All published articles of this journal are available on ScienceDirect.

Rare Variation of the Canalis Sinuosus Mimicking an Aberrant Position of Incisive Canal: A Case Report
Authors Info & Affiliations
Abstract
Introduction
For the rehabilitation of the edentulous anterior maxilla, implant surgeons need to take precautions regarding the nasopalatine canal and its contents. However, another important anatomical structure in this area, i.e., the canalis sinuosus, can sometimes be easily overlooked.
Case Presentation
In this case report, a well-corticated, small radiolucency was noted adjacent to the palatal aspect of the alveolar process in an edentulous area. Initially, it was hypothesized that the nasopalatine canal was positioned laterally due to aberrant embryonic development. Image manipulation of the Cone Beam Computed Tomography (CBCT) scan revealed that the structure was indeed canalis sinuosus.
Conclusion
CBCT technology can offer the implant surgeon not only the chance of increased accuracy but also the avoidance of surgical and restorative complications. However, implant surgeons need to be aware of identifying key anatomical canals and foramen variations during implant planning. In addition, surgery for the placement of dental implants in the anterior maxilla is often complicated due to biomechanical, phonetic, and aesthetic requirements. Therefore, there is a need to make practical adjustments when anatomical limitations exist in the anterior maxilla. Hence, CBCT scans are mandatory before any implant placements, as any interference with the canal may cause non-osseointegration of the implant, sensory dysfunction, and even haemorrhage.
1. INTRODUCTION
With the growing need for rehabilitation of the edentulous anterior maxilla, the anatomy of this region has become increasingly important, especially in implant procedures where the dental implant may interfere with the nasopalatine (incisive) canal and its contents. It is further reported that more care must be taken with females and younger patients during immediate implant placement (at the mid-root level of the maxillary central incisor) due to the proximity of the root to this canal [1]. Therefore, it is essential to evaluate and consider the presence of the incisive canal and its morphology (size and shape) prior to surgical procedures to prevent any complications [2]. Any interference with the canal may actually cause non-osseointegration of the implant or lead to sensory dysfunction [3]. In recent times, the availability of cone-beam computed tomography (CBCT) has enabled the in-depth analysis of any variability in the incisive canal of the anterior maxilla. However, another important anatomical structure, namely the “canalis sinuosus,” can sometimes be easily overlooked when the practitioner concentrates only on the variations of the nasopalatine canal. The canalis sinuosus is a small canal that carries the anterior superior alveolar nerve and opens near the maxillary anterior teeth [4, 5]. The neurovascular bundle supplies the maxillary central incisors, lateral incisors, canines, and surrounding soft tissue with innervation and vascularity [6]. The terminal portion of the canal sinuosus frequently gives rise to accessory intra-osseous canals. These accessory canals terminate in various anatomical locations, most commonly the anterior palate region of the maxilla [7].
2. CASE PRESENTATION
A 41-year-old male patient visited the dental clinic to replace a missing maxillary left lateral incisor (FDI notation 22). Following tooth extraction, the maxillary alveolar buccolabial wall was undergoing resorption (Fig. 1). He expressed interest in having an implant placed at the edentulous site. A policy followed at the faculty is that written patient consent is always obtained prior to any surgical treatment, which also includes imaging procedures. A CBCT examination was performed using the Vatech Green X machine (Hwaseong-si, Gyeonggi-do, Korea) with a 16 x 9 cm field of view and a 0.2 mm voxel size to assess the bone quality and quantity for placement of a dental implant in the anterior maxilla region.
On axial imaging, a well-corticated, small radiolucency was noticed adjacent to the palatal aspect of the alveolar process in the edentulous area (Fig. 2). This mimicked a smaller version of the nasopalatine canal. It was hypothesized that the possibility of the nasopalatine canal in the lateral position was due to some aberrant embryonic development. However, on reviewing axial slices in a superior direction, the actual incisive foramen was noticed in the centre of the anterior maxilla. The shape and location of the nasopalatine canal appeared normal while the small radiolucency showed early signs of cortication loss (Fig. 3). When the sagittal slice was viewed, an actual canal with somewhat less distinctive margins was noticed (Fig. 4). On scrolling upwards, the canal was observed along the medial wall of the maxillary sinus, terminating at its anteromedial margin. At this stage, the right canalis sinuosus was also evident in the same location as the left canal (Fig. 5).

The transparent volume rendering of the anterior maxilla showing the missing maxillary left lateral incisor and labiolingual bone resorption in the corresponding area.

