All published articles of this journal are available on ScienceDirect.

The Impact of Different Access Cavity Designs on the Retreatment Procedure of Single Oval Canals Using Reciprocating File Systems: An Ex-Vivo Study
Authors Info & Affiliations
Abstract
Introduction
This study aimed to compare the efficacy of the reciprocating system for the retreatment procedure of root canals obturated with two different sealers, through two different access designs.
Methods
A total of 40 extracted human mandibular premolars with single oval canals were selected. The samples were divided into two groups (n = 20): Group I, which had an endodontic access cavity (CEC), and Group II, which had a traditional endodontic access cavity (TEC). The samples were divided into subgroups (n = 10) according to the following sealers: Bioceramic, AH, and Saler. Retreatment was performed using the Reciproc system. Teeth were scanned with CBCT, and the percentage of residual filling was calculated. The time needed for retreatment was recorded. The ANOVA test was used for statistical analysis.
Results
A significant difference was observed in retreatment times, with the contracted access combined with the bioceramic (BC) sealer requiring the longest time. Overall, no significant difference was found in the amount of remaining obturating material among the four groups. However, when using contracted access and the BC sealer, a significant difference was noted among the root thirds, with the coronal third showing the highest volume of residual material.
Discussion
The reciprocating retreatment system was not effective in completely cleaning the canals, regardless of the access cavity design or the type of sealer used. One limitation of this study is the use of CBCT; more accurate results might have been obtained with the use of micro-CT.
Conclusions
The contracted access combined with the bioceramic (BC) sealer required the longest retreatment time. Residual obturating material was observed in all groups. The contracted access/BC sealer group exhibited the highest amount of remaining material in the coronal third.
1. INTRODUCTION
The primary objective of retreatment for an endodontically treated tooth is to eliminate persistent microorganisms and/or cure apical periodontitis, hence providing an optimal environment for recovery [1]. The removal of root canal filling would improve the disinfection of the root canal system, followed by three-dimensional root canal obturation [2]. Orthograde retreatment of endodontically treated teeth is considered one of the applicable treatment solutions in cases of post-treatment diseases, based on the good outcome results concluded in the literature [3].
The mechanical removal of gutta-percha is often conducted utilizing several techniques and materials, including hand files, rotary tools, ultrasonic tips, or heating equipment, with or without the application of softening agents such as chloroform [4-9]. The remnants of filling materials left on dentin walls may hinder irrigation and medication from effectively cleaning the canals, which can affect adequate disinfection [10]. Moreover, these remnants can hinder adequate sealing [5].
The complex internal morphology of the root canal system, characterized by isthmuses, apical ramifications, accessory canals, and oval canals, significantly influences the effective removal of residual obturated materials from root canals [11, 12].
The challenges faced in removing gutta-percha primarily stem from the obturation methods and the type of sealer used. Epoxy resin-based sealers, as AH Plus (Dentsply Sirona, Konstanz, Germany), are available in a paste-paste mixture with high physical properties [13]. Calcium silicate-based bioceramic sealers promote efficient tissue healing, along with the hydroxyapatite mineralization of dentin, thereby improving the sealing of root canals [6, 14, 15]. Calcium silicate-based EndoSequence BC (Brassler USA, Savannah, GA) demonstrates low cytotoxicity, superior bonding strength, and effective sealing capability [16]. Moreover, several studies have revealed that BC sealer induces mineralization and stimulates the induction of hard tissue [17].
Removing gutta-percha from root canals using NiTi rotary systems is more effective than hand instruments and is characterized by fewer procedural errors [18]. Root canal instrumentation using nickel-titanium (NiTi) instruments usually rotates inside root canals with limited effect in oval-shaped root canals [19, 20]. Despite the application of circumferential filing motions, a proportion of dentin walls remains untouched [21]. Recent innovations have been implemented in instrument designs to increase their cutting efficiency and fatigue resistance. Modifications have also been done in the metallurgy to improve the nanocrystalline structure [22, 23].
In recent years, reciprocating motions have become a common choice for root canal preparation due to their shorter preparation times, high quality, and ease of use [24]. Several researchers have studied the effectiveness of these file systems for endodontic retreatment procedures [9, 12, 25]. Few studies have investigated the impact of contracted access design on the efficacy of retreatment treatments [26].
