All published articles of this journal are available on ScienceDirect.

Impact of Sociodemographic Variables on Toothache Frequency, Dental Visits, and Oral Health Perceptions in Saudi Arabian Children: An Observational Study
Authors Info & Affiliations
Abstract
Introduction/Objective
Sociodemographic factors influence children's oral health outcomes, including toothache frequency, dental visits, and the reasons for the most recent dental visit. Age, gender, education, geography, and occupation are key variables affecting these outcomes. Understanding these factors is essential for developing targeted interventions to improve oral health. Despite global research on these issues, there is limited recent, region-specific evidence from Saudi Arabia, which this study aims to address.
Methods
A descriptive observational study was conducted among children aged 5–16 years across four regions in Saudi Arabia (Ha'il, Makkah, Medina, and Riyadh). A total of 570 children were included through convenience sampling. Associations between sociodemographic variables and outcomes (toothache frequency, dental visits, and reason for the last visit) were analysed using Chi-square tests and multinomial logistic regression with a significance level set at p < 0.05.
Results
Among 570 participants, 305 (53.5%) reported occasional toothaches, 40 (7.0%) frequent toothaches, and 75 (13.2%) had no dental visit in the past year. Pain was the most reported reason for the last dental visit (253 children, 44.4%). Sociodemographic variables, including age, gender, region, education of household head, and guardian occupation, showed statistically significant associations with oral health outcomes (p < 0.001). Multinomial logistic regression confirmed region-based disparities in toothache frequency.
Discussion
In the current study, oral health outcomes (tooth frequency, dental visits, and reasons for recent dental visits) showed significant relationships with all sociodemographic variables (age, gender, area, household head's education, and guardian occupation). In order to reduce socioeconomic disparities and encourage preventative oral health practices in Saudi Arabia, these findings emphasize the necessity of focused oral health interventions and policies.
Conclusion
Sociodemographic disparities play a critical role in children’s oral health in Saudi Arabia. Targeted interventions addressing regional, educational, and occupational influences are necessary. Future longitudinal studies are recommended to examine causal relationships and evaluate tailored intervention strategies.
1. INTRODUCTION
Sociodemographic factors influence children's oral health outcomes, including toothache frequency, dental visits, and the reason for the most recent dental visit. Age, gender, education, geography, and occupation are the sociodemographic variables influencing these oral health outcomes [1, 2].
Awareness of these variables is a prerequisite for developing focused therapies to improve oral health outcomes. Although these factors were explored by previous studies globally, there is a scarcity of research on youngsters in Saudi Arabia. The current study aims to bridge the research gap with an assessment of the influences of sociodemographic elements on toothache frequency, pattern of dental appointments, and the reasons for the most recent dental visit among Saudi youngsters.
Socioeconomic status, including both income and education, significantly influenced toothache frequency. In Australia, it was found that the prevalence of toothaches increased dramatically between 1994 and 2013, especially among those in the lower-income 25–64 age range [3]. A Finnish study found that throughout a 25-year period, the prevalence of toothaches varied somewhat but remained consistent among males with greater levels of education [4].
Research indicates that the prevalence of toothaches differs by gender. In general, women are more likely than men to report toothaches because of variations in how they experience pain and seek medical help [5]. Given that toothaches are more common in children and adolescents than in older individuals, age is a significant contributing factor to toothaches [6, 7].
According to a Brazilian study, early adolescent dental visits were significantly predicted by maternal education, socioeconomic class, and oral health literacy [8].
In Shenzhen, China, the pattern of dental visits among 12-year-old adolescents was substantially impacted by sociodemographic factors, such as caries severity, ways of maintaining oral hygiene and oral health-related knowledge [9]. In Mexico, unaddressed dental care needs and lack of health insurance were the major factors for dental visits related to pain [10]. In Spain, a lower likelihood of seeking dental care and worse oral health outcomes were reported in children from low-income families or children whose parents had lower levels of education [11, 12]. In Poland, despite the availability of free dental services to children, the utilization of dental services was determined by socioeconomic factors of financial limitations and parental education [13]. Numerous aspects of dental care utilization were brought into the limelight by these results, and these results highlight the importance of drawing immediate attention to address sociodemographic inequalities.
