All published articles of this journal are available on ScienceDirect.

Patients' Perception and Acceptance of Innovative Interdental Cleansing Devices: A Survey-Based Study
Abstract
Introduction
The study aims to evaluate the perceptions and acceptance of innovative interdental cleansing devices, providing insight into participants' perspectives on adopting these important oral hygiene tools.
Methods
This cross-sectional survey-based study was conducted at King Abdulaziz University Dental Hospital. A total of 377 patients were selected, and participants were surveyed online through a questionnaire. The data collected included demographic information, preferences for oral hygiene maintenance, and perceptions, acceptance, and preferences regarding a new interdental device. Statistical analysis was performed using SPSS 27.
Results
The study demonstrates a strong acceptance of the new interdental cleansing device among participants. Specifically, 82.5% reported having used the device, and 78.8% found it more comfortable than traditional methods. Additionally, 79.6% preferred the new device over the traditional approach, and 68.2% noted that it provided better cleaning between their teeth.
Discussion
This study supports the strong acceptability of a new interdental device among patients, as it also aligns with the current literature, which shows evidence that modern oral hygiene devices improve oral hygiene. These results solidify the need for user-friendly designs. However, subjective evaluation data and a lack of clinical confirmation represent significant drawbacks, thus requiring longitudinal and clinically controlled studies.
Conclusion
Most participants widely accept the interdental cleansing device. These devices are faster, more comfortable, and more effective than traditional alternatives. Most of the participants expressed interest in adopting the interdental cleansing device, highlighting its market potential and strong demand. This suggests that these devices are effective in improving oral hygiene.
1. INTRODUCTION
Oral hygiene is crucial for maintaining overall health, and its importance is increasingly recognized as a key component of general health [1]. Various factors, including personal knowledge, attitudes, behaviors, and individual perceptions of health, influence both oral health and overall health. Research shows that individuals who are informed about oral health tend to maintain better oral hygiene [2]. Poor oral hygiene can lead to several serious health issues, such as carcinomas, infective endocarditis, and aspiration pneumonia. Oral squamous cell carcinomas are among the most prevalent cancers in the Southeast Asian subcontinent, and studies indicate that factors contributing to these cancers are often linked to inadequate oral hygiene [3]. Additionally, the normal bacteria found in the mouth can cause infective endocarditis. Lockhart et al. noted that this condition is particularly common among individuals who experience gingival bleeding after brushing their teeth [4]. Oral health is frequently neglected in elderly individuals. However, maintaining good oral hygiene is particularly important for this demographic. Khadka et al. explored the connection between aspiration pneumonia and oral health in older adults, revealing that bacterial colonization in the mouths of those who do not receive professional oral care is often associated with prolonged respiratory infections [5]. Traditional methods, such as dental floss, have been used for a long time to maintain oral hygiene [6]. However, there has been a shift toward new interdental cleansing devices that are gaining popularity due to their enhanced hygiene levels and increased user compliance. These innovative devices have shown significant effectiveness in reducing plaque and improving gingival health [7]. Despite their advantages, interdental cleansing devices have limitations. Many of them require a certain level of hand dexterity for effective use. Studies have shown that individuals with physical impairments often struggle to utilize devices like dental floss and interdental brushes effectively [8].
Using interdental cleansing devices regularly poses a significant challenge for many individuals, as these tools can be difficult to incorporate into daily routines [9]. Furthermore, certain interdental cleansing devices, such as traditional floss and some interdental brushes, may struggle to reach deep interproximal spaces adequately. Holtfreter et al., highlighted that while flossing is more effective than interdental brushes for plaque removal in patients with very tight contacts, it has its limits [10]. Moreover, some interdental devices can lead to gingival trauma and discomfort; a study by Chipre and Shah indicates that enhancing awareness of proper dental device usage can foster better oral hygiene practices [11]. However, improper use of these tools can result in gum recession and injuries, ultimately discouraging daily use. The study conducted by Patil et al., demonstrated a significant lack of knowledge among dental undergraduate students regarding the use of interdental aids [12]. This underscores the importance of understanding patient perceptions and acceptance when transitioning from traditional cleansing tools to more advanced oral hygiene technologies. Such advancements often emphasize personalization, adapting to the user's specific dental anatomy for a more tailored and effective cleaning experience. For instance, many modern devices allow customization based on individual dental structures, ensuring a precise fit. Additionally, features such as adjustable cleaning intensity, duration, and patterns can often be controlled via a connected app, providing a truly personalized oral hygiene experience.
Recent research has demonstrated that the effective use of interdental brushes and water flossers offers superior cleaning capabilities compared to traditional dental floss, significantly improving plaque removal and reducing gingival inflammation [7, 13]. This increasing body of evidence underscores the importance of educating patients about the benefits of using interdental cleansing devices. Innovations in this field are rapidly advancing, enhancing overall oral health. For instance, the introduction of adjustable sizes and sonic vibrations has improved both the accessibility and effectiveness of these devices [14]. Additionally, electric brushes equipped with rotary features are more effective at removing plaque than manual brushes and traditional options, highlighting the vital role of technology and innovation in daily oral hygiene routines. Despite the evident advantages, the availability and acceptance of interdental cleansing devices remain barriers to their widespread adoption. Several studies suggest that a lack of awareness about these innovative tools significantly impacts individuals' willingness to incorporate them into their oral hygiene practices [15].
Several factors significantly influence patients' perceptions regarding oral hygiene practices, including familiarity with traditional methods, the cost-effectiveness of devices, recommendations from dental professionals, and the perceived complexity of using new tools. Understanding these perceptions is crucial for developing targeted educational strategies that promote effective oral hygiene practices. This survey-based study primarily aims to provide valuable insights into how diverse populations perceive and incorporate interdental cleansing devices into their daily oral health routines.
The findings of this study will enhance understanding of patient behaviors, which can assist manufacturers in refining their products and assessing the viability of such devices. Furthermore, dental professionals play a crucial role in shaping patients' perceptions of innovative interdental cleansing devices. By discussing and integrating these tools into routine dental visits, practitioners can significantly influence patients' acceptance and utilization of these devices. Dental professionals can effectively educate patients about the benefits and proper techniques for using these tools.