Therefore, the aim of this in vitro study was to analyse the effect of contracted and traditional endodontic access cavity outlines on the retreatment efficacy of single oval canals using the reciprocal single-file systems when obturated with two different sealers. This aim was based on the hypothesis that none of the systems can completely remove the root filling material from root canals.
2. MATERIALS AND METHODS
This study was designed as an Ex-Vivo comparative study, and for standardization, all procedures were performed by the same operator. Ethical approval for this study was obtained from the Institutional Biomedical Research Ethics Committee of Umm al-Qura University (IRB Approval No. HAPO-02-K-012-2023-06-1664, dated June 20, 2023).
2.1. Sample Size Calculation and Selection
The G*Power statistical power analysis program (version 3.1.9.4) was utilized for sample size determination, indicating that a total sample size (n=40; divided into 10 per subgroup) was adequate to identify an effect size of (F=0.711), achieving an actual power (1-β error) of 0.95 (95%) and a significance level (α error) of 0.05 (5%). Forty extracted human mandibular first and second premolars with mature apices and single roots were collected from the oral surgery clinics of the dental teaching hospital at Umm Al-Qura University in Makkah, Saudi Arabia. The collected teeth were then stored in a 10% formalin solution. The teeth had been extracted due to periodontal disease or orthodontic considerations, and all study participants (from whom mandibular premolars were extracted) provided written informed consent, granting permission to use their extracted teeth in the research. The extracted teeth were rinsed under running water for 60 minutes, then cleaned using a scaler. Periapical radiographs were taken, and the final sample was selected based on specific inclusion and exclusion criteria. Teeth with single roots and fully developed, closed apices were included, while teeth exhibiting multiple canals, fractures, resorption, caries, cracks, open apices, or root curvature exceeding 15° were excluded.
2.2. Samples Grouping
The teeth were divided into two groups of 20 teeth each based on the endodontic access cavity design: Traditional Endodontic Cavity (TEC) and Contracted Endodontic Cavity (CEC). Each group was further subdivided into two subgroups of 10 teeth each according to the type of sealer used: AH Plus sealer or bioceramic (BC) sealer. Accordingly, Group I-A included teeth with TEC, obturated with gutta-percha and AH Plus sealer; Group I-B included teeth with TEC, obturated with gutta-percha and BC sealer; Group II-A included teeth with CEC, obturated with gutta-percha and AH Plus sealer; and Group II-B included teeth with CEC, obturated with gutta-percha and BC sealer.
2.3. Sample Preparation
The teeth were embedded in cold-cured resin blocks. The samples were randomly grouped into two experimental groups based on the type of access cavity preparation (n = 20 each): traditional access cavity preparation and contracted access cavity preparation. The working length was calculated radiographically as 0.5 mm from the apex, and the glide path was established using manual files up to size #25. The cleaning and shaping procedures were done using Protaper Next files (Dentsply Maillefer, Ballaigues, Switzerland). Every file utilized was lubricated with Glyde (Dentsply Maillefer, Ballaigues, Switzerland). Irrigation was performed after each file using 2 mL of 5% NaOCl. Upon completion of instrumentation, all specimens were irrigated with 5 mL of 17% EDTA solution, followed by 5 mL of saline solution, and then dried using appropriate paper points. The specimens were subsequently subgrouped according to the sealer used (n = 10 each): AH Plus (DenTsply, Germany) or BioRoot RCS (Septodont, France). The canals were then obturated with gutta-percha and sealer (Dentsply Maillefer, Ballaigues, Switzerland) utilizing the cold lateral condensation technique. The quality of obturation was assessed radiographically and considered adequate when no voids were detected on the radiograph. The access cavity was filled with interim filling material (Cavit, Detrey, Dentsply) and kept in a humidifier at 37°C for 30 days.
2.4. Retreatment Technique
For filling material removal, the Reciproc Blue RB25 and RB40 instruments (VDW GmbH) were used in all experimental groups, and the protocol was followed according to the manufacturer's instructions. NaOCl alternating with EDTA was used as the irrigation protocol; root canals were then dried using the corresponding paper points (size #40/0.04; VDW GmbH). The retreatment was deemed sufficient when no visible remnants of obturating material were observed.
2.5. Time Recording
The retreatment time was recorded in minutes using a stopwatch till adequate gutta-percha removal was achieved. The time required for changing the instrument was excluded from the analysis.