Precision public health measures are needed to enhance oral health and lower the frequency of tooth-related complaints in the young population of Saudi Arabia. The current study focused on analysing the sociodemographic factors associated with toothache frequency and oral hygiene practices. A better understanding of these factors can guide public health programs and policies aimed at improving the oral health of Saudi children. While such factors have been explored globally, recent region-specific data, particularly from underrepresented areas like Ha'il, remain scarce. This study aims to address this contextual gap and provide insights relevant to Saudi oral health planning.
2. MATERIALS AND METHODS
2.1. Study Design
This descriptive observational study was conducted to explore oral health outcomes among children in Saudi Arabia. Data were collected using a questionnaire distributed by licensed dentists in regions, including Ha'il, Makkah, Medina, and Riyadh. Before participation, informed consent was obtained from parents, and assent was collected from children aged 5-16 years. The data collection period spanned from January 2024 to April 2024.
2.2. Study Participants
Participants were recruited through a non-probability convenient sampling technique across different regions of Saudi Arabia. The inclusion criteria for the study were children under 18 years of age who lived with their parents and were mentally and physically fit. Children with special needs, such as autism, ADHD, cerebral palsy, Down syndrome, or other significant health issues, or those whose parents or guardians did not provide consent, were excluded from the study. Ethical approval was granted by the Scientific Research Committee of the Deanship of Research at the University of Ha’il, Saudi Arabia, under the approval number H-2023-365.
2.3. Study Variables
The study analyzed both independent and dependent variables:
2.3.1. Independent Variables
Sociodemographic factors, including age group, gender, region, education level of the household head, and guardian occupation.
2.4. Data Collection Tool
A validated and reliable questionnaire adapted from the World Health Organization’s (WHO) oral health survey methods was used for data collection [14]. The original questionnaire, designed to assess children’s oral health, was modified to include additional socio-demographic variables specific to Saudi Arabia. The questionnaire included 14 items addressing participants’ demographics and oral health-related outcomes. Responses were recorded in categorical formats tailored to the study’s focus on toothache frequency, dental visits, and reasons for dental visits.
2.5. Statistical Analysis
The collected data were manually coded and entered into SPSS software (version 27) for statistical analysis. Descriptive statistics were used to summarize the data in terms of frequencies and percentages. The Pearson Chi-Square test was applied to determine the relationships between sociodemographic factors and the oral health outcomes. A significance level of p < 0.05 was used for all tests.
To further explore the associations, multinomial logistic regression was performed, enabling analysis of the influence of independent variables on multiple categories of the dependent outcomes. Results were presented as odds ratios (ORs) with 95% confidence intervals (CIs). The goodness-of-fit of the regression models was assessed using pseudo R2 statistics, including Cox & Snell R2, Nagelkerke R2, and McFadden R2, which indicated moderate explanatory power. Multicollinearity among predictors was evaluated using the Variance Inflation Factor (VIF), and all values were below the acceptable threshold of 5. Visual representations of the data were created using bar and stacked bar charts to highlight trends and associations across variables.
3. RESULTS
Table 1 presents the distribution of participants by key demographic attributes, including age, gender, region, education of the household head, and guardian occupation. Among the 570 participants, the majority (47.4%) were aged 5-8 years, and 58.8% were female. Most participants resided in Medina (36.5%) or Makkah (33.3%). The educational level of household heads was predominantly a bachelor's degree (73.5%), while the majority of guardians worked in professional roles, such as teaching (31.9%) or office work (21.4%).
