All published articles of this journal are available on ScienceDirect.

Conventional vs. Digital Impressions: Preferences and Comfort Level among Prosthodontic Patients
Authors Info & Affiliations
Abstract
Introduction
Digital impression techniques have gained popularity due to enhanced patient comfort and workflow efficiency. However, conventional methods remain common in many Saudi institutions. This study aimed to compare patient-reported comfort and preference between digital and conventional impressions in prosthodontic treatment in Almadinah Almunawarah, Saudi Arabia.
Methods
A retrospective, within-subject study was conducted on 100 prosthodontic patients who experienced both digital and conventional impressions. A validated 14-item self-administered questionnaire was used to assess comfort and preference. Descriptive statistics, paired t-tests, and ANOVA were performed using SPSS Version 26 (p < 0.05).
Results
Digital impressions were significantly more comfortable than conventional impressions across multiple domains, including gag reflex, breathing difficulty, and time perception (p < 0.001). Overall, 84% of patients preferred digital impressions. Gender, age, and arch location had no significant influence on preference.
Discussion
Digital impression was the preferred impression technique among patients who received prosthodontic treatments, due to a more comfortable and pleasant experience, compared to conventional impression making procedure.
Conclusion
Investing in digital impression and digital workflow is highly recommended to improve patients' experience during prosthodontic procedures.
1. INTRODUCTION
It is crucial that the oral structures are replicated with high precision, for a prosthetic rehabilitation to be both functional and aesthetically pleasing. Consequently, the impression-taking process is one of the most vital steps in achieving successful restorations [1]. Each stage of the procedure introduces the possibility of human and/or material errors [2]. Conventional impressions, while long considered the gold standard, often require multiple appointments and may lead to procedural inefficiencies. In contrast, digital technologies are now increasingly integrated into clinical dentistry, leading to greater clinical success through enhanced efficiency, accuracy, and patient-centered care [2, 3].
IOS streamlines the process by eliminating the need for tray selection, dispensing, and setting of impression materials, disinfection, and shipping impressions to the laboratory [4]. At the outset, digital scanners were bulky and costly, restricting their availability to a select few innovative dental practices [5]. Nevertheless, with technological advancements and the emergence of smaller, more cost-effective scanners, digital impression systems have gained widespread adoption in dental offices globally [5]. From the patient's viewpoint, conventional impressions are frequently associated with discomfort, gagging, and anxiety, reducing patient acceptance [6]. Research indicates that digital impressions often result in increased patient satisfaction due to the elimination of uncomfortable traditional impression materials [7]. Patients frequently perceive the process of obtaining digital impressions as faster and more convenient, leading to a generally positive experience [6, 7].
Digital workflows encompass not only intraoral scanning but also digital treatment planning, design, and guided implementation. For instance, fully digital workflows have been used successfully for implant placement and crown fabrication with high patient and clinician satisfaction [8]. Such workflows integrate CAD/CAM technologies with cone-beam computed tomography (CBCT) data and virtual design software to improve accuracy and efficiency [7, 9].
Due to restricted access and adoption, many Saudi Arabian healthcare facilities still use traditional methods, even in the face of growing interest in digital impression systems using intraoral scanners (IOS) [7, 9]. The majority of the supporting data for digital impressions comes from international studies, despite the fact that they clearly improve patient comfort and workflow efficiency. Particularly in prosthodontic settings, there is a lack of localized research evaluating patients' perceptions toward digital versus traditional techniques. For Saudi dental practices, this gap must be filled in order to successfully integrate digital technology into everyday dental practice. Thus, the aim of this study was to evaluate and compare patient preferences, acceptance, and satisfaction with traditional and digital impression techniques in patients with prosthodontic treatment. The null hypothesis stated that there is no discernible difference between the two approaches in terms of patient comfort or preference.
