All published articles of this journal are available on ScienceDirect.

Maximal Mouth Opening Index among Dental Students in Khartoum University
Authors Info & Affiliations
Abstract
Introduction
This study aimed to determine the maximum mouth opening (MMO) among a group of Sudanese adults. Reduced mouth opening (MO) can lead to difficulties in mastication and social interactions, potentially impacting dental treatment planning. Comparing the MMO values between males and females, relating each subject’s 3-4 finger width to inter-incisal distance was the method used.
Methodology
A total of 277 undergraduate students (179 females and 98 males), aged 18–25 years, participated in the study. MMO was measured as the vertical inter-incisal distance using a digital vernier caliper. Participants were also assessed on the number of fingers they could fit vertically between their incisors, with the normal range defined as 3–4 fingers. The finger width in millimeters was then compared to the previously measured MMO. Additionally, the ratio between MMO and maximum lateral mandibular movements (right and left excursions) was recorded.
Results
The overall mean MMO was 52.64 ± 6.4 mm, with males exhibiting a significantly higher mean MMO (56.33 ± 6.77 mm) compared to females (50.62 ± 5.19 mm). Approximately 69.3% (n=192) of participants could place four fingers vertically between their incisors. A statistically significant difference was found when comparing the mean MMO to the finger width measurements (p < 0.001). The mean lateral excursion was 9.13 mm, and a significant correlation between MMO and lateral excursion was observed, with a ratio of approximately 1:5.6
Discussion
The mean MMO was 52.6 mm, higher than most previous studies, possibly due to ethnic and physical differences. Males showed greater MMO than females, likely due to larger mandibular size, although females may have relatively greater joint mobility. Most subjects could insert four fingers vertically between their incisors, unlike other populations, reflecting higher MMO in this group. Lateral mandibular movement averaged 9.13 mm, consistent with other studies, and a weak positive correlation was found between vertical and lateral mouth movements, especially in males.
Conclusion
The mean MMO in this Sudanese adult population was 52.64 mm, with males demonstrating significantly greater mouth opening than females. Most participants (69.3%) could accommodate four fingers inter-incisally. The ratio of MMO to lateral excursion was higher than previously reported in the literature, suggesting potential population-specific variations.
1. INTRODUCTION
Maximum mouth opening (MMO) is expressed as the greatest distance between the incisal edge of the maxillary central incisors to the incisal edge of the mandibular central incisors at the midline [1], or as corrected inter-incisal distance by adding the amount of vertical overlap between the upper and lower incisors [2]. The range of mouth opening plays a significant role in the diagnosis of many clinical conditions and can have implications for the management and treatment of patients. Early detection of decreased or limited mouth opening is necessary for a prompt and efficient approach to diagnosis and to plan out the treatment options judiciously [3]
In order to make a diagnosis of decreased mouth opening, it is essential to establish what constitutes the normal opening for the population [4] since MMO among different populations has been reported to vary considerably, and its range is specific for a given population [3]. Studies have found significant correlations between MMO and body size parameters such as height and weight. Regression equations have been proposed to estimate MMO based on these factors, especially in young adults [2, 5-8]. In addition, a significant relation between the mouth opening and other body measurements such as the patient’s own 3 or 4 finger widths, the mandibular length, and lateral excursions was found [9-11].
there is limited data on MMO values among Sudanese, a population that may have specific anatomical and functional characteristics. Establishing baseline MMO values can aid in early detection of TMJ disorders and guide clinical care.
This study is an attempt to establish the normal range of mouth opening among a group of healthy Sudanese dental students without known TMJ disorders, orofacial pain, and correlate it to the finger width of the same person.
2. MATERIALS AND METHODS
This is a descriptive analytical cross-sectional study that was conducted on Sudanese undergraduate students (1st to 5th year) in the Faculty of Dentistry - University of Khartoum. The manuscript has been developed in accordance with the SAGER (Sex and Gender Equity in Research) guidelines.
2.1. The Sample Size
277 students (98 males and 179 females). All undergraduate students (1st to 5th year) were included in the study if they agreed to participate and satisfied the following criteria.
2.2. Method for Measuring the Mouth Opening
For measuring the MMO, a digital caliper (Vernier) was used (Fig. 1), each participant was asked to get seated; with the head in a resting position, before the inter incisal distance was measured, in frontal vision.