| Variable | Categories | n (%) |
|---|---|---|
| Age group (years) | 5-8 | 270 (47.4%) |
| 9-12 | 191 (33.5%) | |
| 13-16 | 109 (19.1%) | |
| Gender | Male | 235 (41.2%) |
| Female | 335 (58.8%) | |
| Region | Ha'il | 92 (16.1%) |
| Makkah | 190 (33.3%) | |
| Medina | 208 (36.5%) | |
| Riyadh | 80 (14.0%) | |
| Education (household head) | No education | 4 (0.7%) |
| Primary | 13 (2.3%) | |
| Middle | 18 (3.2%) | |
| Secondary | 75 (13.2%) | |
| Bachelor | 419 (73.5%) | |
| Diploma | 15 (2.6%) | |
| Postgraduate education | 26 (4.6%) | |
| Guardian Occupation | Agriculture | 3 (0.5%) |
| Business | 29 (5.1%) | |
| Daily laborer | 18 (3.2%) | |
| Teacher | 182 (31.9%) | |
| Driver | 5 (0.9%) | |
| Office worker | 122 (21.4%) | |
| Others | 211 (37.0%) |
| Question | Categories | n (%) |
|---|---|---|
| Q4: Toothache frequency | Often | 40 (7.0%) |
| Occasionally | 305 (53.5%) | |
| Rarely | 175 (30.7%) | |
| Never | 30 (5.3%) | |
| Don’t know | 20 (3.5%) | |
| Q5: Dental visits | Once | 88 (15.4%) |
| Twice | 200 (35.1%) | |
| Three times | 85 (14.9%) | |
| Four times | 24 (4.2%) | |
| More than four times | 58 (10.2%) | |
| No visit during the past 12 months | 75 (13.2%) | |
| Never had dental care | 20 (3.5%) | |
| Don’t remember | 20 (3.5%) | |
| Q6: Reason for last visit | Pain or trouble with teeth, gums, or mouth | 253 (44.4%) |
| Treatment/follow-up treatment | 170 (29.8%) | |
| Routine check-up | 50 (8.8%) | |
| No visit during the past 12 months | 85 (14.9%) | |
| Don’t know | 12 (2.1%) |
Table 2 summarizes participants' responses to key oral health-related questions. Most reported occasional toothaches (53.5%), while 7.0% experienced frequent toothaches. Regarding dental visits, 35.1% of participants visited the dentist twice in the past year, but 13.2% reported no visits. Pain or trouble with teeth was the most common reason for visits (44.4%), followed by follow-up treatments (29.8%).
