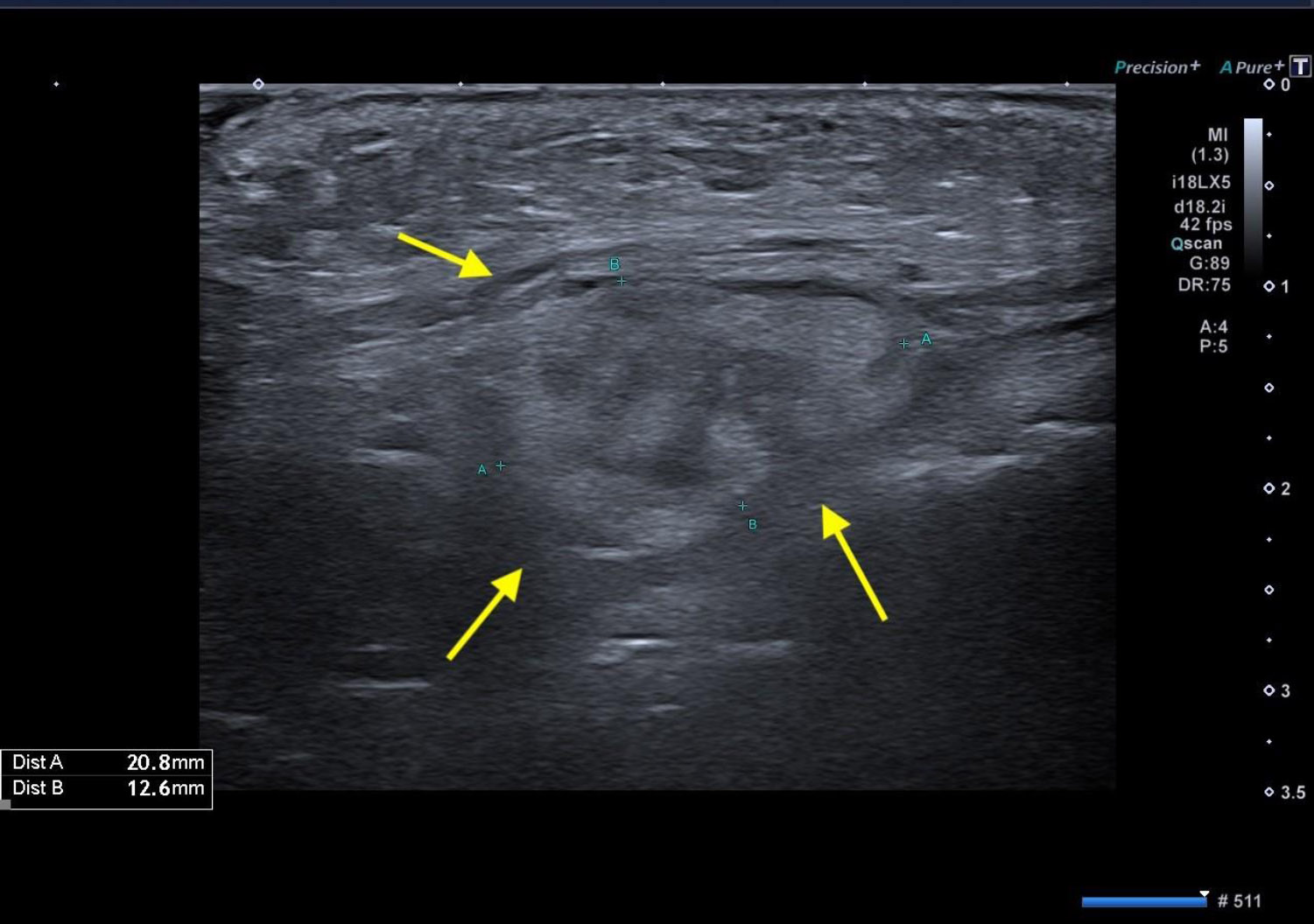
Initial echography. The presence of a 3x2 cm central inhomogeneous portion with irregular and blurred edges, surrounded by a hyperechoic halo (yellow arrows), suggesting a granulomatous lesion.

The area of the collection was identified through palpation of the cheek and carefully marked using a dermographic pencil for precise localization.
During a 4-day check, the patient reported an almost complete resolution of symptoms, with no signs of inflammation or bleeding visible. A follow-up ultrasound was scheduled, and it revealed two anechoic areas (3 mm in diameter) and a blurred hyperechoic region in the subcutaneous and muscular areas, with no clear boundaries (Fig. 6). Microbiological analysis resulted in negative findings, and facial asymmetry was no longer visible.