2.6. Cone Beam Computed Tomography (CBCT) Evaluation and 3D Evaluation of the Volumetric Images
After completion of the retreatment procedure, the specimens were scanned using cone-beam computed tomography (CBCT) to calculate the percentage of residual obturating material at the coronal, middle, and apical thirds of the root [12]. The CBCT images were acquired using the Planmeca ProMax 3D scanner (Planmeca, Helsinki, Finland). Each sample was scanned using an amorphous silicon flat panel sensor with a 0.5 mm focal spot size, 14-bit grayscale resolution, and a cesium iodide (CsI) scintillator. The scanning parameters were standardized for all samples: a voxel size of 0.3 mm, a tube current of 18.54 mA, a tube voltage of 120 kVp, and a scanning time of 8.9 seconds. Following the acquisition of cone-beam CT images, the Digital Imaging and Communications in Medicine (DICOM) files were imported into Mimics Medical (v19.0; Materialise, Belgium), an image processing application used for three-dimensional modeling and design. The amount of obturation material that remained was measured and examined using a threshold procedure. Along the length of the root, masks were produced at the apical, middle, and coronal levels, and the associated volumes were calculated in cubic millimeters (Fig. 1).
2.7. Statistical Analysis
Numerical data were assessed for normality by examining the data distribution and conducting normality tests (Kolmogorov-Smirnov and Shapiro-Wilk tests). The retreatment time data had a normal (parametric) distribution; however, the volume of remaining obturating material data demonstrated a non-normal (non-parametric) distribution. Data was presented as median, range, mean, and standard deviation. The one-way ANOVA test was employed to compare the groups for parametric data. Bonferroni's post-hoc test was employed for pairwise comparisons following a significant ANOVA test. The Mann-Whitney U test was utilized to compare the two access techniques and the two sealing types for non-parametric data. The Friedman test was employed to compare root levels within the group. The Kruskal-Wallis test was employed to compare the total volume of residual obturating material between the four groups. Dunn's test was utilized for pairwise comparisons where either Friedman’s test or the Kruskal-Wallis test yielded significant results. The significance level was established at p < 0.05. Statistical analysis was conducted using IBM SPSS Statistics for Windows, Version 23.0. Armonk, New York: IBM Corporation.
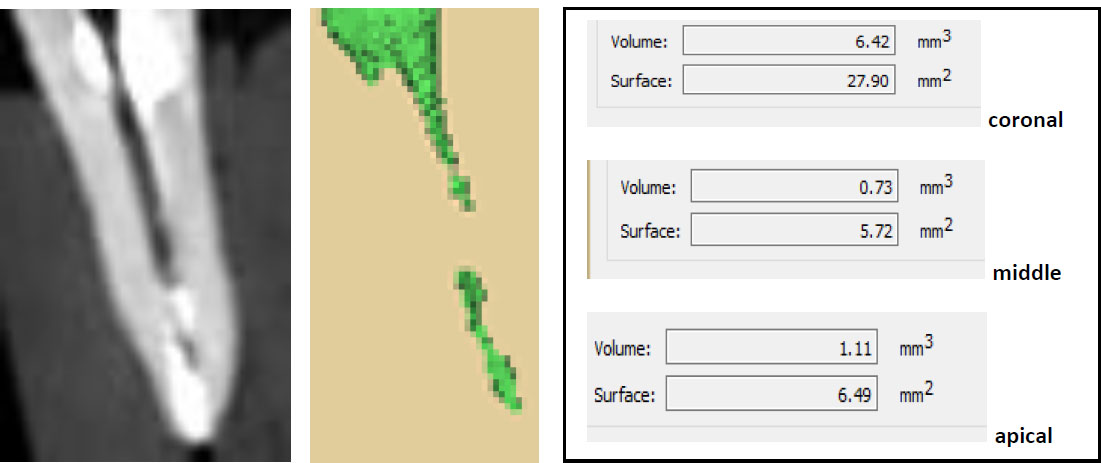
Cone beam CT showing the measuring technique of residual filling material in contracted access + BC sealer.