2. METHODS
2.1. Study Design
This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [10]. It is a retrospective within subject observational study, in which subjects who were exposed to both impression methods (i.e. digital and conventional) were recruited. Then, they received a questionnaire to compare their preferences, acceptance, and level of satisfaction with both techniques. The data was collected during the period between June and August 2024.
2.2. Study Subjects
Inclusion criteria included Saudi and non-Saudi adult patients requiring single or multiple crowns and/or bridges in the anterior and/or posterior regions who underwent both digital and conventional impression techniques from both centers. Subjects' age range was from 18 to 65 years old. The study was conducted between June and August 2024. Patients who showed up to the follow-up visit within a week after the impression appointment were considered in the study. Patients who did not experience both impression techniques and those who did not agree to consent were excluded from the study.
2.3. Sample Collection and Study Tool
A total of 100 subjects (45 males and 55 females) were recruited from restorative/prosthodontic clinics at 2 centers; Prince Sultan Military Hospital and Prince Mohammed bin Abdulaziz Hospital in Madinah, KSA. For the traditional impression technique, impressions were taken in a one-step process using polyvinyl siloxane (PVS) and alginate material. Full-arch impressions, including the upper arch with the palate and aligned arches, were captured with the use of retraction cords with an equigingival finish line before the impression was taken. For the digital impression technique, intra-oral scans were performed as a full-arch scan using a standardized scan strategy without the use of retractors. The scan was completed in one step. Traditional impressions and digital scans were taken on separate days, with traditional impressions being taken first. The patients included in the study completed their treatment based on the digital impression techniques taken. Before participating, subjects provided their informed consent, and the study was carried out in compliance with the 2013 revision of the Declaration of Helsinki.
A previously validated questionnaire [11], with some modifications, was utilized. The questionnaire was anonymous and self-administered, electronically sent to the subjects during the follow-up appointments. It evaluated patients’ perception after being subjected to conventional impressions using multiple materials and the digital impression using the 3Shape system (TRIOS 3, 2017, Denmark) with a scanner and CEREC Omnicam scanner (Densplay Sirona, USA). The questionnaire was divided into four main sections: The first gathered demographic information (age, gender, nationality, education, and employment) about the patients. The second section focused on patient comfort during treatment with the conventional impression technique, which was further divided to assess their experience with both lower and upper jaw impressions. The third section focused on patient comfort during treatment with the digital impression technique and was further divided to assess their experience with both lower and upper jaw impressions. Finally, the fourth section explored patient preference for the impression technique used and assessed patient acceptance of the time taken for each impression technique.
The questionnaire was administered in Arabic and reviewed for content validity by a panel of bilingual dental professionals to ensure linguistic accuracy and conceptual equivalence.
These questions also utilized a 3-point Likert scale (1 = strongly agree, 2= Neutral, 3 = strongly disagree). Based on a Likert scale of 3 points, the weighted mean was calculated, and the level of agreement was determined as described in Table 1. A 3-point Likert scale was chosen to reduce response fatigue and ensure clarity across diverse educational backgrounds.
| Weighted Mean Range | Level |
|---|---|
| 1.00 – 1.66 | Disagree |
| 1.67 – 2.33 | I don't know (Neutral) |
| 2.34 – 3.00 | Agree |
The questionnaire was distributed among study participants through the patients’ mobile numbers or email addresses provided by the patients. The received subjects’ responses were anonymous. Patients in this study were subjected to both techniques because the CAD-CAM was recently introduced to the centers, and conventional impressions were taken as backup records. Therefore, no potential bias was detected.
2.4. Statistical Analyses
Data were transferred to IBM SPSS Statistics (ver 28). Cronbach’s Alpha test was applied on a pilot sample (n=10) to check for the reliability and internal consistency of the study variables before proceeding with the study. After ensuring acceptable reliability scores, the study was conducted, and the rest of the analysis process was continued. Descriptive statistics were used to identify demographic characteristics of study participants (the center, age, gender, education level, and employment status). Likert scale and testing for significance were done using t-test and One way ANOVA, at 5% significance level. Based on a Likert scale of three points, the weighted mean was calculated, and the level of agreement was determined as described in Table 1.