A well-corticated, small radiolucency was noticed adjacent to the palatal alveolar bone in the left incisor region on the axial view.

The incisive canal is noticed in the centre of the maxilla, while the canalis sinuosus is on the lateral side.
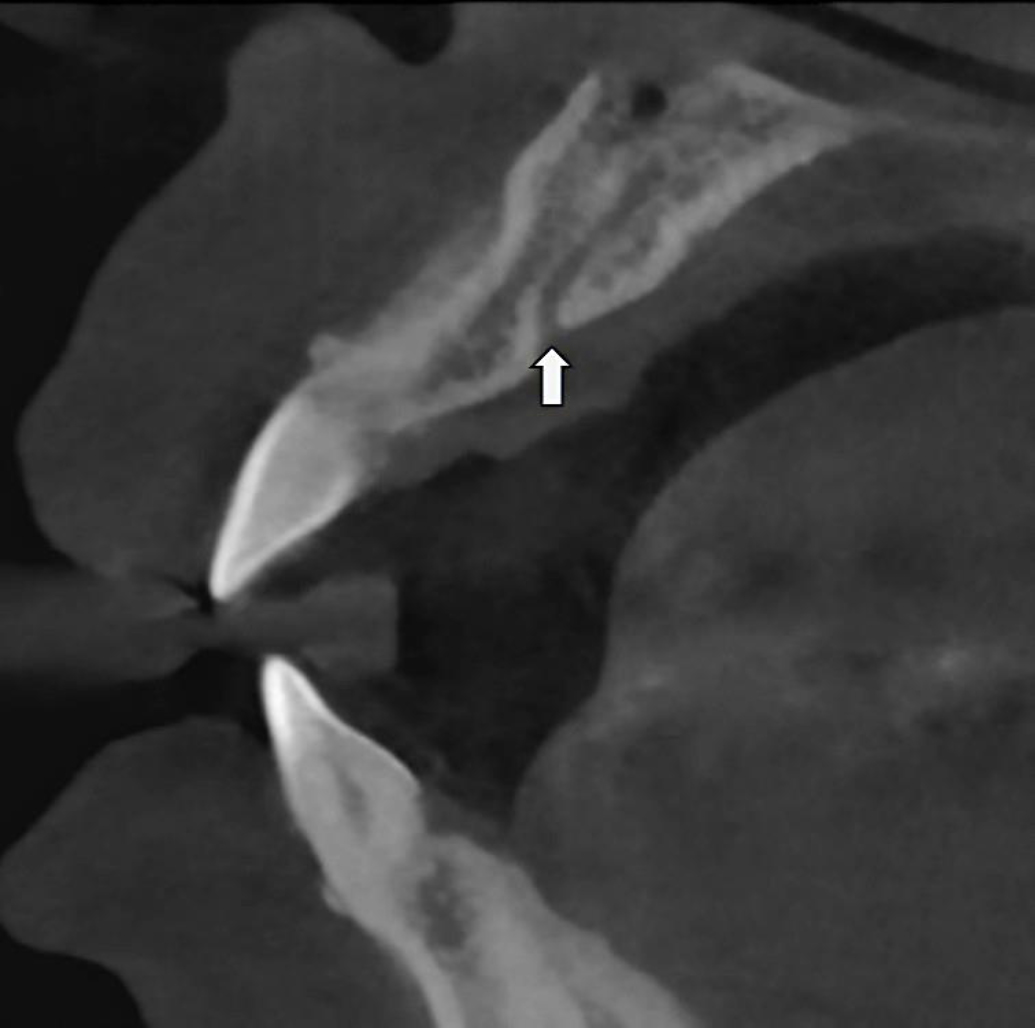
Sagittal CBCT slice showing the presence of canalis sinuosus in the left side of the anterior maxilla.