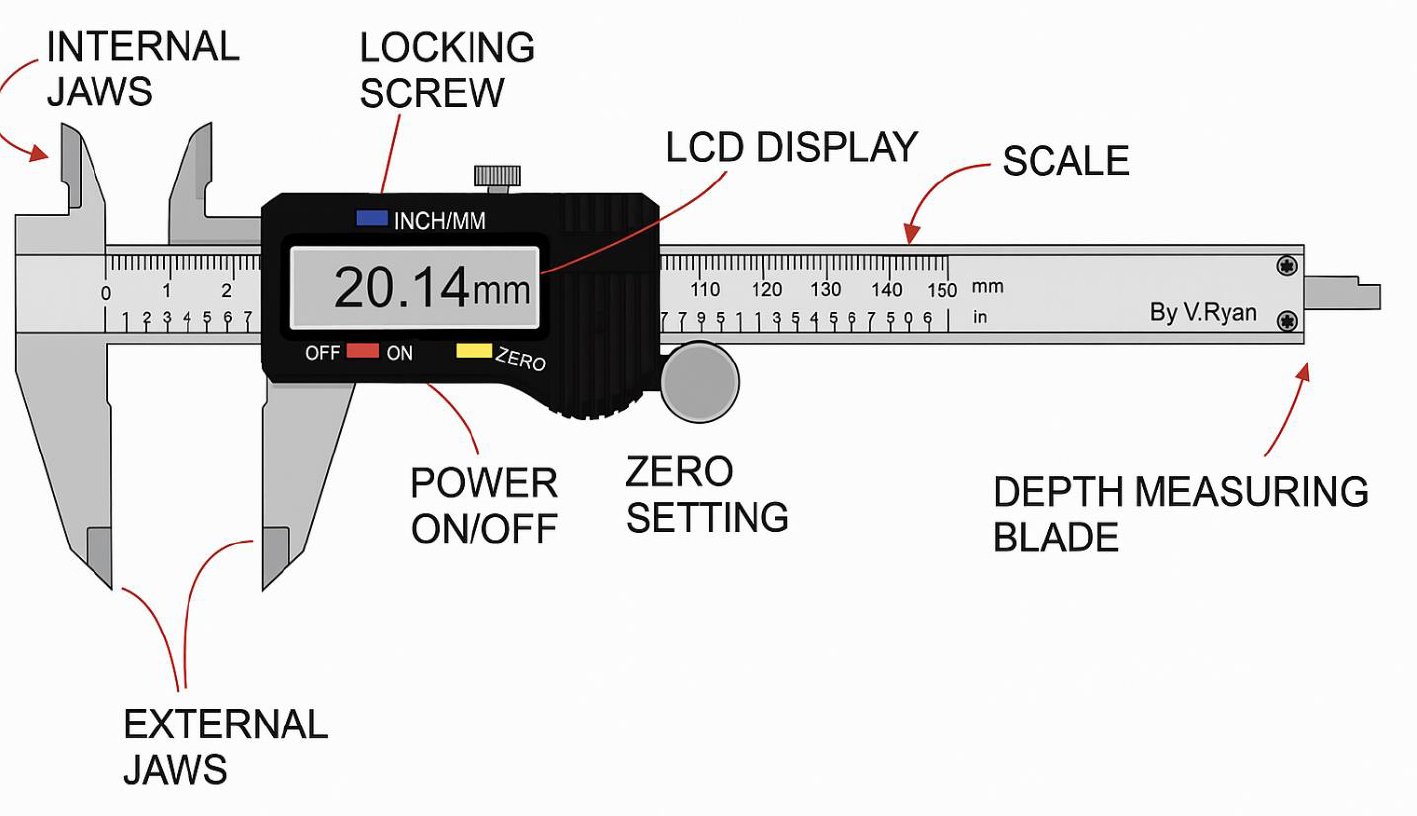
An illustrated drawing of a vernier.
The subject was then asked to open his/ her mouth wide until no further opening was possible. After verification of the zero reading, the inside-measuring jaws of the Vernier were placed into the inter incisal space and were slid apart until they contacted the opposing incisal edges. The measurement was then read and recorded in millimeters with two decimal digits. For each subject, the measurement was taken twice and, afterwards, the average was calculated. Finally, the caliper jaws were wiped and disinfected with ethyl alcohol and rubbed with cotton (Fig. 2).