Two weeks later, the patient underwent the extraction of tooth 2.6. One month later, no symptoms were evident.
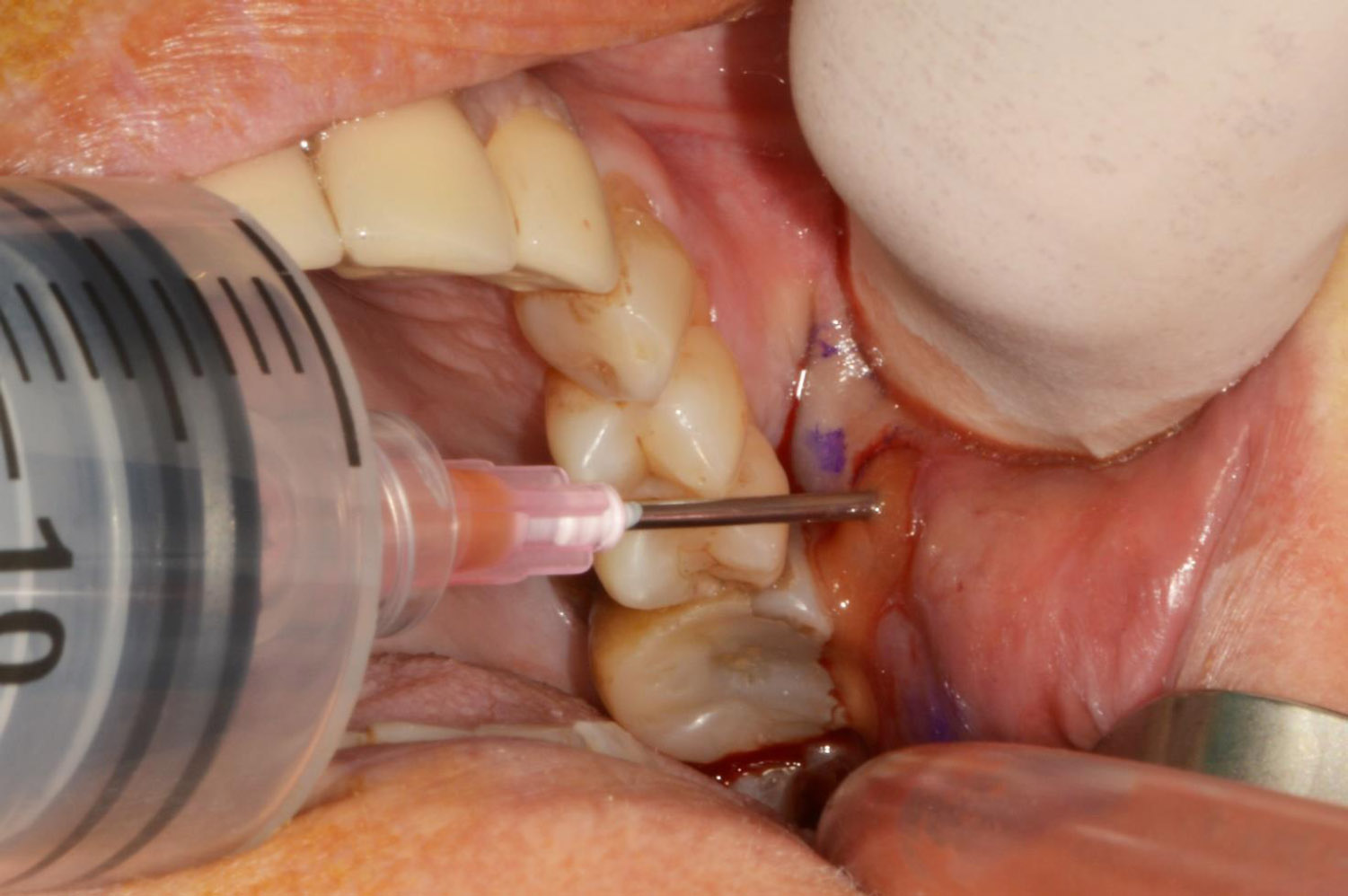
Surgical drainage. Manual compression of the cheek resulted in the release of a brownish fluid, which was aspirated for analysis.