2.5. Sample Size Justification
Sample size estimation was based on an a priori power analysis assuming a medium effect size (Cohen’s d = 0.5), α = 0.05, and power (1 – β) = 0.9. According to standard calculations, a minimum of 86 participants was required (Cohen, 1988). With a final sample of 100, the statistical power achieved was approximately 90.3%, ensuring robust analysis.
3. RESULTS
The obtained values from the Cronbach’s Alpha test were 0.859 and 0.886 for the conventional and digital impression sections, respectively. This indicates that very good reliability was achieved for the 14 items included in the questionnaire. The questionnaire was then sent to 150 subjects who fulfilled the inclusion criteria from both centers. The response rate was 67% as 100 subjects participated in the study and completed the questionnaire.
Demographic characteristics of our sample are summarized in Table 2. Similar distribution was observed among different age groups, with more participants within the age group 46 and older (22%). Regarding gender, 55% were females and 45% were males. Majority of participants were Saudi citizens (94%), while only 6% were from other nationalities. Most of our samples were married (72%), then single (23%). More than half of our participants (56%) were with an education level of a bachelor’s degree or above. while those with post-secondary and high-school and below were 16% and 28%, respectively.
| Variable | Category | N (%) |
|---|---|---|
| Age | 18-25 | 16% |
| 26-30 | 13% | |
| 31-35 | 17% | |
| 36-40 | 18% | |
| 41-45 | 14% | |
| 46 and above | 22% | |
| Gender | Male | 45% |
| Female | 55% | |
| Nationality | Saudi | 94% |
| Non-saudi | 6% | |
| Marital status | Single | 23% |
| Married | 72% | |
| Divorced | 1% | |
| Widow | 4% | |
| Education level | High school or below | 28% |
| Post-secondary (associate diploma) | 16% | |
| Bachelor and above | 56% | |
| Employment status | Employed | 50% |
| Not Employed | 50% |
The sample was equally distributed among the two centers (i.e.; Prince Sultan Military Hospital and Prince Mohammed bin Abdulaziz Hospital in Madinah, KSA). Accordingly, subjects were divided equally between 3Shape TRIOS and CEREC Omnicam intraoral scanner (IOS) systems. Most of the participants included in the study received 2-4 units (51%), then single units (37%). A small number received 8 units or more (Table 3). These units were located in anterior, posterior teeth, or both, while posterior units were observed in the majority of participants (81%).
| Variable | Category | N (%) |
|---|---|---|
| Center | Prince Sultan Military Hospital | 50% |
| Prince Mohammed bin Abdulaziz Hospital, Madinah | 50% | |
| Intra-oral scanner | 3Shape TRIOS | 50% |
| CEREC Omnicam | 50% | |
| Number of prosthetic units | single | 37% |
| 2-4 | 51% | |
| 5-7 | 7% | |
| >= 8 | 5% | |
| Location of prosthetic units | Anterior | 18% |
| Posterior | 81% | |
| Anterior and Posterior | 1% |
| Item | Impression Method | Mean | SD | Agreement Level | t-value | p-value |
|---|---|---|---|---|---|---|
| Unpleasant experience. | Conventional Impression | 2.16 | 0.78 | Neutral | 8.45 | 0.000 |
| Digital Impression | 1.33 | 0.60 | Disagree | |||
| Shortness of breath. | Conventional Impression | 1.86 | 0.75 | Neutral | 7.20 | 0.000 |
| Digital Impression | 1.21 | 0.50 | Disagree | |||
| Helplessness | Conventional Impression | 1.83 | 0.81 | Neutral | 6.50 | 0.000 |
| Digital Impression | 1.22 | 0.48 | Disagree | |||