Mouth opening measuring by using a vernier.
2.3. The Three or Four Fingers Method
The participant was asked to open his/her mouth as wide as possible again and try to position his /her fingers vertically aligned. The ability to position the fingers, vertically aligned, between the upper and lower central incisors up to the first distal inter phalangeal folds was documented. For the 3-finger assessment, the index, middle, and ring fingers were used. For the 4-finger assessment, the little finger was added. The width of 3 or 4 fingers was then measured by the vernier measured (Fig. 3).
For measuring the lateral movement, demarcation of two reference points, using a non-toxic pencil on the labial surface of the central maxillary and mandibular incisors, with the teeth in edge-to-edge occlusion, was performed. This reference point was used for measurement of the range of motion during mandibular excursion. The subject was asked to open slightly (physiological rest position) and move the mandible as far as possible toward the right as in (Fig. 4a) then return to the reference point at rest position (Fig. 4b) lastly move the mandible as far as possible toward the left (Fig. 4c). the measurement was done by a millimeter ruler and digital caliper between the two reference points.
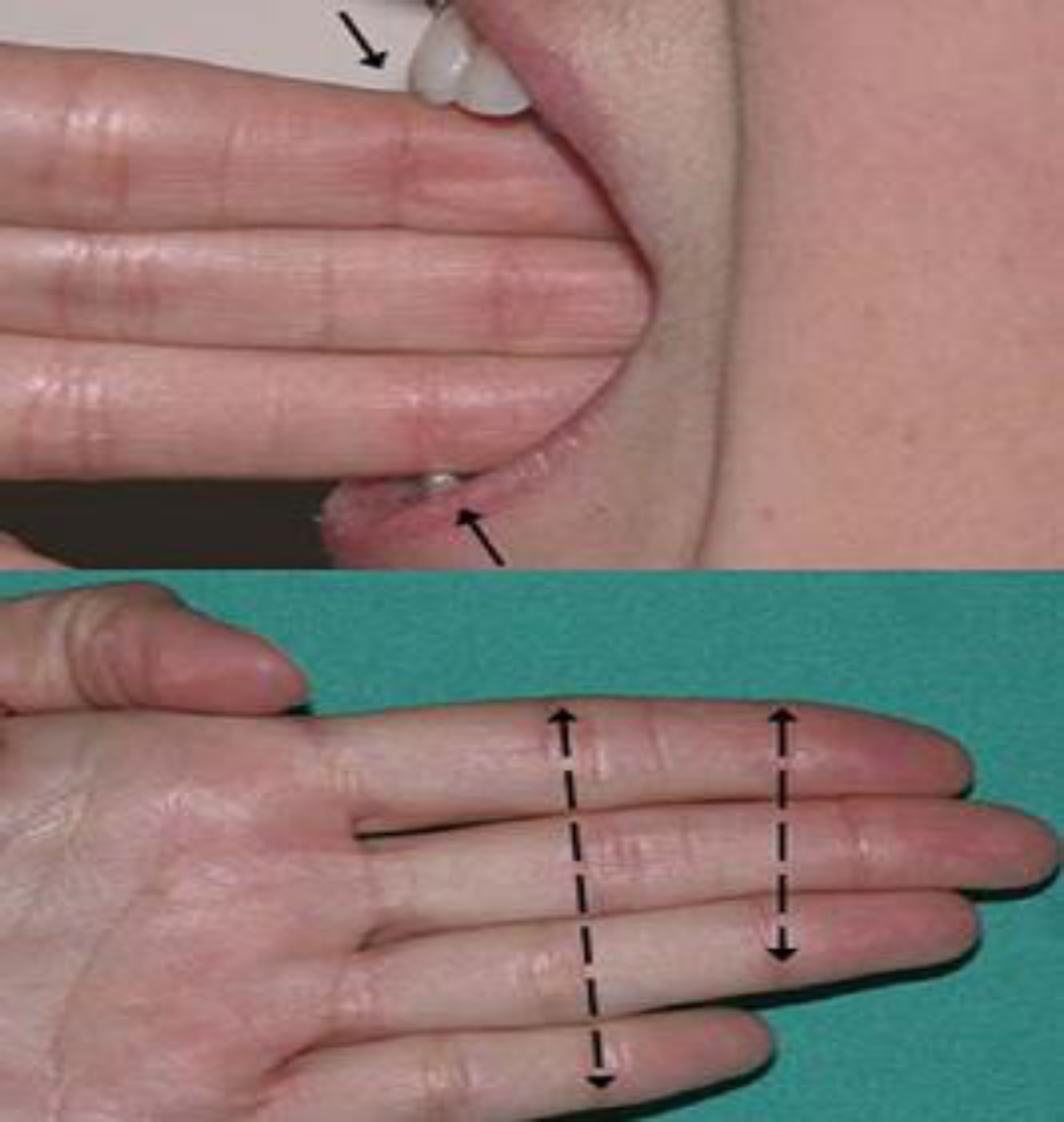
Mouth opening measuring by using 3 and 4 digits method.