The distribution of toothache frequency, dental visits, and reasons for the last dental visit by gender is illustrated in Fig. (1). Among females, “occasionally” was the most common toothache frequency, reported by over 50%, followed by “rarely” and “never.” Males exhibited a similar trend. Regarding dental visits, females most frequently reported visiting the dentist “once” or “twice,” similarly males also had higher proportions of once or twice visits.” The primary reason for dental visits among both genders was “pain,” especially among males, where it accounted for nearly 60%. Males reported more “treatment/follow-up” visits compared to females, while “check-ups” were reported by 10% respondents in both groups.
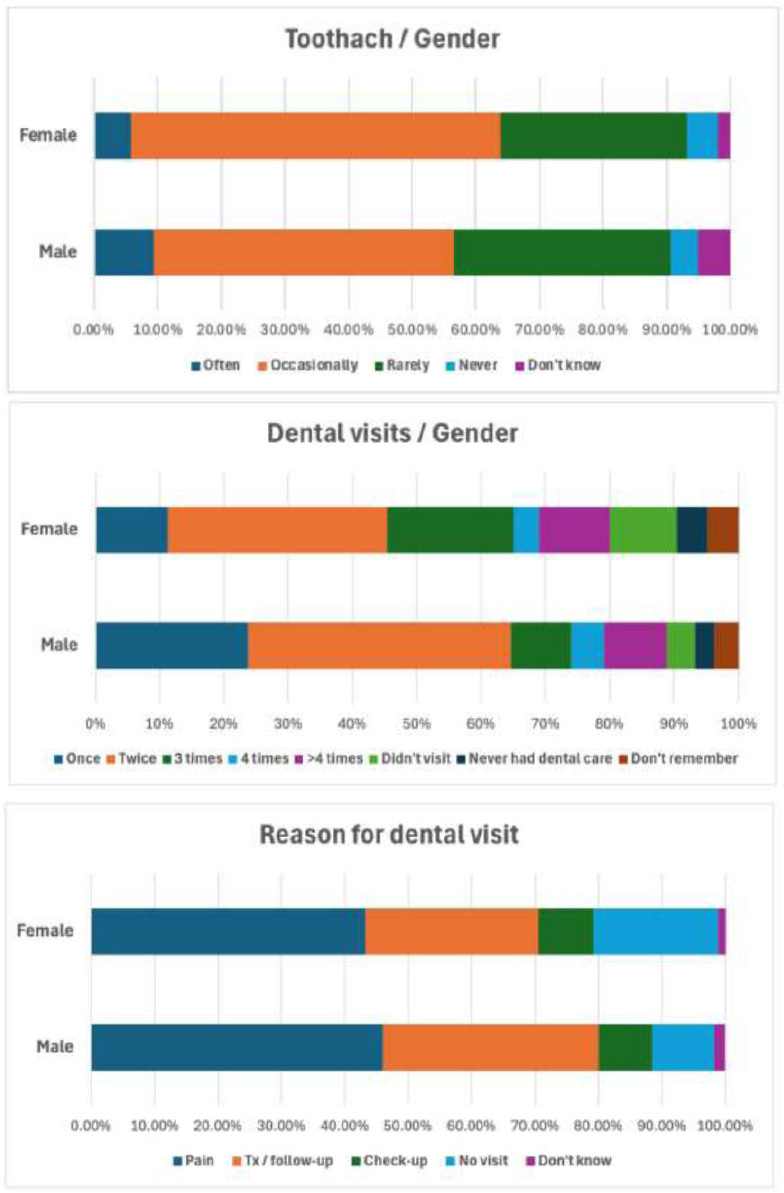
Distribution of toothache frequency, dental visit, and reason for last dental visit by gender.
Fig. (2) shows the distribution of toothache frequency, dental visits, and reasons for the last dental visit among three age groups: 5–8, 9–12, and 13–16 years. Toothache was most frequently reported as 'occasionally' across all age groups, with the highest proportion in the 5–8 years group. The 9–12 years group had the highest percentage of children who reported toothaches 'often,' while the 13–16 years group had the highest percentage reporting 'never.' For reasons for dental visits, pain was the most common across all age groups, with the 5–8 years group showing the highest percentage. A notable proportion of children in all groups reported 'no visit.