This research investigates the perspectives and acceptance of interdental cleansing devices through a survey-based methodology, providing a fresh and unique insight into patients' attitudes and behaviors toward adopting these essential oral hygiene tools. The study specifically aims to evaluate the effectiveness and user adaptability of the patented Interdental Cleansing Device (US 11,179,230 B1) in comparison with traditional techniques.
Additionally, the research will provide valuable knowledge for public health initiatives aimed at improving oral hygiene practices within the community. The results may guide the design and implementation of interventions to address prevalent misconceptions or concerns surrounding interdental cleansing. By empowering dental professionals to encourage the use of these devices, public health campaigns can become more persuasive and effective.
This study also identifies key barriers to the acceptance of interdental cleansing devices, including cost, accessibility, perceived difficulty of use, and a lack of awareness about the importance of interdental cleansing. Gaining insights into these factors will be crucial for developing targeted strategies in oral hygiene campaigns that focus on specific populations, thereby enhancing overall oral health.
2. MATERIALS AND METHODS
2.1. Study Settings and Design
The study utilized a cross-sectional design conducted at King Abdulaziz University Dental Hospital to evaluate patients' perceptions, acceptance, and preferences regarding the new interdental cleansing device in Jeddah, Saudi Arabia. The participants were directed to use the Interdental Cleansing device (US 11, 179, 230 B1) according to the manufacturer’s guidelines. The device included upper and lower trays that consisted of pre-threaded floss, allowing for simultaneous interdental cleaning.
2.2. Sample Size
The required sample size for this cross-sectional survey was determined using the Raosoft sample size calculator, with a 95% confidence level, 5% margin of error, and a response distribution of 50%. An estimate of the minimum recommended sample size in the target population was determined to be 377 participants. To ensure adequate power and generalizability of the findings in the dental hospital setting, this sample size was chosen. A convenience sampling method was used to recruit individuals who fulfilled the inclusion criteria and attended their visits at King Abdulaziz University Dental Hospital in Jeddah.
2.3. Pilot Study
The feasibility and reliability of the questionnaire were assessed during a pilot study prior to conducting the main study. Fifty participants were included in the pilot study, recruited at King Abdulaziz University Dental Hospital, Jeddah, who had booked their dental appointments. A pilot study was conducted to ensure that the questions were understandable and suitable for worldwide use, and to measure the Interdental Cleansing Device according to the patent (US 11,179,230 B1).
Participants completed the questionnaire, which included demographics, oral hygiene preferences, and acceptance and perceptions of the Interdental Cleansing Device, only after trying it with the guidance of a dentist. All 11 measures in the “Acceptance and Perceptions” section were evaluated for reliability and validity due to their direct link to the study's aim and objectives. These items include questions regarding device use, ease of understanding, advantages, comfort, speed of usage, handling, and comparison with traditional methods (Appendix A).
2.3.1. Reliability Analysis
Reliability was determined by using Cronbach’s alpha in SPSS version 27. No answers were missing from any of the 50 people surveyed. With a Cronbach’s alpha score of 0.839, the results indicate that the questionnaire is internally valid, as scores above 0.7 are considered adequate. The data indicate that the questionnaire precisely recorded how participants felt about and accepted the device.
2.3.2. Validity Analysis
The construct validity of the scale was tested with Principal Component Analysis without rotation on the data from all 11 items. KMO was calculated as 0.796, which is greater than 0.6; therefore, the sample was sufficiently large for factor analysis. Since χ2 (235.798) ≥ 358.356, Bartlett’s Test of Sphericity showed that the correlation matrix could be used in factor analysis (df = 358.356, p < 0.001). The extracted components from PCA are three, with eigenvalues greater than 1, which explain 65.9% of the total variance: Component 1 at 42.3%, Component 2 at 13.5%, and Component 3 at 10.0%. All elements exhibited communalities of 0.566 or higher, indicating that the extracted components largely explained them. Item loadings for effectiveness, comfort, speed, handling, and preference on Component 1 (0.718-0.839) suggested that these items all fall under the same concept of device acceptance. Most of the weight was attributed to Component 2, indicating an independent dimension of awareness. The findings demonstrated that the instrument can accurately measure device perceptions.
2.3.3. Descriptive Findings
The pilot study gave some preliminary information about the participants. Using the data collected from the 50 participants, 48.0% used the interdental cleansing device, 52.0% had heard of it, and 58.0% had tried it (noted as “AI-powered” in the pilot, which was corrected to “Interdental Cleansing Device” in the main study due to a terminology error). More than half found the device easier to use (64.0%), better at cleaning back teeth (66.0%), best at cleaning between the teeth (70.0%), additionally it was more convenient (68.0%), helped them save time (72.0%), was easier to handle (66.0%), better to use than conventional toothbrushes (64.0%) and most respondents would recommend it (68.0%). Results from these tests confirmed that the questionnaire records meaningful impressions, as suggested by the main results.
2.3.4. Refinements
Participants in the pilot were asked to clarify some questions; the phrase “AI-powered device” was not clear to everyone. For this reason, we updated the term “AI-powered” to simply “the Interdental Cleansing Device (US 11,179,230 B1)” for better understanding. Two more questions were excluded from the section on “Acceptance and Perceptions” because respondents indicated they did not make much sense, and some were repetitive. Questions about design appeal and general user preferences did not align closely with the main goal of the study. All remaining questions were simplified and clarified in language, and we updated the instructions to ensure everyone knew how to operate the device. The pilot confirmed that online testing was feasible and that a completion time of 15 minutes was acceptable. There was no need to make major adjustments to the main questionnaire, as both its reliability (Cronbach’s alpha = 0.839) and validity (KMO = 0.796, explaining 65.9% of the variance) results provided support for the main study.
The findings of the pilot study helped design the main study’s questionnaire to reliably assess patient perceptions and acceptance of the Interdental Cleansing Device. High reliability and enough validity supported the tool, and using an approach to fix flawed questions improved its focus and simplicity.