The examination and measurements were performed while the subject was seated comfortably in the dental chair in an upright position. The time of evaluation was kept consistent (between 9 am and noon).
To ensure measurement reliability, the examination was repeated for 10% of the study participants by the same examiner after 1 week then Kappa test was performed to investigate intra-examiner reliability. 10%-20% variation was considered as an acceptable range.
Data has been collected over a period of three months by means of color-coded examination sheets for gender differentiation and ease of extraction. White colored examination sheets were assigned for male subjects, while light blue was assigned for female subjects (Appendix 1). An excel document was utilized for data entry and extraction.
All participants had been informed about the purpose of the study, and a written consent was signed (Appendix 2).
2.4. Statistical Analysis
The data were imputed and analyzed by using SPSS version 22.
Data was analyzed Gender based, comparison of parameters was conducted using the student t-test, correlation coefficients were determined between the mouth opening and fingers measurement, for all tests, a p <0.001 will be considered significant.

Shows measurment of lateral excursion. (a). Measurment of right lateral excursion from midline. (b). Midline. (c). Measuement of left lateral excursion from midline.
3. RESULTS
Most participants were females with a total of 277 (179 female/98 male). Students between the ages of 18-25 with a response rate of 98% where 5 students from those who are fulfilling the inclusion and exclusion criteria refused to participate in the study (Table 1).
The mean maximum mouth opening among the population was 52.6±6.4 mm, the largest mouth opening recorded was 70mm, while the smallest was 40mm. According to gender, the mean mouth opening in males was 56.33 ± 6.77 (43 – 70 mm). In females, the mean was 50.62±5.19 mm with the range of (40- 67mm) (Table 2).
The results showed a significant difference between males and females regarding maximum mouth opening when tested with an independent student’s T-test, males have a higher mouth opening when compared to females. Most of our study participants, 192(69.3%) were able to place 4 fingers vertically aligned, between the upper and lower central incisors up to the first distal interphalangeal folds. While only 85 (30.7%) were able to place 3 fingers vertically aligned.
Two-thirds of males, 62 (63.3%) were able to place 4 fingers, and only 36 (36.7%) could place 3 fingers, while in females, almost three quarters130 (72.6%) were able to place four fingers and 49(27.4%) were 3 fingers (Table 3). By performing chi chi-squared test, p= 0.106, the p-value was not significant which means that there is no correlation between the number of fingers and the gender of the participant statistically.
When fingers were measured in mm, the mean was found to be 50.35±6.3 mm with the range of (38-72 mm).