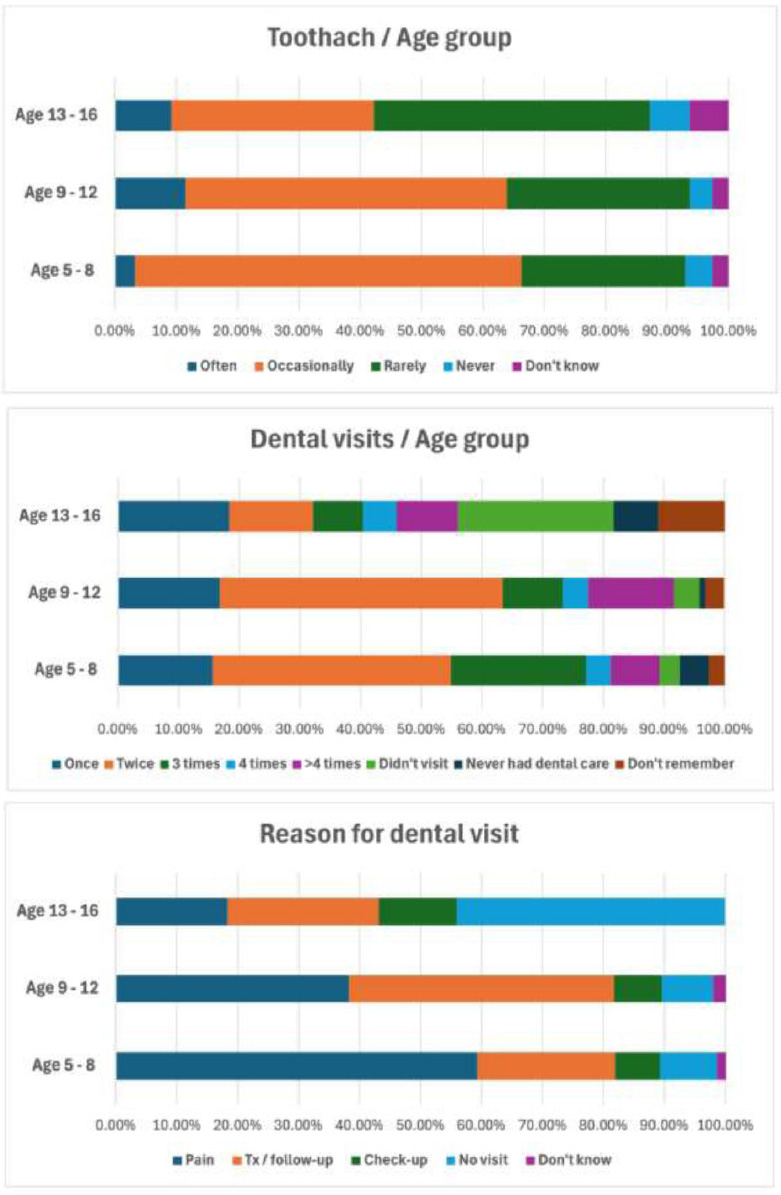
Distribution of toothache frequency, dental visit, and reason for last dental visit by age group.
Table 3 examines the associations between sociodemographic factors and oral health outcomes, including toothache frequency, dental visits, and reasons for the last visit. Chi-square tests (χ2) were performed for each outcome, with overall p-values reflecting the smallest p-value across the three outcomes. Adjusted p-values were calculated using the Bonferroni correction (0.05/3 = 0.017) to address the issue of multiple comparisons and ensure the observed associations are statistically robust. The value 0.05 was divided by 3 because 3 Chi-square tests were applied for each sociodemographic variable (tooth frequency, dental visits, and reasons for last dental visits).
All sociodemographic variables demonstrated significant associations with oral health outcomes, even after applying the Bonferroni correction. Age group showed strong associations with all outcomes, with p < 0.001 for toothache frequency (χ2 = 37.7), dental visits (χ2 = 116.4), and reasons for the last visit (χ2 = 126.5). Similarly, gender was significantly associated with dental visits (χ2 = 33.1, p < 0.001), resulting in an overall p-value of p < 0.001. Region also displayed significant associations, with p < 0.001 consistently observed across toothache frequency (χ2 = 20.5), dental visits (χ2 = 25.3), and reasons for the last visit (χ2 = 30.7). Education of the household head emerged as a critical factor, particularly influencing the reasons for the last visit (χ2 = 219.4, p < 0.001), while guardian occupation maintained significant relationships across all outcomes, including dental visits (χ2 = 148.8, p < 0.001).