| Overall acceptable experience | Conventional Impression | 2.25 | 0.63 | Neutral | -2.08 | 0.039 |
| Digital Impression | 2.45 | 0.73 | Agree | |||
| The appointment was perceived as non-stressful | Conventional Impression | 2.27 | 0.68 | Neutral | -2.45 | 0.015 |
| Digital Impression | 2.51 | 0.70 | Agree | |||
| Anxious about future impression procedure | Conventional Impression | 1.85 | 0.83 | Neutral | 4.05 | 0.000 |
| Digital Impression | 1.41 | 0.70 | Disagree |
| Item | Impression Method | Mean | SD | Agreement Level | t-value | p-value |
|---|---|---|---|---|---|---|
| Upper Jaw | ||||||
| Gag reflex | Conventional impression | 1.62 | 0.78 | Disagree | 4.50 | 0.000 |
| Digital impression | 1.21 | 0.48 | Disagree | |||
| Queasiness | Conventional impression | 1.66 | 0.81 | Neutral | 4.99 | 0.000 |
| Digital impression | 1.19 | 0.49 | Disagree | |||
| Breathing difficulties | Conventional impression | 1.92 | 0.81 | Neutral | 6.56 | 0.000 |
| Digital impression | 1.27 | 0.57 | Disagree | |||
| Discomfort | Conventional impression | 2.22 | 0.80 | Neutral | 9.68 | 0.000 |
| Digital impression | 1.28 | 0.55 | Disagree | |||
| Lower Jaw | ||||||
| Item | impression Method | Mean | SD | Agreement Level | t-value | p-value |
| Gag reflex | Conventional impression | 1.48 | 0.70 | Disagree | 3.91 | 0.000 |
| Digital impression | 1.16 | 0.42 | Disagree | |||
| Queasiness | Conventional impression | 1.58 | 0.74 | Disagree | 5.00 | 0.000 |
| Digital impression | 1.15 | 0.44 | Disagree | |||
| Breathing difficulties | Conventional impression | 1.93 | 0.80 | Neutral | 7.21 | 0.000 |
| Digital impression | 1.24 | 0.53 | Disagree | |||
| Discomfort | Conventional impression | 2.23 | 0.78 | Neutral | 8.27 | 0.000 |
| Digital impression | 1.40 | 0.64 | Disagree | |||
Comparison of comfort and satisfaction level items between conventional and digital impression methods is summarized in Table 4. There was a statistically significant difference was observed between the two methods for all questionnaire items. The mean agreement levels for unpleasant experience, shortness of breath, helplessness, anxiety, and stress during the appointment were 'Neutral' for the conventional impression and 'Disagree' for the digital impression.
Regarding comfort level during the impression taking procedure, most of our participants disagree with the presence of gag reflex during both impression taking methods, for the upper and lower jaws. While for queasiness, breathing difficulty, and discomfort, the majority responded as neutral for conventional and disagreed for the digital impression method, for both jaws. There was a statistically significant difference between conventional and digital impressions for all items in this section (p < 0.05) (Table 5). However, no significant difference was found between upper and lower jaws in any of the items. The majority of our sample preferred digital over conventional impression technique (84%) (Fig. 1). Table 6 summarizes subjects’ responses to impression techniques preference items.
Significant difference was found between responses from Saudi and non-Saudi participants for conventional impression only (p= 0.048). However, this should be taken with caution due to the small number of non-Saudi participants. Other factors including age, gender, marital status, education level, employment status, number and location of prosthetic units, did not show a significant difference for all items included in the questionnaires (p > 0.05).