| Gender | Frequency | Percentage |
| Male | 98 | 36.4 |
| Female | 179 | 64.6 |
| Total | 277 | 100 |
| - | Mean/mm | Standard Deviation | Minimum/mm | Maximum/mm |
| Population | 52.64 | 6.4 | 40 | 70 |
| Male | 56.33 | 6.77 | 43 | 70 |
| Female | 50.6 | 5.19 | 40 | 67 |
| - | Three Fingers | Four Fingers | Total |
| Males | 36 | 62 | 98 |
| 36.7% | 63.3% | 100% | |
| Females | 49 | 130 | 179 |
| 27.4% | 72.6% | 100% | |
| Total | 85 | 192 | 277 |
| 30.7% | 69.3% | 100% |
| - | Gender | Number | Mean | SD | p-value |
| Three fingers | Male | 36 | 50.17 | 6.84 | 0.001 |
| Females | 49 | 45.71 | 3.8 | ||
| Total | 85 | 47.59 | - | ||
| Four fingers | Males | 62 | 55.62 | 5.85 | 0.001 |
| Females | 130 | 49.65 | 5.47 | ||
| Total | 192 | 51.58 | - |
| Gender | - | Number | Mean | SD | Correlation | p-value |
| Male | MMO | 98 | 56.33 | 6.77 | 0.854 | 0.001 |
| Fingers in mm | 98 | 53.61 | 6.74 | |||
| Females | MMO | 179 | 50.62 | 5.19 | 0.791 | 0.001 |
| Fingers in mm | 179 | 48.57 | 5.35 |
| - | Mean | SD | 95% Confidence Interval of the Difference | p-value | |
| - | - | - | Lower | Upper | - |
| Male | 2.71 | 3.65 | 1.98 | 3.45 | 0.001 |
| Female | 2.05 | 3.41 | 1.55 | 2.56 | 0.001 |
In males, the mean of finger measure was found to be in general 53.61±6.8 mm. Males who were able to place 3 fingers, the mean was 50.17mm, and those who were able to place four fingers, the mean was 55.62mm. In females, the general mean finger measurement was 48.57±5.35mm. For females who were able to place 3 fingers, the mean was 45.71mm, and in those who were able to place 4 fingers, it was 49.65mm (Table 4). The results showed a significant correlation (p-value=0.001) between MMO measured clinically and MMO recorded indirectly through fingers measuring in both males and females, Pearson’s correlation = 0.854 and 0.791 respectively (Table 5). The finger measurement was slightly lower than the clinical MMO, the mean difference between the two measurements was slightly higher in males (2.7 ± 3.67) when compared to females (2.05 ± 3.41) (Table 6). There was a significant difference in the level of 0.001 when the T-test compared the mean of maximum mouth opening and the mean of finger measurement in mm, since the MMO was always higher than the finger measurement. This phenomenon was significant in both genders, it was slightly higher in males (2.7±3.65) when compared to females (2.05±3.41) (Table 6).
The right and left lateral excursions were measured, and the mean of both was correlated to the maximal mouth opening.
In general, the maximum right lateral excursion was 14.6mm and the minimum was 3mm, with a mean of 9.29±2.13mm. The maximum left lateral excursion was 15 mm, and the minimum was 4.4mm, with a mean of 8.98±1.91. The mean for the left and right lateral excursion was 9.13±1.77mm. In males the mean between right and left was 9.29 ± 1.89, and in females it was 9.05± 1.7mm (Table 7).
| - | - | Mean | SD | Minimum | Maximum |
| General | Right lateral excursion | 9.29 | 2.13 | 3 | 14.6 |
| Left lateral excursion | 8.98 | 1.91 | 4.4 | 15 | |
| Mean of right & left | 9.13 | 1.77 | 0 | 15 | |
| Male | Right lateral excursion | 9.52 | 2.4 | 3 | 14.6 |
| Left lateral excursion | 9.05 | 1.95 | 5.1 | 12.8 | |
| Mean of right & left | 9.29 | 1.89 | 5 | 13 | |
| Female | Right lateral excursion | 9.16 | 1.96 | 5.2 | 14.2 |
| Left lateral excursion | 8.94 | 1.89 | 4.4 | 15 | |
| Mean of right & left | 9.05 | 1.69 | 5 | 15 |
| - | Person Correlation | p-value | Comment |
| General population | 0.199 | 0.001 | Significant |
| Male | 0.214 | 0.034 | Significant |
| Female | 0.172 | 0.021 | Significant |
| - | Number | Mean | SD |
| General | 277 | 0.178 | 0.04 |
| Male | 98 | 0.184 | 0.038 |
| Female | 179 | 0.175 | 0.036 |
A weak positive correlation exists between the maximum mouth opening and the lateral excursion in general, where person correlation was 0.199 with a significant p-value of 0.001. This was prominent in males compared to females (Table 8).
The ratio of the maximum mouth opening to the lateral excursion was (1:5.62). According to gender, the ratio was (1:5.43) and (1:5.71) in males and females respectively (Table 9).
4. DISCUSSION
The inter-incisal distance during active opening (that achieved by the patient without assistance) was used in this study, as in most previous studies, to determine the maximum mouth opening measurement, with the advantage that the measuring point is relatively more permanent and more easily determined. Although other investigators found passive mouth opening to be greater but Dijkstra et al stated that errors can occur due to variable forces applied [12].