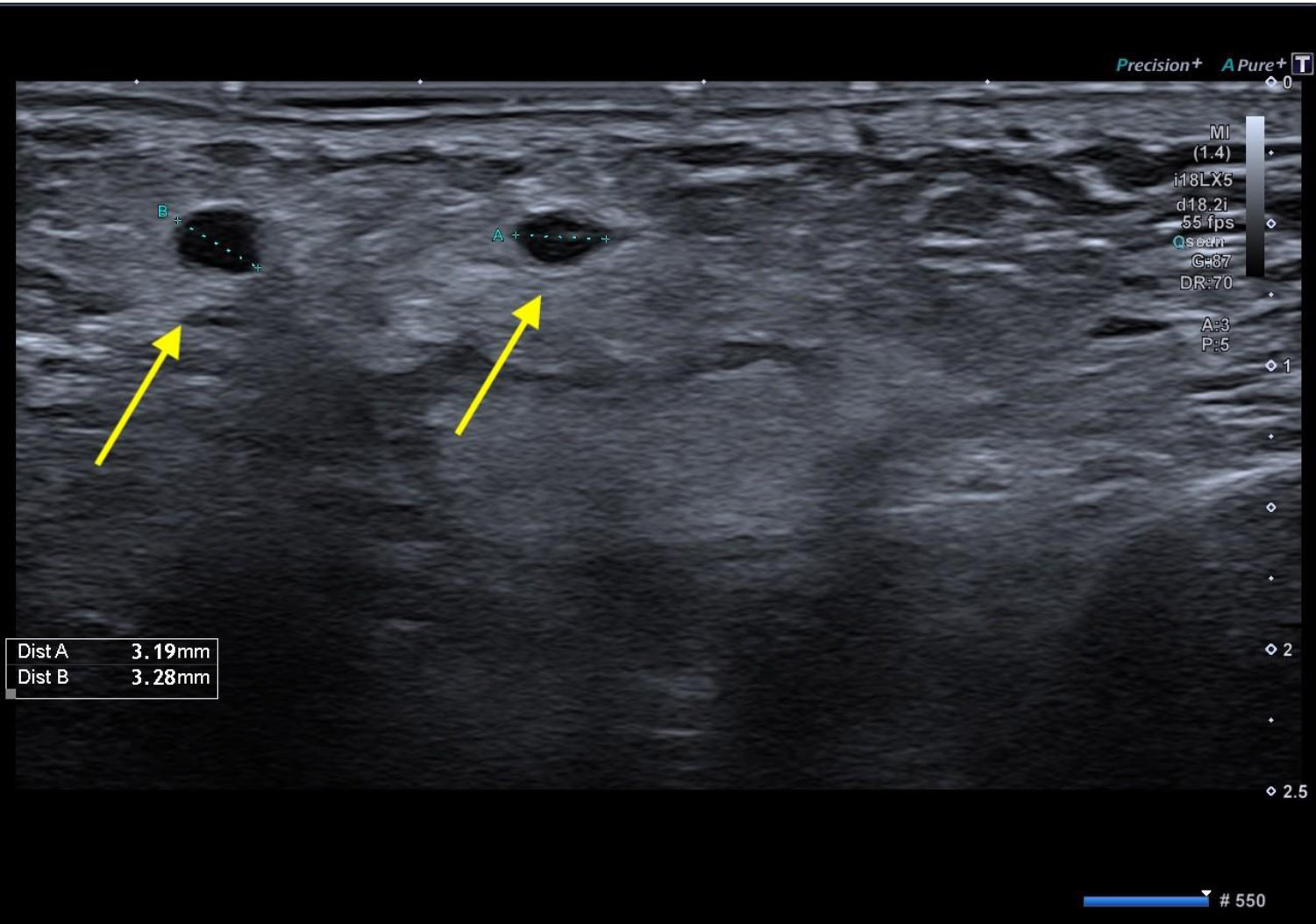
Post-operative ultrasonography. Two small anechoic areas of approximately 3 mm in diameter were identified (yellow arrows), along with a poorly defined hyperechoic region within the subcutaneous and muscular tissues, lacking clear demarcation.
3. DISCUSSION
This case has illustrated an uncommon, but clinically significant complication associated with the off-label use of ozonized sunflower oil. While ozone has become increasingly popular in dentistry for its antimicrobial, anti-inflammatory, and tissue-regenerative effects [18], the therapeutic safety of its various formulations, particularly ozonized oils, depends heavily on the mode of administration [26-28]. As seen in this report, deviation from topical application, such as inadvertent or unintentional injection into soft tissue compartments, may provoke a foreign body reaction and chronic inflammation [29, 30].