| Traditional Access + AH Sealer (n = 10) | Traditional Access + BC Sealer (n = 10) | Contracted Access + AH Sealer (n = 10) | Contracted Access + BC Sealer (n = 10) | p-value | Effect Size (Eta Squared) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| 4.1 B | 0.91 | 4.56 B | 0.99 | 4.11 B | 0.58 | 5.02 A | 0.57 | 0.038* | 0.206 |
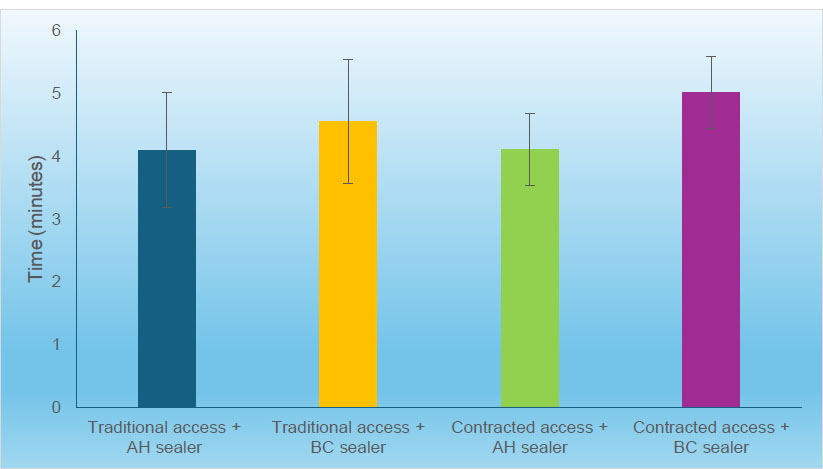
Bar chart representing mean and standard deviation of the results of retreatment times in different groups.
3. RESULTS
3.1. Retreatment Time
The results showed a statistically significant difference in retreatment times among the groups (p = 0.038; effect size = 0.206). The group with contracted access and BC sealer demonstrated a significantly higher mean retreatment time compared to the other three groups. However, pairwise comparisons among the remaining groups revealed no statistically significant differences (Table 1, Fig. 2).
3.2. Volume of Remaining Obturating Material
3.2.1. Comparison between Access Techniques
As shown in Table 2 (group AH sealer), there was no significant difference between traditional and contracted access designs at the coronal, middle, and apical root levels, as well as the overall volume of remaining obturating material.
While in the BC sealer group, there was no statistically significant difference between traditional and contracted access techniques at the coronal root level. While at the middle, apical root levels as well as the overall volume of remaining obturating material, traditional access showed statistically significantly lower volume of remaining obturating material than contracted access (p-value = 0.017, Effect size = 1.258), (p-value = 0.002, Effect size = 1.835) and (p-value = 0.021, Effect size = 1.203), respectively.
3.2.2. Comparison between sealers
There was no statistically significant difference between AH and BC with traditional and contracted accesses. While at the coronal root level as well as the overall volume of remaining obturating material, AH sealer showed statistically significantly lower volume of remaining obturating material than BC sealer (p-value = 0.001 and 0.031, respectively) (Table 3).
3.2.3. Comparison between Root Levels
Analysis of the percentage of remaining obturating material at different root levels is presented in Table 4. A statistically significant difference was observed among the root levels (p = 0.004, <0.001, and <0.001, respectively). Pairwise comparisons revealed that the coronal third had a significantly higher volume of remaining obturating material compared to the middle and apical thirds (Table 4).
3.2.4. Comparison between the Overall Volume of Remaining Obturating Material in the Four Groups
Regardless of the root level, the results showed that there was no significant difference among the overall volume of remaining obturating material in the four groups (Table 5, Fig. 3).