In the current study, assessment of mouth opening was accomplished by measuring the inter incisal distance with a digital caliper when a patient opened actively (without assistance).
Several methods of extra oral measurement of mouth opening were described in previous studies, including angle of mouth measurements [12], cephalometric radiographs [13] and the use of instruments such as the Mandibular Excursiometer [14]. These are often costly and require special apparatus. On the other hand, many different instruments, such as rulers, dividers, Willis Bite Gauge, and Alma bite gauge, have been used to measure linear mouth opening [15]. Wood and Branco compared direct and extra oral measurements and concluded that direct measurements using a ruler were more precise and accurate [16].
The advantages of the digital caliper used in the current study are based on accuracy as well as ease of operation and reading.
Inter-incisal distance plus overbite is thought to be a more accurate reflection of the vertical distance travelled by the mandible [3] and was used by some researchers [10] However, what is clinically important is the functional opening of the mouth, which is the inter-incisal distance without the overbite that allows normal social function for the patient and adequate access to the oral cavity for clinicians, and not the vertical distance traveled by the mandible.
The mandible moves around the temporomandibular joints TMJs, which act as bilateral hinges.
This anatomical structure affects the movement of the mandible during opening and closing. It will follow a curved arcing path rather than a simple linear one. The MMO interincisal distance, typically recorded a straight-line distance between the edges of the upper and lower central incisors. While this provides a convenient and reproducible measure, it does not capture the true trajectory of mandibular movement. As a result, linear measurements may underestimate or oversimplify the functional range of motion.
Due to the wide range of mouth opening among the population and even within the same population correlation between the amount of vertical mouth opening and the width of three or four fingers proposed by Zawawi et al. [9], also a correlation between the amount of vertical mouth opening to the amount of right and left lateral mandibular movement was suggested by Hochstedler et al [11].
In the current study, two measurements were made per case, and the mean of the two values was recorded. Previous studies using the inter-incisal distance for the determination of MMO, have taken an average of two or three successive measurements and have found the last measurement to be the largest [17]. However, Agerberg found that mouth opening decreased with repetition. This might have been caused by decreasing muscle power with succeeding measurements [2].
To avoid the bias due to inaccurate determination of mouth opening, proper selection of subjects was confirmed. Accuracy of inter- incisal distance was maintained if subjects had their own anterior teeth, but difficulties arise when incisors are absent, traumatized, restored, or incompletely erupted, as mentioned in the previous study [3]. Moreover, exclusion criteria comprised subjects with TMJ problems in addition to those with previous or current orthodontic treatment, in order not to alter the accuracy of the results.
In the current study, the mean measurement for the Sudanese population mouth opening was found to be 52.6 mm (males 56.3mm, females 50.6mm), although this finding is considered high in relation to most studies [3, 6, 18] but other studies found similar measurements for the same age group [19-21]. Although differences among samples and measuring methods cannot be excluded, variations like race and stature among populations can also explain this difference and support the hypothesis that each population has a specific mandibular range of motion.
A consistent finding across studies is the significant difference between males and females [3, 20, 22]. A fact that was also portrayed by the results of this study. The values of MMO depend on the size of the mandible, which is significantly greater in males than in females [23]. This is likely due to the physical size; males are generally larger than females, so the head and face bone structures are accordingly bigger, hence it is conceivable that MMO would be larger in males. However, it has been reported that joint mobility in general is greater in females than in males gender [3]. The angle of the mandible was studied by Pullinger et al. [24], and found that it increased in women. This finding aligns with the general observation that women tend to have greater joint laxity. Pullinger et al. further supported this by demonstrating that, even after adjusting mouth opening measurements for height and body weight, women still exhibited a greater range of mouth opening relative to their size, although their average absolute mouth opening remained lower than that of men [24].
Other studies reported that the influence that gender has on MMO in adults is not observed in children because they do not have the sexual maturity of adults [25].
According to previous studies, mouth opening was greatest in the age range of 16-24 [3] and it will decrease after that, so our study was confined to this age group to find the maximal mouth opening among Sudanese population the explanation for that is the end of the human growth period and the aging process will start after this age leading to degenerative and osseous changes in the condylar head and mandibular fossa [18].