2.4. Device Detail
The interdental cleansing device, as described in U.S. Patent No. 11,179,230 B1, is a customizable interproximal flossing device designed to enhance the efficiency and thoroughness of oral hygiene by simultaneously flossing all interproximal spaces between teeth. The device comprises two primary components: a first tray and a second tray, each produced as a single contiguous body tailored to fit the user's upper and lower jaws, respectively. The first tray features a first inner surface and a first outer surface that form a trench configured to surround the teeth of the upper jaw, while the second tray similarly forms a trench for the lower jaw's teeth. Each tray is equipped with a plurality of hooks disposed along the inner surfaces, designed to guide strands of dental floss threaded through them. Positioned in any one of the individual recesses or channels, these hooks prevent the floss from entering the tangential spaces between the adjacent teeth except when it is used. A handle couples the trays close enough together so that, when inserted into the mouth, the trays are held substantially parallel to one another, allowing simultaneous flossing of the upper and lower jaws. The device further includes at least one interproximal brush mounted on either or both trays to function as a floss for specific interproximal spaces. In addition, the device may have a motor with a switch providing “on,” “off,” and optionally intermediate speed settings to automatically perform the flossing action, similar to devices in electric toothbrushes. It may also have a storage compartment for the floss, enhancing usability. The device is custom-made based on the dental impressions of the user's teeth and gums, guaranteeing a good fit that eliminates the need for the user to spend hours learning the art of flossing with traditional methods. Conventional finger flossing suffers from disadvantages in terms of effort, time, and accessibility, which this design addresses [16].
2.5. Data Collection Tool
Data were collected through an online questionnaire administered to participants who had visited the facility. Participants’ dental visits were followed by the administration of an online questionnaire using tablets provided in the waiting room, guided by trained dental professionals to use the device according to the manufacturer's guidelines. All participants had previous practical experience with the device before taking the survey, which provided a consistent background for data collection. We note that participants were already very familiar with the device due to previous exposure from the hospital dental outreach programs, which offered community workshops and provided information at past dental appointments. The survey questionnaire to assess their perceptions, acceptance, and preferences consisted of three parts: (1) Demographics, which included age, gender, education status, domicile, present dental conditions, last dental visit, and number of dental visits per month; (2) Personal Preferences and Oral Hygiene, which included participants' existing oral hygiene habits and preferences; and (3) Acceptance and Perceptions of the Innovative Interdental Device, which specifically focused on the participants' views regarding the new interdental device.
2.6. Inclusion and Exclusion Criteria
The inclusion criteria target patients aged 18 and older who can provide informed consent. Exclusion criteria include individuals under 18, adults with cognitive impairments who are unable to consent, and patients with severe physical limitations that hinder effective device use. Recruitment employed a convenience sampling method, where dental staff shared flyers and verbally invited patients attending scheduled routine check-ups or treatments, excluding those requiring local or general anesthesia, such as extractions. Patients with prior appointments were respectfully informed by being passed the study information and explained participation based on the nature of their visits.
2.7. Ethical Consideration
The Research Ethics Committee of the Faculty of Dentistry, King Abdulaziz University, approved the study protocol (Reference Number: 90-09-24). This study adhered to all procedures outlined in the ethical standards of the relevant committee on human experimentation and the Helsinki Declaration of 1975, as revised in 2013.
All participants were included in the study, having provided their informed consent. All information was anonymized prior to analysis, and participants were assured of the confidentiality of their responses. The study was designed to be entirely voluntary, and participation was specifically not connected in any way to participants’ dental care; thus, any of them could withdraw at any time without suffering adverse effects to the dental care they received.
2.8. Statistical Analysis
Statistical analysis was conducted using SPSS version 27. Descriptive statistics were used to calculate frequency distributions among participants regarding their demographic information, Personal Preferences for Oral Hygiene, and their perception and acceptance of new interdental devices.
Statistical analysis was conducted using IBM SPSS Statistics software, version 27. Demographic characteristics, oral hygiene preferences, and perceptions on the interdental cleansing device were summarized using descriptive statistics (frequencies and percentages).
The last eleven questions of the questionnaire were designed to calculate an Acceptance Level Score for each participant, evaluating their perceptions and acceptance of the interdental cleansing device. The reliability of these questions was assessed through a high Cronbach’s alpha value of 0.839, indicating that they effectively measured a single underlying construct. Based on the total scores, participants were subsequently categorized into three distinct levels of acceptance.
- Score 0-4 = Low acceptance.
- Score 5-7 =Acceptance of moderate but not high
- Score 8-11 = high acceptance.
The chi-square test for independence was used to evaluate associations between the acceptance levels and demographic variables (age, gender, education, and domicile). Furthermore, Spearman’s rho correlation was used to determine the strength and direction of the relationship between acceptance levels and continuous or ordinal variables. Statistical significance was considered at a p‐value less than 0.05.
3. RESULTS
3.1. Demographics
To assess patient perceptions and Acceptance of Innovative Interdental Cleansing Devices, a total of 377 participants were included in the study. Table 1. Shows the demographics of the study population. There were 185(49.1%) females and 192(50.9%) males. The age was categorized into four different categories, with most of the recruited patients falling into the 18 to <25 years old category (87, 23.1%), followed by 81 (21.5%) participants aged between 35-<45 years, and 25-<35 years, accounting for 75 (19.9%). Educational Level was categorized into five different categories, in which 86 (22.8%) participants had a PhD or higher level of education, 69(18.3%) had a Master's, 70(18.6%) had a Bachelor's, 69(17.5%) had completed their high school, and 86(22.8%) had less than a high school diploma.
Participants were almost equally divided between those with rural (184, 48.8%) and urban (193, 51.2%) domiciles. Eighty-five (22.5%) participants reported visiting the dentist almost twice a month. One hundred forty-one (37.4%) participants last visited the dentist between 2 to 6 months ago. Eighty-four (22.3%) participants reported that they do not have any dental conditions. However, participants reported experiencing gum problems (113, 30%), dental caries (92, 24.4%), and missing teeth (88, 23.3%).