The diagnostic challenge presented by this case lies in the clinical similarity between a foreign body granuloma and an odontogenic abscess. The patient’s history of persistent facial swelling, coupled with lack of response to antibiotics and corticosteroids, initially pointed toward a resistant infection. Only after a more thorough anamnesis and imaging evaluation was the suspicion raised of a non-infectious inflammatory collection caused by ozonized oil. Given that ozonized sunflower oil is lipophilic and non-resorbable, it can persist in soft tissues and trigger localized immune responses, especially when injected unintentionally into deeper planes.
Ultrasonography played a central role in the differential diagnosis. The imaging revealed an irregular, avascular intramuscular collection with blurred margins and a surrounding hyperechoic halo, indicative of a granulomatous lesion. This is consistent with previously published findings in the field of cosmetic dermatology, where ultrasonography has been used to characterize complications from dermal fillers, especially non-resorbable materials [31]. The present case has provided support to the growing value of ultrasound in oral and maxillofacial diagnostics, not only for its non-invasive nature, but also for its ability to differentiate fluid collections, foreign materials, and abscesses with a high degree of accuracy [32].
The treatment strategy emphasized a minimally invasive approach. While traditional open surgical drainage was considered, a less traumatic needle aspiration was preferred to reduce morbidity. Although this initially achieved only partial resolution, a second aspiration proved effective. This has been found to align with best practices in managing similar filler-related lesions, where conservative management often precedes excisional intervention. The use of ultrasound-guided aspiration, although not performed in this case, has been well-documented in the context of oral cavity lesions [33], and could represent a valuable improvement, particularly in complex or recurrent presentations.
This case has also mirrored patterns observed in aesthetic medicine, where adverse tissue responses are frequently caused by the persistence of injected materials, such as silicone or even hyaluronic acid. A recent systematic review documented that over 87% of adverse reactions to injectable fillers occur due to foreign body responses [29], and more than half of the cases are associated with unapproved or impure materials, such as liquid silicone [30]. Although ozonized oils have not been mentioned in these studies, the pathophysiological mechanisms appear similar, suggesting that any non-resorbable injectable substance can behave unpredictably when misplaced in soft tissues.
Furthermore, the importance of accurate clinical documentation and patient communication cannot be overstated. In this case, the lack of clarity surrounding the initial treatment and the absence of procedural details complicated the diagnostic process. This underlines the ethical and medico-legal implications of using alternative or off-label substances without sufficient documentation.
In summary, while ozonized sunflower oil remains a promising adjunctive therapy in dentistry, its safe use is contingent upon the appropriate route of administration. Misapplication, particularly through injection into non-target tissues, can result in unexpected and potentially protracted complications. Clinicians should be vigilant about the physical properties of therapeutic agents, especially those not designed for parenteral use. When complications arise, imaging modalities, such as ultrasonography, can be invaluable for diagnosis, treatment planning, and monitoring. This case reinforces the necessity of adhering to evidence-based protocols and raises awareness of a rare but relevant clinical scenario.
CONCLUSION
To date, no local adverse effects have been reported in the literature regarding the topical use of ozonized oil in dentistry. However, this case has demonstrated that off-label applications, particularly intratissue injections, may lead to significant complications due to the non-resorbable nature of the oil and its potential to elicit a foreign body inflammatory response. When such events occur, minimally invasive management through needle aspiration can offer a safe and effective therapeutic option. Moreover, ultrasonography has proven to be an essential diagnostic tool, enabling accurate differentiation from odontogenic infections and guiding appropriate treatment.
This case report has presented certain limitations that must be acknowledged. The lack of accurate documentation of the initial treatment required retrospective reconstruction of the patient’s history, which may have introduced potential recall bias. Diagnosis relied solely on clinical and ultrasound findings, without histopathological confirmation to definitively characterize the lesion. Additionally, the aspiration procedure was conducted without real-time ultrasound guidance, which may have limited its precision and effectiveness. Furthermore, the limited follow-up did not allow for the assessment of possible long-term complications.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: F.B., C.S.: Study conception and design; M.Z.: Data collection; R.D.L.: Analysis and interpretation of results; A.R., F.B.: Drafting of the manuscript. All authors have reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| O3 | = Ozone |
| ROS | = Reactive Oxygen Species |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
CONFLICT OF INTEREST
Dr. Claudio Stacchi is the Editorial Advisory Board member of the Open Dentistry Journal.
ACKNOWLEDGEMENTS
Declared none.