Ethnicity significantly influences the range of maximum mouth opening (MMO). Studies among Nigerian, Indian, and Albanian groups showed statistically significant and notable variations between different ethnic groups that persisted even when controlling for other factors such as age, height, and weight, which themselves also correlate with MMO [5, 26, 27].
In contrast to most studies which found that the majority of their population are able to place 3 fingers vertically aligned interincisally, two studies supported our results and found that only 8.6%, 36.3% of the study group were able to place 4 fingers [9, 17].
Concerns were raised by chima [21] that a good number of their sample were able to insert more than three fingers conveniently into the mouth .these concerns will be justified in pathological conditions of the temporo-mandibular joints, infections and maxillofacial tumours associated with slow progressive limitation of mouth opening, there may be a delay in diagnosis if three finger breadth measurement is used in a patient capable of inserting more than three fingers comfortably into the mouth. In our study, this is not the case; most subjects were able to place 4 fingers regardless of gender, and this might be due to the first finding that the examined subjects had a higher mouth opening than found in most literature.
Lateral movements of less than 8 mm are considered restricted [23, 28]. This study gave an average value of 9.13 mm for the lateral movements in general and 8.9 to 9.3 mm on the left and right sides respectively. These results are in accordance with studies where the mean lateral movements range from 8.7 to 11.1mm for the lateral movements [2, 28]. The ratio between the vertical mouth opening amount and the amount of right and left lateral movement was higher than that found by Hochstedler et al. [11], there was a positive week relationship that was more obvious in males than in females. Studies in this area were limited and need more investigation.
CONCLUSION
The average MMO in the Sudanese population was 52.64 mm, which is notably higher than values reported in Caucasian and Asian populations. This suggests potential ethnic or regional variations in oral physiology. Males demonstrated significantly greater MMO compared to females in the 18–25-year age group, highlighting gender as an important factor influencing mouth opening capacity.
A majority (69.3%) of participants were able to place four fingers inter-incisally, indicating a consistent and practical clinical measure of MMO within this population. The ratio between MMO and lateral excursion was higher than previously recorded, suggesting unique mandibular movement characteristics in the studied group.
STRENGTHS
- The study provides valuable normative data on MMO and lateral excursion specific to the Sudanese population, filling a gap in the literature.
- Inclusion of gender-based analysis offers insight into physiological differences within the population.
- Use of simple clinical measures (finger placement) enhances the practical applicability of findings.
LIMITATIONS AND RECOMMENDATIONS
- The sample size and demographic scope were limited; thus, results may not be fully generalizable to the entire Sudanese population.
- Comparative studies involving diverse ethnic groups could further elucidate the observed differences in MMO and mandibular movements.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: M.S.A.: Study concept or design; S.A.A.: Data collection and writing the paper; A.N.: Data analysis or interpretation; S.A.: Contributed to writing the paper: SA. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MMO | = Maximum Mouth Opening |
| MO | = Mouth Opening |
| TMJs | = Temporomandibular Joints |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical committee of the research board of the faculty of dentistry University of Khartoum, Sudan approved the research on 14/9/2015.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Participant agreement was obtained via filling in informed consent after explaining the research title and purpose in clear, simple words. Only data that is relevant to the study purpose was extracted, and confidentiality was maintained.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [M.S.A] upon reasonable request.
FUNDING
The work was conducted as a part of the MSc education program at Khartoum University dental college, and no grants or financial support were received.
ACKNOWLEDGEMENTS
Declared none.
APPENDIX 1
Examination Sheet
Date____________
Age_____________
Gander: Male
 Female
Female
Do you agree to participate in this research?
Yes
No
Examination:
Class ɪ
Class ɪɪ
Class III
Mouth opening measurement:
MMO digital measurement: _____________mm
Finger measurement:
3 fingers
4 fingers
Finger width measurement _________________mm
Lateral movement: Right ____mm Left ____mm
APPENDIX 2
Consent Form
University of Khartoum
Faculty of dentistry
Department of oral rehabilitation
Conservative dentistry
Dear student:
In research named”Maximal Mouth Opening Index among Dental Students of Khartoum University”
Your participation is highly evaluated and appreciated as a serve for your community by establishing a base line for feather investigations
Your consent is required to include you in the research, Clinical examination will be carried out. All information will be confidential.
Dr. Samar Amin Elsayed
I …………………………………………………………….
Agree to participate in the above-mentioned research.
Signature …………………
Date …………………………