Table 1.
| Demographics | n (%) | |
|---|---|---|
| Gender | Female | 185 (49.1%) |
| Male | 192 (50.9%) | |
| Age | 18-<25 years | 87 (23.1%) |
| 25-<35 years | 75 (19.9%) | |
| 35-<45 years | 81 (21.5%) | |
| 45-<55 years | 69 (18.3%) | |
| 55 years or older | 65 (17.2%) | |
| Education | Bachelor’s degree | 70 (18.6%) |
| High school graduate | 66 (17.5%) | |
| Less than a high school diploma | 86 (22.8%) | |
| Master’s degree | 69 (18.3%) | |
| PhD or higher | 86 (22.8%) | |
| Domicile | Rural | 184 (48.8%) |
| Urban | 193 (51.2%) | |
| Frequency of dental visit in a month | More than three times | 75 (19.9%) |
| None | 77 (20.4%) | |
| Once | 67 (17.8%) | |
| Three times | 73 (19.4%) | |
| Twice | 85 (22.5%) | |
| Last dental visit | < 2 months | 123 (32.6%) |
| > 6 months | 113 (30.0%) | |
| 2-6 months | 141 (37.4%) | |
| Dental conditions | Dental caries (tooth decay) | 92 (24.4%) |
| Gum problems | 113 (30.0%) | |
| Missing teeth | 88 (23.3%) | |
| None | 84 (22.3%) | |
3.2. Personal Preferences for Oral Hygiene
The personal preferences of the study participants for maintaining oral hygiene are presented in Table 2 and Figs. (1 and 2). Of the 377 participants, nearly half reported that they do not consider maintaining oral health necessary (188, 49.9%), 126 (33.4%) were unsure of their oral health condition, and 134 (35.5%) reported poor oral health. In contrast, 117 (31.0%) reported good oral health. Additionally, 187 (49.6%) participants had tooth discoloration, 129 (34.2%) reported experiencing bad breath, and 121 (32.1%) were unsure whether they had bad breath. Fig. (1) illustrates the distribution of brushing habits, showing that brushing frequency was nearly evenly distributed: 96 (25.5%) participants reported not brushing their teeth. At the same time, similar numbers reported brushing once or twice a day. The duration of brushing was also comparable across groups, with 126 (33.4%) brushing for less than 1 minute, 128 (34.0%) for 1 to 2 minutes, and 123 (32.6%) for more than 2 minutes. Most participants used horizontal strokes (112, 29.7%), followed by those using all types of brushing techniques (103, 27.3%), and most preferred medium bristle brushes (107, 28.4%). Additionally, most participants changed their brushes every three months (109, 28.9%). Fig. (2) shows survey responses on interdental cleansing devices, indicating that the participants did not clean their tongue while brushing (196, 52.0%), but 205 (54.4%) found interdental cleansing necessary. Furthermore, 194 (51.5%) had a flossing habit, with 106 (28.1%) flossing three times a day, and 103 (27.3%) using unwaxed floss. A total of 192 (50.9%) participants reported interdental brushing, and 196 (52.0%) experienced gum bleeding when using an interdental cleansing device. Awareness of tooth decay causes was reported by 171 (45.4%) participants, 189 (50.1%) cleaned their teeth after eating sweets, and 198 (52.5%) did not follow their dentist’s advice, with 189 (50.1%) not having learned brushing techniques from a dentist.
| Variable | Response | n (%) |
|---|---|---|
| Health of teeth and gums | Bad | 134 (35.5) |
| Good | 117 (31.0) | |
| Not sure | 126 (33.4) | |
| Necessary to maintain oral health | No | 188 (49.9) |
| Yes | 189 (50.1) | |
| Bad breath | No | 127 (33.7) |
| Not sure | 121 (32.1) | |
| Yes | 129 (34.2) | |
| Teeth discoloration | No | 190 (50.4) |
| Yes | 187 (49.6) | |
| Aware of tooth decay causes | No | 206 (54.6) |
| Yes | 171 (45.4) | |
| Follows the dentist's advice | No | 198 (52.5) |
| Yes | 179 (47.5) |
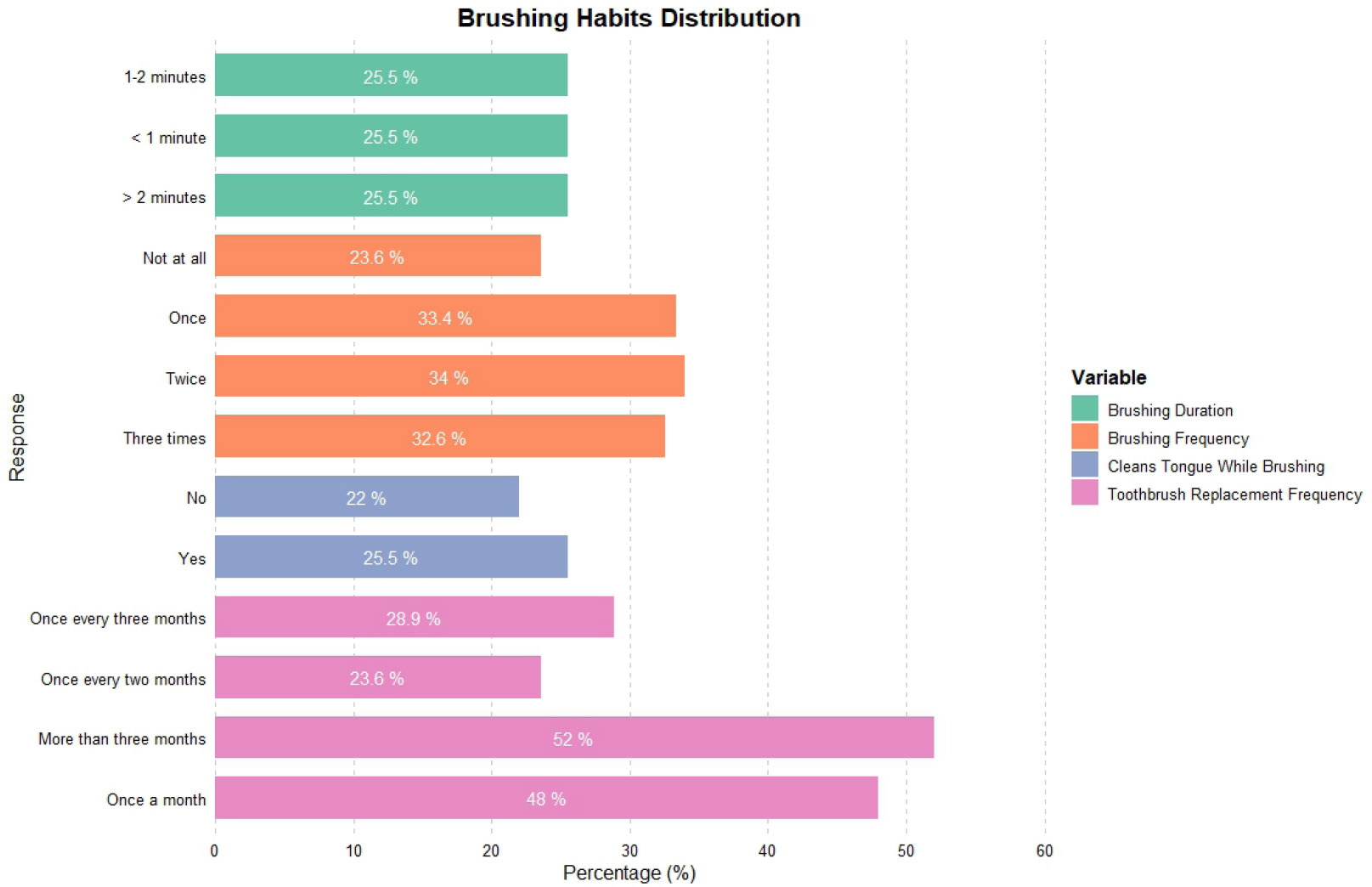
Brushing habits of participants, showing frequency, duration, technique, and bristle type preferences.