| Sociodemographic Variable | Q4 (Toothache Frequency) (χ2, p-value) |
Q5 (Dental Visits) (χ2, p-value) |
Q6 (Reason for Last Visit) (χ2, p-value) |
Overall p-value | Adjusted p-value |
|---|---|---|---|---|---|
| Age Group | χ2 = 37.7, p < 0.001 | χ2 = 116.4, p < 0.001 | χ2 = 126.5, p < 0.001 | p < 0.001 | p < 0.017 |
| Gender | χ2 = 10.6, p = 0.032 | χ2 = 33.1, p < 0.001 | χ2 = 13.0, p = 0.043 | p < 0.001 | p < 0.017 |
| Region | χ2 = 20.5, p < 0.001 | χ2 = 25.3, p < 0.001 | χ2 = 30.7, p < 0.001 | p < 0.001 | p < 0.017 |
| Education of the Head of Household | χ2 = 57.1, p < 0.001 | χ2 = 179.1, p < 0.001 | χ2 = 219.4, p < 0.001 | p < 0.001 | p < 0.017 |
| Guardian Occupation | χ2 = 50.6, p = 0.001 | χ2 = 148.8, p < 0.001 | χ2 = 121.4, p < 0.001 | p < 0.001 | p < 0.017 |
| Region | Often (OR, 95% CI) | Occasionally (OR, 95% CI) | Rarely (OR, 95% CI) | Never (OR, 95% CI) | p-value |
|---|---|---|---|---|---|
| Ha'il | 1.2 (1.0-1.5) | 1.0 (0.9-1.2) | 1.8 (1.4-2.3) | 1.1 (0.9-1.3) | 0.02 |
| Riyadh | 1.3 (1.1-1.6) | 1.1 (0.8-1.4) | 1.5 (1.2-1.9) | 1.0 (0.7-1.3) | 0.03 |
| Makkah | 1.6 (1.3-2.0) | 2.3 (2.0-2.6) | 1.0 (0.8-1.2) | 0.8 (0.5-1.1) | 0.01 |
| Medina | 2.0 (1.5-2.5) | 1.8 (1.4-2.2) | 1.2 (1.0-1.4) | 1.0 (0.8-1.3) | 0.04 |
The application of the Bonferroni correction was crucial in ensuring that these associations were not identified by chance, given the multiple comparisons performed. This adjustment affirms the reliability of the findings, highlighting the strong and consistent relationships between sociodemographic factors and oral health outcomes.
Table 4 depicts how participants from different regions report the frequency of toothaches, categorized as “often,” “occasionally,” “rarely,” and “never.” These associations were investigated using a multinomial logistic regression model. This model helps in comprehending how residing in a certain area affects the probability of falling into one of the response groups as opposed to others. Along with 95% confidence intervals (CIs) to show the accuracy of these estimations, odds ratios (ORs) were provided to measure these possibilities. To make sure the results were statistically credible, Pearson chi-square tests were carried out to verify that the model fits the data well.
In terms of toothache frequency, the findings of the current study demonstrated differences across regions of Saudi Arabia. With an OR of 2.0 (95% CI: 1.5–2.5, p = 0.04) for the “often” category, Medina participants were most likely to experience regular toothaches. Reflecting a noteworthy trend for intermittent toothache complaints, Makkah residents were more likely to report “occasionally” experiencing toothaches (OR = 2.3, 95% CI: 2.0–2.6, p = 0.01). With individuals somewhat more likely to report “often” (OR = 1.3, 95% CI: 1.1–1.6, p = 0.03) and “rarely” (OR = 1.5, 95% CI: 1.2–1.9, p = 0.03), Riyadh exhibited modest relationships. Ha'il, in contrast, demonstrated the strongest association with “rarely” reported toothaches (OR = 1.8, 95% CI: 1.4–2.3, p = 0.02), suggesting infrequent dental issues are more common in this region.
Regarding dental visits, the majority in all regions reported visiting the dentist “once” or “twice,” with Ha'il showing the highest percentage of single visits. Non-visits were reported only in Ha'il, Madinah and Riyadh regions, with a notable proportion in Madinah and Riyadh regions also indicating they “never had dental care.” The primary reason for dental visits was “pain” across all regions, particularly dominant in the Ha'il and Makkah regions, where it accounted for 60% of responses. “Check-ups” were the least cited reason in all regions, while “no visit” responses were significant in the Madinah and Riyadh regions (Fig. 3). These results highlighted key sociodemographic groups, such as children from certain regions or with less-educated guardians, who may be at greater risk of poor oral health outcomes. Identifying such groups allows for the design of targeted public health interventions, such as school-based awareness campaigns, improved parental education programs, and region-specific dental service planning.
4. DISCUSSION
Sociodemographic factors have a major impact on children's oral health outcomes, particularly in terms of toothache prevalence, dental visit frequency, and reasons for seeking care. These outcomes were substantially influenced by sociodemographic factors of age, parental education, family income, and geographic location [1, 2]. These outcomes highlight the importance of sociodemographic factors in shaping and enhancing the oral health of youngsters. On an international level, these connections were extensively investigated by the previous studies; however, the current study filled a void in the literature by offering an understanding of the specific scenario of Saudi children.