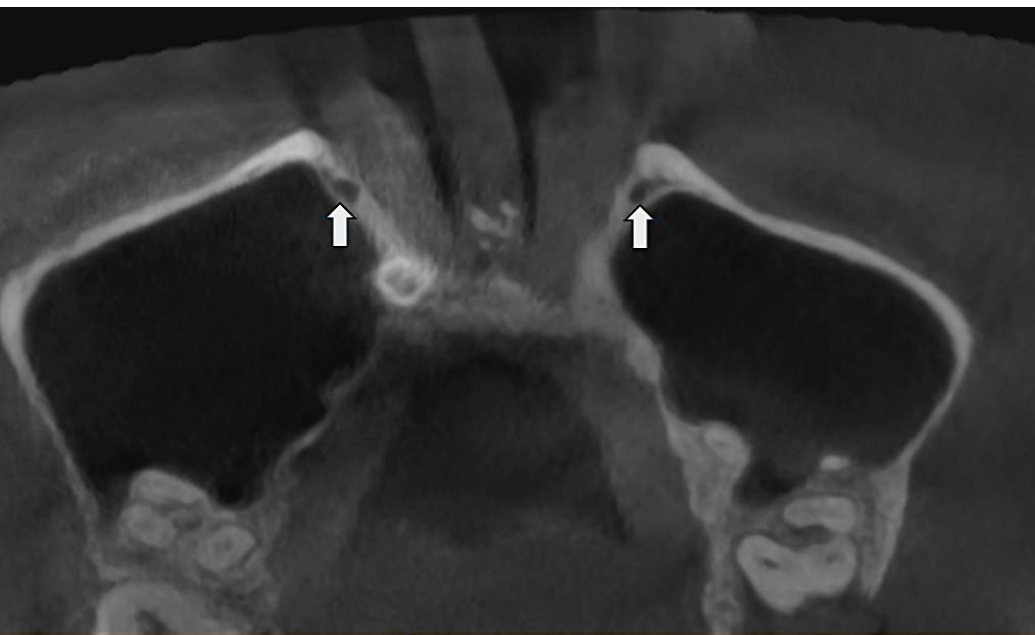
The canalis sinuosus was noticed along the anteromedial margin of the maxillary sinus bilaterally.
3. DISCUSSION
The infraorbital nerve is a branch of the maxillary nerve, which is the second division of the trigeminal nerve. This infraorbital nerve supplies the skin and midface mucosa. When it emerges on the face through the infraorbital foramen, the infraorbital nerve is divided into three alveolar anterior branches (anterior, middle, and posterior superior alveolar nerves) and four distal branches (inferior palpebral, external nasal, internal nasal, and superior labial) [4, 8]. The passage of the anterior superior alveolar nerve is through a small neurovascular canal. This small canal, called the canalis sinuosus, runs forward and downward to the inferior wall of the orbit [5, 9]. The name ” canalis sinuosus” was introduced by Frederic Wood Jones in 1939 to describe a double-curved bony canal arising from the lateral aspect of the infraorbital canal [9]. Subsequently, it proceeds along the nasal margin, giving off neurovascular branches and forming a dental plexus in the alveolus, which supplies the anterior teeth. The branches of the anterior superior alveolar nerve and artery also supply the nasal septum via the foramen septale [10, 11]. It has been reported that canalis sinuosus can appear unilateral or bilateral, most frequently in the regions of central incisor, followed by lateral incisor, and sometimes even in the canine region [9].
Neurosensory disturbance and haemorrhage have been reported during dental implant placement, and canals are said to be a frequent occurrence in the anterior region of the maxilla [12-15]. The nasopalatine duct may migrate and become so superficial that its contents emerge from the edentulous ridge [10]. This was evident in the present case, where the canalis sinuosus was noticed in the edentulous space, mimicking an aberrant position of the nasopalatine canal (Fig. 2). Additionally, the nasopalatine canal tends to enlarge in all dimensions after tooth extraction, and this is believed to progress with age [1]. A similar phenomenon could occur in the canalis sinuosus, particularly when it is located in an edentulous area.
CONCLUSION
CBCT technology can offer the implant surgeon not only the chance of increased accuracy but also the avoidance of surgical and restorative complications [16]. CBCT provides precise details of the studied region and eliminates overlapping images. In addition to collecting reliable linear and angular measurements, it enables the reconstruction of scanned images in multiple planes and in three dimensions [17]. However, implant surgeons need to be aware of identifying canals and foramen variations during implant planning. In addition, surgery for the placement of dental implants in the anterior maxilla is often complicated due to biomechanical, phonetic, and aesthetic requirements [5]. Therefore, adjustments are necessary when anatomical limitations exist in the anterior maxilla. Any iatrogenic damage to the canalis sinuosus can lead to unpredictable complications, such as postoperative pain, paresthesias, and haemorrhage that can only be resolved by removal of the implant, making the treatment a failure [18].
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.H.J.: Study conception and design; P.H., N.P.R., and P.N.: Writing the paper; A.R.K.: Writing the original draft preparation; M.K.A.: Investigation. All authors reviewed the results and approved the final version of the manuscript.
ABBREVIATION
| CBCT | = Cone Beam Computed Tomography |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [P.N] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