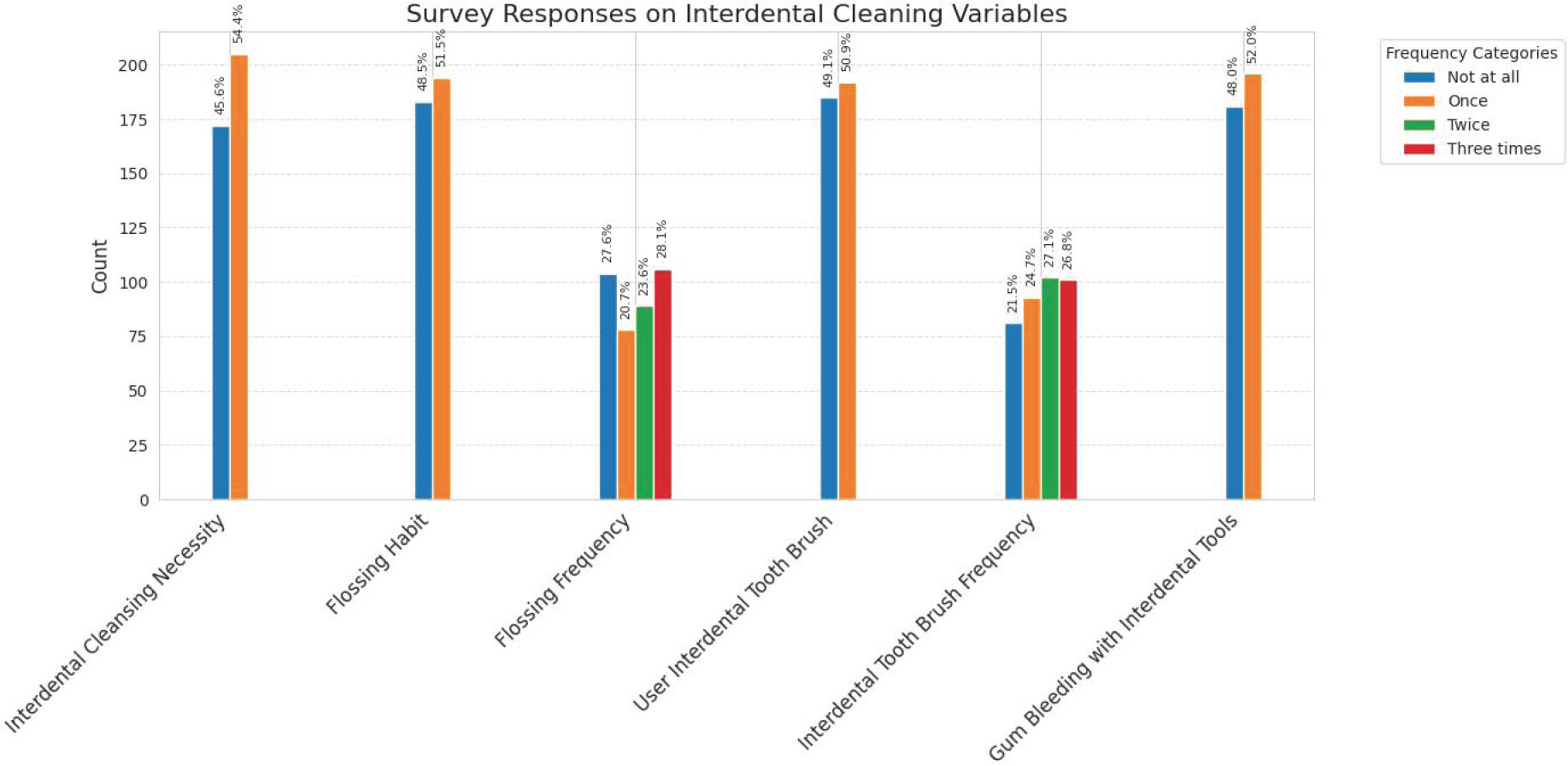
Interdental cleaning habits of participants, detailing tongue cleaning, flossing, gum bleeding, and awareness of oral hygiene practices.
3.3. Acceptance and Perceptions of The New Interdental Cleansing Device
Table 3 illustrates the acceptance and perceptions of participants regarding the New Interdental Cleansing Device, among a total of 377 participants. Specifically, 311 (82.5%) participants found the interdental cleaning device effective in cleaning their teeth, while 66 (17.5%) participants disagreed with this perspective. A total of 308 (81.7%) participants had heard about the interdental cleansing device before using it, 313 (83%) participants reported having used the device before, and 243 (64.5%) participants agreed with its effectiveness. However, 56(14.9%) were not sure and 78(18.6%) denied. New interdental cleaning devices were found to be more effective for cleaning back teeth in 249 (66%) participants, with improved reach to the interproximal areas of the teeth in 257 (68.2%) participants.