| Sealer | Root Level | Traditional Access (n = 10) | Contracted Access (n = 10) | p-value | Effect Size (d) | ||
|---|---|---|---|---|---|---|---|
| Median (Range) | Mean (SD) | Median (Range) | Mean (SD) | ||||
| AH sealer | Coronal | 2.5 (1.2, 4.9) | 2.69 (1.28) | 2.5 (0.9, 3.4) | 2.26 (0.82) | 0.519 | 0.29 |
| Middle | 1.2 (0.5, 10.1) | 2.01 (2.88) | 1.65 (0, 3) | 1.66 (0.97) | 0.448 | 0.343 | |
| Apical | 1.85 (0.8, 3) | 1.89 (0.78) | 1.8 (0.5, 3.9) | 1.9 (1.03) | 0.940 | 0.034 | |
| Overall | 1.8 (1.13, 5.27) | 2.2 (1.23) | 2.15 (0.77, 2.93) | 1.94 (0.83) | 0.791 | 0.119 | |
| BC sealer | Coronal | 2.9 (0.9, 6.1) | 3.22 (1.75) | 4 (2.6, 8.6) | 4.48 (1.82) | 0.130 | 0.718 |
| Middle | 0.45 (0, 2.3) | 0.75 (0.9) | 1.55 (0.8, 2.5) | 1.67 (0.54) | 0.017* | 1.258 | |
| Apical | 1.3 (0, 2.8) | 1.27 (0.88) | 2.35 (1.3, 3.7) | 2.57 (0.77) | 0.002* | 1.835 | |
| Overall | 1.62 (0.43, 3.23) | 1.75 (0.94) | 2.8 (1.77, 4.03) | 2.91 (0.73) | 0.021* | 1.203 | |
| Access Technique | Root Level | AH Sealer (n = 10) | BC Sealer (n = 10) | p-value | Effect Size (d) | ||
|---|---|---|---|---|---|---|---|
| Median (Range) | Mean (SD) | Median (Range) | Mean (SD) | ||||
| Traditional access | Coronal | 2.5 (1.2, 4.9) | 2.69 (1.28) | 2.9 (0.9, 6.1) | 3.22 (1.75) | 0.596 | 0.238 |
| Middle | 1.2 (0.5, 10.1) | 2.01 (2.88) | 0.45 (0, 2.3) | 0.75 (0.9) | 0.082 | 0.844 | |
| Apical | 1.85 (0.8, 3) | 1.89 (0.78) | 1.3 (0, 2.8) | 1.27 (0.88) | 0.096 | 0.801 | |
| Overall | 1.8 (1.13, 5.27) | 2.2 (1.23) | 1.62 (0.43, 3.23) | 1.75 (0.94) | 0.449 | 0.343 | |
| Contracted access | Coronal | 2.5 (0.9, 3.4) | 2.26 (0.82) | 4 (2.6, 8.6) | 4.48 (1.82) | 0.001* | 2.065 |
| Middle | 1.65 (0, 3) | 1.66 (0.97) | 1.55 (0.8, 2.5) | 1.67 (0.54) | 0.940 | 0.034 | |
| Apical | 1.8 (0.5, 3.9) | 1.9 (1.03) | 2.35 (1.3, 3.7) | 2.57 (0.77) | 0.096 | 0.801 | |
| Overall | 2.15 (0.77, 2.93) | 1.94 (0.83) | 2.8 (1.77, 4.03) | 2.91 (0.73) | 0.031* | 1.099 | |
| Access Technique | Root Level | AH Sealer (n = 10) | BC Sealer (n = 10) | ||
|---|---|---|---|---|---|
| Median (Range) | Mean (SD) | Median (Range) | Mean (SD) | ||
| Traditional access | Coronal | 2.5 (1.2, 4.9) A | 2.69 (1.28) | 2.9 (0.9, 6.1) A | 3.22 (1.75) |
| Middle | 1.2 (0.5, 10.1) B | 2.01 (2.88) | 0.45 (0, 2.3) C | 0.75 (0.9) | |
| Apical | 1.85 (0.8, 3) B | 1.89 (0.78) | 1.3 (0, 2.8) B | 1.27 (0.88) | |
| p-value | 0.004* | <0.001* | |||