According to the current study, 7.0% of children reported having toothaches frequently, whereas 53.5% of children had toothaches occasionally. Dental health problems are common among Saudi children, with research indicating elevated incidences of dental caries and toothache. Three-quarters of children (34.5% of those surveyed) had repeated toothaches, and 62.5% reported not cleaning their teeth every day [15]. A research study in the Ha'il region of Saudi Arabia indicated an 18% incidence of school absenteeism attributable to toothache among secondary school pupils [16].
Maintaining children's oral health requires routine dental visits. According to the current study, 35.1% of participants had two dental appointments in the preceding year, and 13.2% said they had no visits during that time. Studies conducted in Saudi Arabia reveal a lack of adherence to suggested visitation procedures. In Al Madinah, just 9.2% of kids between the ages of 9 and 12 reported going to the dentist on a regular basis [17]. A study on male school children in Saudi Arabia indicated that 56% had missed dental checkups in the past year, while 34.5% had recurrent toothache [15].
Research in Saudi Arabia revealed that children often seek dental consultations later than recommended, with most initial visits occurring between the ages of 3 and 6 years [18, 19]. The principal reasons for initial dental consultations were dental caries, pain, and emergencies [18-20]. The present study revealed that 44.4% of recent dental appointments were attributable to toothache or other oral concerns. Follow-up treatments accounted for 29.8%, whereas routine checkups comprised 8.8%.
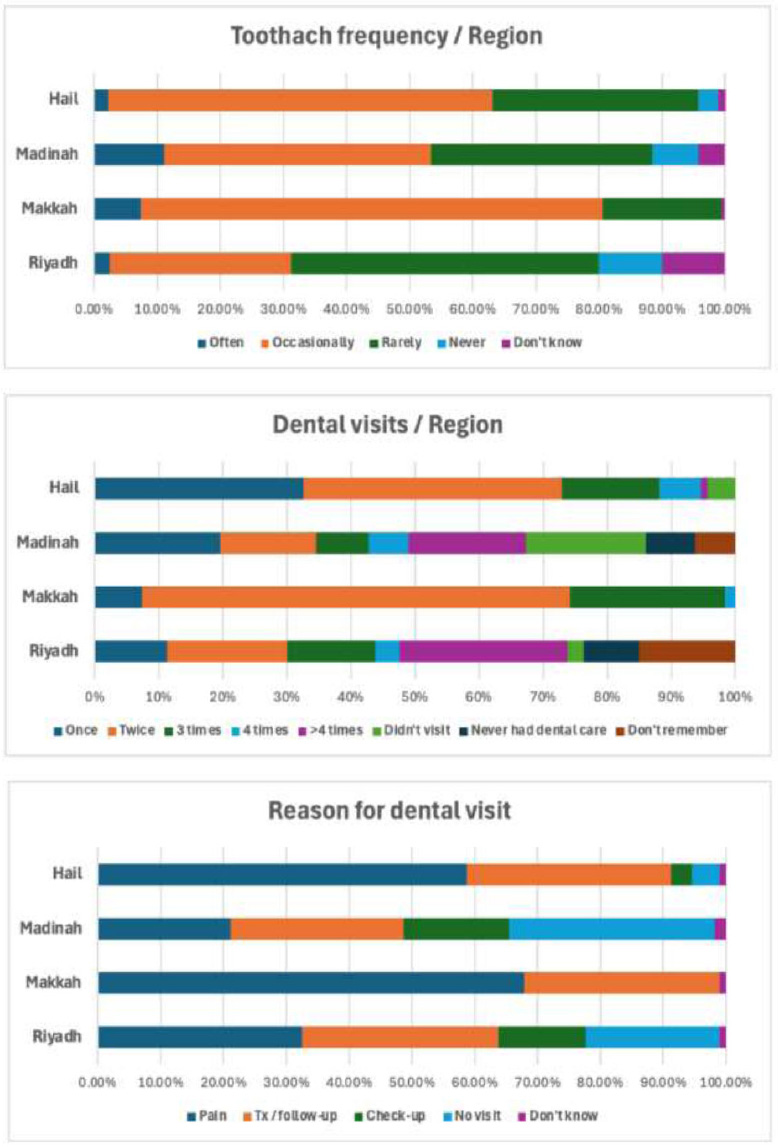
Percentages of distribution of toothache frequency, dental visits, and reason for last dental visits by region.