Comfort was another major factor assessed for the development and progression of new interdental devices. A total of 297 (78.8%) participants found this device more comfortable than the traditional one. Three hundred three (80.4%) participants reported that the new device was faster than the traditional method, with better handling support (299, 79.3%). Three hundred (79.6%) participants responded positively to replacing the traditional method with the new device, and 297 (78.8%) recommended this device to others.
| Acceptance and Perceptions with the New Interdental Cleansing Device | n (%) | |
|---|---|---|
| Used interdental cleaning aid | No | 66 (17.5%) |
| Yes | 311 (82.5%) | |
| Heard of a new device | No | 69 (18.3%) |
| Yes | 308 (81.7%) | |
| Used interdental cleansing device | No | 64 (17.0%) |
| Yes | 313 (83.0%) | |
| Found a new device more effective | No | 78 (20.7%) |
| Not sure | 56 (14.9%) | |
| Yes | 243 (64.5%) | |
| New device better for back teeth | No | 70 (18.6%) |
| Not sure | 58 (15.4%) | |
| Yes | 249 (66.0%) | |
| New device better for interproximal areas | No | 63 (16.7%) |
| Not sure | 57 (15.1%) | |
| Yes | 257 (68.2%) | |
| New device more comfortable | No | 80 (21.2%) |
| Yes | 297 (78.8%) | |
| New device faster than traditional device | No | 74 (19.6%) |
| Yes | 303 (80.4%) | |
| New device better handling | No | 78 (20.7%) |
| Yes | 299 (79.3%) | |
| Replace conventional methods | No | 77 (20.4%) |
| Yes | 300 (79.6%) | |
| Recommend new interdental cleansing device | No | 80 (21.2%) |
| Yes | 297 (78.8%) | |
| Variables | Acceptance Category | Gender | Education | Age |
|---|---|---|---|---|
| Acceptance category | 1.000 | -0.003 | -0.038 | -0.048 |
| - | (0.954) | (0.464) | (0.353) | |
| Gender | -0.003 | 1.000 | -0.021 | 0.094 |
| (0.954) | - | (0.687) | (0.070) | |
| Education | -0.038 | -0.021 | 1.000 | 0.084 |
| (0.464) | (0.687) | - | (0.102) | |
| Age | -0.048 | 0.094 | 0.084 | 1.000 |
| (0.353) | (0.070) | (0.102) | - |
Table 4 indicates weak and, for the most part, nonsignificant relationships between the Acceptance Category and the demographic variables of Gender, Education, and Age, as determined by Spearman’s Rho correlation coefficients (N = 377). There is a negligible correlation between the Acceptance category and Gender (ρ = 0.003; p = 0.954), indicating an insignificant relationship. Equally, the correlation with Education is weak (ρ = -0.038, p = 0.464) and negative (weak tendency to lesser acceptance with higher education, although not statistically significant). Furthermore, the correlation with age is weak and negative (ρ = -0.048, p = 0.353), indicating a slight tendency for acceptance to decrease with increasing age, although this is not statistically significant. Gender and age are demographic variables that exhibit a weak positive correlation (ρ = 0.094, p = 0.070), indicating a slight tendency for one gender to be associated with older age groups. The weak positive correlation is also between Education and Age (ρ = 0.084; p = 0.102) and between Education and Gender (ρ = -0.021; p = 0.687). Overall, the results suggest that the examined demographic variables do not exhibit a strong or statistically significant relationship with the Acceptance Category.
The chi-square test between demographic variables (Gender, Education, Age Group, and Domicile) and the Acceptance Category of the device is reported in Table 5. None of the demographic variables is statistically associated with any of the levels of acceptance (Low, Moderate, High). Distribution of high, moderate, and low acceptance was similar for males (0.5% Low, 24.0% Moderate, 75.5% High) and females (0.0% Low, 24.9% Moderate, 75.1% High; χ2 = 0.997, p = 0.607). There was no significant difference in acceptance patterns at different education levels. Master’s degree holders had the highest proportion of High acceptance (84.1%), while High School graduates had the lowest proportion (68.2%). However, the chi-square test (χ2 = 8.553, p-value = 0.381) was not significant. The highest acceptance rate was observed in the Age Group 18 - <25 (82.8%), and the lowest in the Age Group 25 - <35 (65.3%). however, the chi-square value (χ2 =12.735; p-value = 0.121) for this variable was not significant. For domicile, acceptance patterns were comparable between rural (Low 0.5%, Moderate 25.0%, and High 74.5%) and urban (Low 0.0%, Moderate 23.8%, and High 76.2%) sites (χ2 = 1.138, p-value = 0.566). Overall, no demographic variable was significantly influenced by acceptance categories, indicating that the acceptance of the device is largely independent of gender, education, age, and domicile.
4. DISCUSSION
This investigation gives insights from 377 patients at King Abdulaziz University Dental Hospital who were assessed and received the proposed interdental cleansing device (US 11,179,230 B1). This study demonstrates that utilizing an advanced dental tool can aid in maintaining good oral hygiene. However, it is essential to acknowledge that the findings are based on individuals' personal experiences, rather than clinical tests of the device's performance. Although participants' feedback suggests that the products were very effective, these results should be confirmed by clinical trials that measure plaque levels, gum health, and the reduction in the risk of tooth decay. As a result of this drawback, we see that user experiences tell us about adoption, but we should rely on clinical research to demonstrate a product’s efficacy.