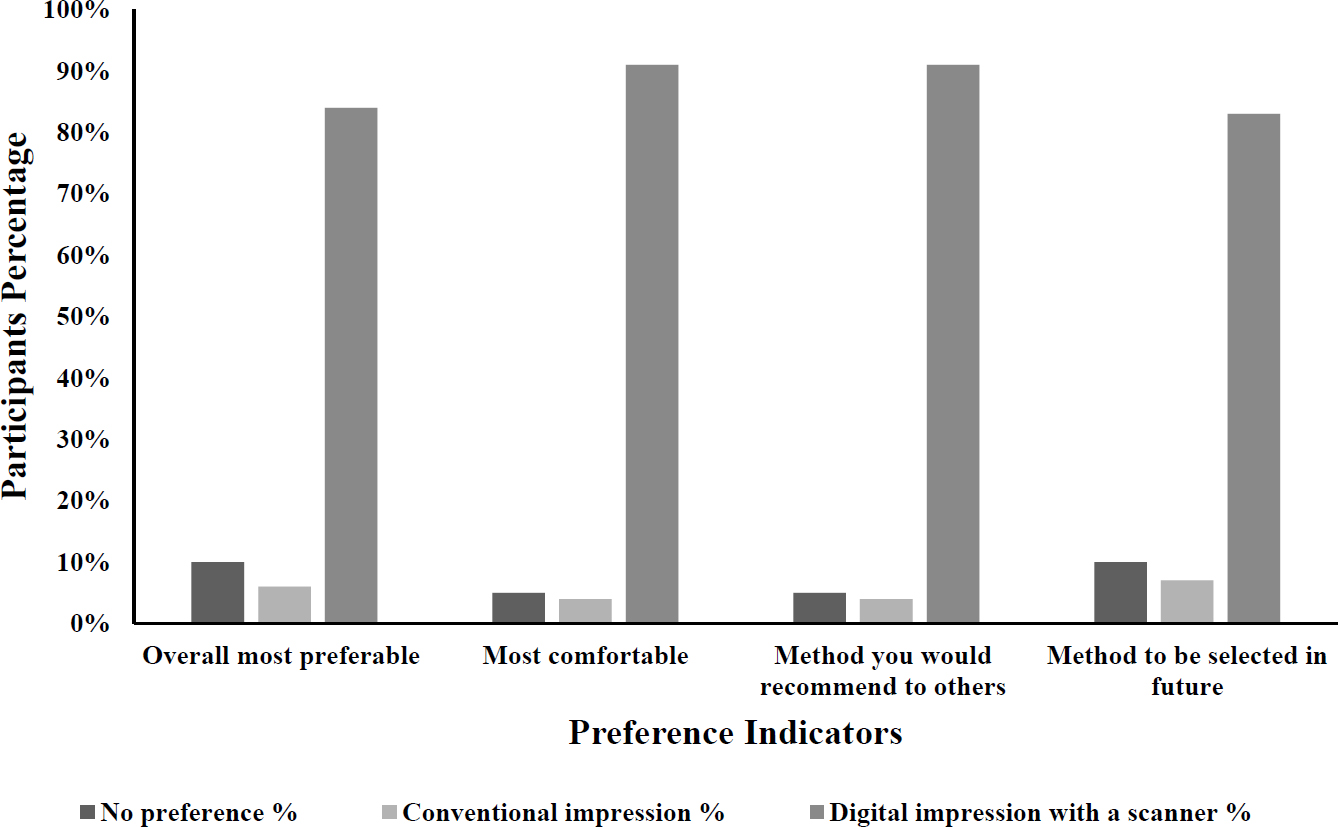
Impression techniques preference among participants.