In the current study, oral health outcomes (tooth frequency, dental visits, and reasons for recent dental visits) showed significant relationships with all sociodemographic variables (age, gender, area, household head's education, and guardian occupation). Only 6.8% of people reported regularly seeing the dentist, indicating that preventative services are still not widely used even with free dental care [21]. Most children wait until they are between the ages of three and six for their first dental appointment [19, 22]. According to research, women are more likely than men to have regular dental checkups [17]. The majority of Saudi female school children (64.1%) went to the dentist in the previous year. Better oral health outcomes and frequent dental visits were positively correlated with greater maternal education, higher family income, daily tooth brushing, no dental pain, and abstaining from soft drinks [23, 24]. Larger families and parents with less education are more likely to face dental care barriers [25]. Despite recommendations from dental academies, parental compliance with early dental visits remains low, with pain being the dominant reason for initial visits [19]. Our findings align with recent studies from Dammam and Madinah that reported similar sociodemographic influences on dental service utilization among school children. This study adds new value by presenting region-specific patterns, especially from underrepresented areas like Ha'il, and provides post-pandemic data that is scarce in the existing literature.
In this study, there were significant variations in self-reported oral health across regions. The findings suggest that regional factors, such as access to care or environmental conditions, may influence how often individuals experience toothaches. Understanding these patterns can help design targeted interventions to improve oral health outcomes in specific areas.
Despite the valuable insights from this study, there are some limitations to consider. Since the data is self-reported, there is a chance that participants may not always recall details accurately or might give answers they think are more socially acceptable. Also, because this is a cross-sectional study, it captures a snapshot in time, making it difficult to conclude for sure whether sociodemographic factors directly influence oral health outcomes. A long-term study would be needed to track these patterns over time and confirm the connections. The study also faced limitations due to the use of convenience sampling and restricted geographic coverage, which may impact the generalizability of the results to other regions or the broader population.
Overall results of the current study underline the necessity of better oral health education for Saudi Arabian parents and children, as well as a greater understanding of the value of early and routine dental checkups. In order to reduce socioeconomic disparities and encourage preventative oral health practices in Saudi Arabia, these findings emphasize the necessity of focused oral health interventions and policies.
CONCLUSION
The current study accentuated the significant influence and impact of sociodemographic factors on the oral health outcomes in children. Age, gender, family occupation and income, parental education, and region were found to be exerting a considerable influence on the toothache prevalence, regularity of dental visits, and motivation for the recent visit to the dentist. Developing context-specific public health strategies for dealing with oral health inequities and improving children’s oral health is absolutely necessary. The patterns observed in the current study draw attention to this need. By motivating regular dental care and the removal of access difficulties, these context-specific public health initiatives can greatly improve the oral health of Saudi Arabian children. Future research should consider longitudinal and intervention-based studies to explore causal relationships and assess the effectiveness of targeted oral health programs in different sociodemographic groups.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: M.A.: Study conception and design; A.A.: Conceptualization; H.A.A.: Data collection; H.D.A., M.A.A., E.A., and A.A.S.: Analysis and interpretation of results; F.O.A.: Visualization; S.S.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| ADHD | = Attention Deficit Hyperactivity Disorder |
| OR | = Odds Ratio |
| CI | = Confidence Interval |
| VIF | = Variance Inflation Factor |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was granted by the Scientific Research Committee of the Deanship of Research at the University of Ha'il, Saudi Arabia, under the approval number H-2023-365.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from parents of the participants of the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available upon reasonable request from the corresponding author [S.S]. It is not deposited in any public repository.
ACKNOWLEDGEMENTS
Declared none.