| Variable | Category |
Low n (%) |
Moderate n (%) |
High n (%) |
Chi-square | p-value |
|---|---|---|---|---|---|---|
| Gender | Male | 1 (0.5%) | 46 (24.0%) | 145 (75.5%) | 0.997 | 0.607 |
| Female | 0 (0.0%) | 46 (24.9%) | 139 (75.1%) | |||
| Education | PhD+ | 0 (0.0%) | 23 (26.7%) | 63 (73.3%) | 8.553 | 0.381 |
| Master's | 0 (0.0%) | 11 (15.9%) | 58 (84.1%) | |||
| < High School | 1 (1.2%) | 19 (22.1%) | 66 (76.7%) | |||
| High School | 0 (0.0%) | 21 (31.8%) | 45 (68.2%) | |||
| Bachelor's | 0 (0.0%) | 18 (25.7%) | 52 (74.3%) | |||
| Age Group | 18-<25 | 0 (0.0%) | 15 (17.2%) | 72 (82.8%) | 12.735 | 0.121 |
| 25-<35 | 0 (0.0%) | 26 (34.7%) | 49 (65.3%) | |||
| 35-<45 | 0 (0.0%) | 16 (19.8%) | 65 (80.2%) | |||
| 45-<55 | 0 (0.0%) | 18 (26.1%) | 51 (73.9%) | |||
| 55+ | 1 (1.5%) | 17 (26.2%) | 47 (72.3%) | |||
| Domicile | Rural | 1 (0.5%) | 46 (25.0%) | 137 (74.5%) | 1.138 | 0.566 |
| Urban | 0 (0.0%) | 46 (23.8%) | 147 (76.2%) |
Participants reported that the interdental cleaning device was effective in helping to maintain their oral health. Studies have shown that interdental brushes and water flossers are more effective than regular floss in removing plaque and improving gum health. A review of studies by Kotsakis et al. [17] showed that using interdental brushes was much more successful at removing plaque between teeth than floss, mainly because of their ability to sweep away plaque in people with broader gaps in the back of their mouth. In addition, a review by Worthington et al. [18] concluded that liquid flossers worked better than string floss to control gingival bleeding, probably because liquid flosses are simpler to use and can go deeper between the teeth, aligning with these findings our results indicated that participants experienced significant ease of use and comfort with the prototype, suggesting that it may offer ergonomic benefits comparable to those observed with alternative tools. The fact that many people prefer this device represents an important insight that user-friendly design tactics, such as adjustable trays and the integration of upper and lower flossing, may resolve the primary issues with interdental cleaning. Since flossing can depend on good hand movement and requires a lot of time, it is often skipped by individuals who find it too difficult. The way the device is made, according to the patent [16], helps overcome these problems by automating flossing and fitting it to each person’s unique teeth and gums. This aligns with the findings of Ng and Lim [14], who suggest that using high-quality interdental tools helps individuals maintain good oral hygiene. Many people in the current study agreed that the interdental cleaning device was faster and more pleasant than regular dental floss, suggesting it could encourage them to maintain the habit long term, a key factor in preserving oral health. A similar study reported that an interdental brush was easier to use than daily flossing [19]. The study revealed an unexpected finding: age, gender, and education levels were not correlated with acceptance of the device. However, the high acceptance rate indicates that many people appreciated its design. This is significant because it contrasts with many other studies, which suggest that increased knowledge and information facilitate the adoption of new oral care methods for certain individuals [12]. This study suggests that improving understanding and educating individuals can encourage them to engage in and promote interdental cleaning. The knowledge gaps regarding tooth decay and inconsistent adherence to oral health advice indicate that participants lacked sufficient knowledge about dental hygiene. These findings align with those of Chipre and Shah and Vandana et al., who noted that a lack of knowledge about interdental aids often prevents their use and leads to poorer oral hygiene [11, 20]. Dental experts can help bridge this gap by explaining the purpose of interdental cleaning and demonstrating the correct techniques for practicing it. According to a study by Worthington et al. [18], guidance from dental professionals significantly increased the number of patients with periodontal disease who began using interdental brushes. Adding the interdental cleansing device to routine dental visits may also increase patient willingness and compliance. Furthermore, the study results clarify the broader impact of interdental cleaning on oral health. Proper care of interdental spaces may reduce the chances of developing cavities, periodontal disease, and potential tooth loss. According to Nakao et al. [21], a five-year follow-up study demonstrated that the use of interdental brushes significantly helped reduce tooth loss rates. Similarly, Marchesan et al. [22] found, using data from the National Health and Nutrition Examination Survey, that the use of interdental cleaning tools decreased the risk of caries and gum disease. The study's limitations restrict its ability to provide clinical outcomes, underscoring the need for future studies to evaluate the device's impact on plaque indices, gingival inflammation, and caries incidence. Traditional brushing cannot effectively clean the areas between teeth, unlike the device discussed here, which offers significant advantages. Barbe et al. [23] and Weik et al. [24] reported that brushing alone cannot completely remove the plaque between the teeth in patients with poor hygiene. It is important because plaque builds up most frequently between teeth, leading to gingivitis, periodontitis, and caries. According to the current studies, respondents reported that the device removed interproximal plaque, which agrees with findings highlighting the advantages of using interdental tools. A study, conducted by Slot et al. [25], showed that interdental brushes were twice as effective as brushing alone in reducing interproximal plaque.
The findings indicate significant concerns that may impact public health intervention initiatives. While the interdental cleansing device has gained widespread acceptance, its market potential remains promising. However, challenges related to high costs, limited purchasing options, and low consumer awareness must be addressed to facilitate broader adoption. Graziani et al. [26] demonstrated that advanced oral cleaning tools are often prohibitively expensive for most consumers in low-income groups. This problem can be resolved through public health initiatives that raise awareness of more affordable devices or help support the development of new ones like this. Community oral health programs may be strengthened by adopting these new tools.
This study provides knowledge about the perceptions and acceptance of the innovative interdental cleansing device. However, several limitations must be taken into account. Since participants recorded their oral hygiene habits, opinions, and experiences of the tool via self-reported information using an online questionnaire, there is a greater likelihood of self-reporting bias, which can result from both overreporting and underreporting. This may affect the reported validity of acceptance and efficacy. Additionally, non-response bias may have occurred because the survey was voluntary and conducted among patients visiting King Abdulaziz University Dental Hospital. The results may have been skewed toward more positive perceptions, as individuals who declined to respond may have systematically differed from those who did in terms of their degree of interest in oral hygiene or familiarity with interdental devices.
Furthermore, since participants’ excitement about the new device may have inflated these results, it is not possible to definitively link the observed benefits to the device without a control group of people who cleaned their interdental spaces solely with conventional dental floss or interdental brushes. The single-site design in Jeddah, Saudi Arabia, also limits generalizability, as the participant group may not accurately represent larger populations with varying geographic, cultural, or sociological contexts, despite diversity in terms of age, gender, and education. In turn, this may negatively impact device usage in other locations. The sampling technique and sample size may also have introduced selection bias, as these patients are likely more engaged in oral health practices than the general population. Moreover, the cross-sectional design only assessed opinions from brief interactions with the device under a dentist's supervision. Thus, the reported opinions primarily reflect initial impressions of adoption while excluding subsequent effects on sustained effectiveness, long-term use, and adherence. These outcomes may ultimately affect adoption rates due to factors such as cost, ease of integration into daily routines, and durability. Previous studies reported that device customization based on dental impressions, as described in US 11,179,230 B1, may raise accessibility problems in terms of cost and availability, particularly for individuals with physical limitations or limited dexterity [8]. This study did not address these issues. These limitations suggest that further research should incorporate control groups, longitudinal designs, multiple population groups, and strategies for addressing self-reporting and non-response biases, such as the use of objective measures and participation incentives. Such studies are necessary to validate and demonstrate these findings.