| - | No Preference | Conventional Impression | Digital Impression |
|---|---|---|---|
| Pain/Sensitivity | 21% | 4% | 75% |
| Breathing difficulty | 9% | 3% | 88% |
| Gagging reflex | 11% | 5% | 84% |
| Appointment duration | 7% | 6% | 87% |
| Taste, smell, voice or heat | 10% | 5% | 85% |
| Size of the intraoral device (scanner/impression tray) | 20% | 10% | 70% |
4. DISCUSSION
Two different intraoral digital scanners were used in this study including 3Shape Trios scanner and CEREC Omnicam scanner. They were used with a complementary metal semiconductor (CMOS) sensor, providing a more comprehensive comparison. Over the past two decades, numerous IOS have been introduced to the market. Recent studies, however, highlight the TRIOS 3 as one of the most accurate among these systems [12]. It is widely recognized for its accuracy, particularly for capturing critical surfaces like crown preparation margins when using its High Resolution (High res) setting, as recommended by the manufacturer. Compared to the CEREC system, TRIOS 3 offers versatility in scan settings, potentially providing superior finish line detail, though at the cost of increased chair-time [12]. While CEREC scanners are also accurate and commonly used in restorative dentistry, their scanning techniques may prioritize workflow efficiency over customizable resolution settings [12]. In studies comparing complete-arch scanning, the 3Shape Trios was identified as having the best balance between speed and accuracy [13]. However, it was found that the CEREC Omnicam scanner surpassed the Trios in terms of both trueness and precision 11. The 3Shape TRIOS 3 scanner was found to stand out as the most time-efficient, completing a full scan in just 3 minutes and 8 seconds [14]. A study showed that the CEREC Omnicam system demonstrated greater accuracy in measuring occlusal contacts compared to the T-scan system, particularly in the anterior teeth region and across the entire dentition. No significant differences were observed between the two systems in the premolar and molar areas [15]. Moreover, this study showed no significant difference between the two scanners regarding patients’ preferences.
Digital impression scanners streamline the process by eliminating the need for tray selection, dispensing, and setting of impression materials, disinfection, and shipping impressions to the laboratory. Additionally, they offer enhanced patient comfort as a supplementary advantage [16-18]. IOS increases efficiency by enabling digital transmission of impressions directly to the laboratory, rather than relying on conventional mail. Moreover, digital impression files can be electronically stored, reducing space management concerns and facilitating efficient record-keeping practices. At the outset, digital scanners were bulky and costly, restricting their availability to a select few innovative dental practices. With technological advancements and the emergence of smaller, more cost-effective scanners, digital impression systems have gained widespread adoption in dental offices globally.
From dentists' perspectives, IOS was found to require minimal chairside support, is easy to learn for beginners, and provides high efficiency [19]. It also improved visualization, simplified capture, reduced costs, and streamlined lab communication [19]. Moreover, the results of this study highlight the patients’ preference for IOS over conventional impression materials for recording intraoral data, in agreement with previous studies. The primary reasons for patients favoring digital impressions include the avoidance of pain or sensitivity, breathing difficulties, gag reflex, and unpleasant sensations such as taste, smell, or heat during the procedure. Additionally, the shorter appointment duration and the smaller size of the intraoral device further contributed to the preference for IOS over conventional methods [2, 20]. These findings align with previous studies indicating that patients generally prefer digital impressions to traditional ones due to the greater comfort and ease of the process, as well as a final prosthesis that fits well and meets aesthetic expectations [21, 22]. Therefore, embracing digital impressions has the potential to notably improve the dental experience for both practitioners and patients [23].
Digital impressions offer several advantages over conventional methods, they are not without limitations [5]. Clinical difficulties can lower digital impression accuracy, particularly in full-arch prosthetics where intra-arch discrepancies are frequent [3, 19] and in teeth with deep subgingival margins, which can impair scan accuracy [22]. There are still restrictions even though appropriate retraction, fluid management, and clinical expertise may increase accuracy in deep margins [24]. Nonetheless, traditional impressions continue to show consistent accuracy and are frequently employed, especially in intricate situations and long-span edentulous areas [5, 20, 25]. For implant-supported restorations, IOS had the lowest accuracy compared to the conventional open-tray pick-up method and the closed-tray technique [26].
Furthermore, the price and learning curve of digital impression with IOS may prevent their widespread use. These results highlight the necessity of selecting the appropriate impression method according to the clinical requirements, case complexity, and practitioner expertise [3, 8, 9, 22, 25, 26].
Neither impression technique induced gag reflex or queasiness in the majority of participants. This outcome is likely due to the fact that all procedures were performed by dental specialists and consultants, whose expertise could contribute to a more comfortable and controlled experience for the patients. A dentist's experience and years of service have been related to positive patient experience and increased satisfaction [27, 28]. Years of experience would enhance a dentist’s technical and communication skills with the patients. The former was found to be an essential factor in patients’ satisfaction, comfort, and loyalty [28].