CONCLUSION
In conclusion, this study demonstrates that a substantial number of individuals appreciate the unique interdental cleansing device, underscoring its potential to improve the comfort, efficiency, and effectiveness of dental care. The findings underscore the importance of user-centered design and the necessity of professional guidance in advancing interdental cleaning practices. However, it is important to approach these results with caution, as the study relies on self-reported data. Further clinical research is needed to comprehensively evaluate the device's performance. The insights gained from this investigation can inform dental practices, drive product development, and support public health initiatives aimed at promoting the adoption of modern oral hygiene products.
AUTHOR’S CONTRIBUTIONS
The author confirms sole responsibility for the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Institutional Review Board of King Abdulaziz University - Faculty of Dentistry, Saudi Arabia (Reference Number: 90-09-24).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants before the survey commenced. The study was designed to be entirely voluntary, and participation was specifically not connected in any way to participants’ dental care; thus, any of them could withdraw at any time without suffering adverse effects to the dental care they received.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [M.B] upon reasonable request.
ACKNOWLEDGEMENTS
The author is very thankful to all the associated personnel who contributed to this research.
APPENDIX A
Section 1: Demographics
Gender
• Male
• Female
Age
• 18-24 years
• 25-34 years
• 35-44 years
• 45-54 years
• 55 years or older
Education
• Less than a high school diploma
• High school graduate
• Bachelor’s degree
• Master’s degree
• PhD or higher
Domicile
• Urban
• Rural
Frequency of Dental visits in a month
• None
• Once
• Twice
• Thrice
• More than thrice
When was the last time you visited a dentist?
• < 2 months
• 2-6 months
• > 6 months
Do you have any of the following dental conditions?
• Gingivitis
• Periodontitis
• Edentulism
• Dental caries
• None
Section 2: Personal Preferences and Oral Hygiene
How would you describe the health of your teeth and gums?
• Good
• Bad
Do you think it is necessary to maintain the health of your teeth and gums?
• Yes
• No
Do you experience bad breath?
• Yes
• No
Do you have teeth discoloration?
• Yes
• No
How often do you brush your teeth in a day?
• Once
• Twice
• Thrice
• Not at all
How long does it take for you to brush your teeth?
• < 1 minute
• 1-2 minutes
• > 2 minutes
What type of bristles do you prefer on your toothbrush?
• Soft
• Medium
• Hard
How do you brush your teeth?
• Circular strokes
• Horizontal strokes
• Vertical strokes
• All
How frequently do you change your toothbrush?
• Once a month
• Once every two months
• Once every three months
• After three months
Do you clean your tongue while brushing?
• Yes
• No
Do you think interdental cleaning is necessary to maintain oral health?
• Yes
• No
Do you floss?
• Yes
• No
How often do you floss your teeth in a day?
• Once
• Twice
• Thrice
• Not at all
What type of floss do you use?
• Waxed floss
• Unwaxed floss
• Tape floss
• Super floss
• Polytetrafluorethylene floss
• None
Do you use interdental toothbrush?
• Yes
• No
How often do you use interdental toothbrush in a day?
• Once
• Twice
• Thrice
• Not at all
What do you usually use to clean your teeth?
• Toothbrush
• Interdental device
• Dental floss
• Toothpick
• Others
Do your gums bleed when you use interdental toothbrush or floss?
• Yes
• No
Do you use interdental toothbrush or floss after having anything sweet?
• Yes
• No
Are you aware about the causes of tooth decay?
• Yes
• No
Have you learnt the correct technique of brushing and flossing to clean interproximal areas (space between adjacent teeth) from online videos or a dentist?
• Yes
• No
Do you follow the advice of your dentist?
• Yes
• No
Section 3: Acceptance, Perceptions, Experience and Satisfaction with the New Interdental Cleansing Device
Have you ever used an interdental cleaning aid?
• Yes
• No
Have you heard of the new Interdental cleansing device?
• Yes
• No
Have you used the new Interdental cleansing device?
• Yes
• No
Is the new Interdental cleansing device more effective in removing residual food than conventional interdental cleaning aids (interdental toothbrush and dental floss)?
• Yes
• No
Is the new Interdental cleansing device more effective in reaching the backmost teeth compared to conventional interdental cleaning aids?
• Yes
• No
Is the new Interdental cleansing device more effective in cleaning the interproximal areas (space between adjacent teeth) of tooth compared conventional interdental cleaning aids?
• Yes
• No
Is the new Interdental cleansing device more comfortable to use compared to conventional interdental cleaning aids?
• Yes
• No
Is the new Interdental cleansing device faster in cleaning teeth than conventional interdental cleaning aids?
• Yes
• No
Does Interdental cleansing device have a better grip than conventional interdental cleaning aids?
• Yes
• No
How satisfied are you with the quality of the Interdental cleansing device?
• Very satisfied
• Satisfied
• Neutral
• Dissatisfied
• Very Dissatisfied
How satisfied are you with the design of the Interdental cleansing device?
• Very satisfied
• Satisfied
• Neutral
• Dissatisfied
• Very Dissatisfied
How satisfied are you with the ease of use of the Interdental cleansing device?
• Very satisfied
• Satisfied
• Neutral
• Dissatisfied
• Very Dissatisfied
Would you replace conventional oral cleansing methods such as interdental toothbrushes and dental floss with Interdental cleansing device?
• Yes
• No
Would you recommend Interdental cleansing device to others?
• Yes
• No
Overall, how satisfied are you with Interdental cleansing device?
• Very satisfied
• Satisfied
• Neutral
• Dissatisfied
• Very Dissatisfied