This study also investigated the effect of tooth location, including maxillary and mandibular anterior and posterior teeth, on patients’ preferences. These variables were included in the same subject in an attempt to reduce inter-subjects’ variability in patients' experience. It has been suggested that IOS provides superior accuracy and precision in the anterior region compared to the posterior region [29]. Our findings showed that tooth location seemed to have no impact on patients’ satisfaction toward impression making procedure.
While digital dentistry and CAD/CAM workflows have clear benefits, a considerable proportion of dentists still refrain from using IOS [7]. Some dental practices may face infrastructural limitations or financial constraints that impede their ability to procure digital impression systems, thereby potentially limiting the accessibility of this technology in certain regions or communities [7]. This study is among the first to explore digital vs. conventional impression preferences specifically within a Saudi prosthodontic setting, contributing novel data in a region where digital infrastructure is still developing.
It is noteworthy that a within-subject retrospective study design was used in this study, compensating for the small sample size. This would reduce the variability between subjects and, consequently, reduce the need for a larger number of participants. Moreover, the study sample appears to be representative of the local Saudi population, as a similar distribution was observed across different adult age groups (Table 2), as well as between genders: male (45.0%) and female (55.0%). The samples were recruited equally from two different governmental hospitals, both equipped with CAD/CAM machines and IOS. This adds strength to the results, as patients receiving treatment in these hospitals represent a wide range of socioeconomic backgrounds.
5. STUDY LIMITATION
As a limitation of this study, patients underwent the two impression techniques on different visits, which may introduce recall bias. One week was the maximum allowed time period between visits in this study in an attempt to minimize recall bias. It has been suggested that one to seven days is an acceptable time period to avoid recall bias [30]. Registration priority in governmental hospitals is primarily given to Saudi citizens. This resulted in a very small number of non-Saudi participants in the current sample. In addition, this research was confined to multiple centers in one region of the country; therefore, results should be taken with caution. Furthermore, the study highlights a clear patient preference for digital impressions and emphasizes that demographic variables such as gender, age, or education had minimal influence. For better generalization, Future research may investigate cost-effectiveness and long-term clinical accuracy of digital methods, expanding sample recruitment to include private clinics and different regions of the country.
CONCLUSION
The findings of this study support the growing preference for digital impression techniques among patients receiving prosthodontic treatment. Digital methods demonstrated significantly greater patient comfort and reduced procedural anxiety. These insights highlight the value of integrating digital workflows in routine prosthodontic treatments in Saudi Arabia.
Considering the limitations of this study, it can be concluded that:
1- Digital impression techniques provide more reduction in queasiness, breathing difficulty, and discomfort during impression taking, compared to conventional methods.
2- IOS reduces patient’s anxiety and discomfort, which makes the impression taking visit more pleasant and acceptable, compared to conventional impression materials.
3- Generally, digital impression techniques are preferable over conventional methods among prosthodontic patients in Saudi Arabia.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: G.Z.A., L.T.A.: Study conception and design, and draft manuscript; A.W.T., O.A.G., A.A.B.: Data collection; A.A.A.: Analysis and interpretation of results. All authors have read and agreed to the published version of the manuscript.
LIST OF ABBREVIATIONS
| CAD/CAM | Computer-Aided Design and Computer-Aided Manufacturing. |
| CBCT | Cone Beam Computed Tomography |
| IOS | Intraoral Scanner |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| KSA | Kingdom of Saudi Arabia |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Taibah University College of Dentistry Research Ethics Committee, reference number TUCDREC/020624/GZAlmadani.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants for the use of their responses and anonymized data for research and publication purposes. The consent form was on the first page before they started the questionnaire.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo Repository at https://doi.org/10.5281/zenodo.15994033, reference number 15994033.
ACKNOWLEDGEMENTS
Declared none.