| Effect size (w) | 0.556 | 0.833 | |||
| Contracted access | Coronal | 2.5 (0.9, 3.4) | 2.26 (0.82) | 4 (2.6, 8.6) A | 4.48 (1.82) |
| Middle | 1.65 (0, 3) | 1.66 (0.97) | 1.55 (0.8, 2.5) C | 1.67 (0.54) | |
| Apical | 1.8 (0.5, 3.9) | 1.9 (1.03) | 2.35 (1.3, 3.7) B | 2.57 (0.77) | |
| p-value | 0.067 | <0.001* | |||
| Effect size (w) | 0.27 | 0.91 | |||
| Overall Remnant | Traditional Access + AH Sealer (n = 10) | Traditional Access + BC Sealer (n = 10) | Contracted Access + AH Sealer (n = 10) | Contracted Access + BC Sealer (n = 10) | p-value | Effect Size (Eta squared) |
|---|---|---|---|---|---|---|
| Median (Range) | 1.8 (1.13, 5.27) | 1.3 (0, 2.8) | 1.8 (0.5, 3.9) | 2.8 (1.77, 4.03) | 0.051 | 0.017 |
| Mean (SD) | 2.2 (1.23) | 1.27 (0.88) | 1.9 (1.03) | 2.91 (0.73) |
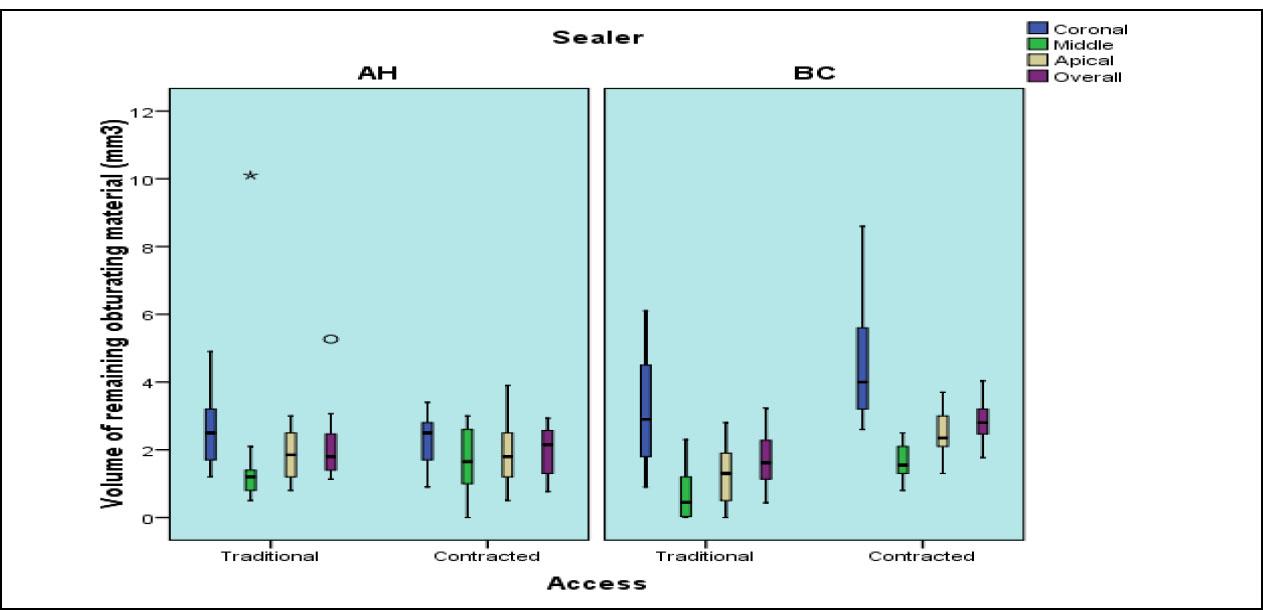
Box plot showing median and range results of volume of remaining obturating materials in different groups (Star and circle represent outliers).
4. DISCUSSION
Contracted designs of access cavities should be effective as traditional access cavities, regardless of the benefits of maintaining the pericervical dentin [26]. More reports are required to assess the impact of various access cavity outlines on the performance of NiTi rotary files in removing root canal filling materials.
To avoid the disadvantages of previous evaluation techniques, such as sectioning and 2-D radiographic techniques, three-dimensional CBCT scanning was used in this study. This technique is non-invasive, ensuring a more accurate assessment of residual debris on the canal walls and decreasing the bias in image interpretation [10, 20].
Although the general design of NiTi rotary systems is suitable for removing root-filling materials, no studies to date have proven the total removal of filling material during the retreatment of root canals, regardless of the techniques or instruments employed [4, 7, 8, 12, 25]. Single-rooted human extracted mandibular premolars were selected to be used in this study. It was reported that the prevalence of oval-shaped canal morphology is 27% [12, 19].
Root canal fillings using gutta-percha with sealer are the most common filling material used for obturating the root canals [27]. An epoxy-resin sealer is regarded as the gold standard for root canal filling materials, so it was used in comparison to BC sealer in this study [16, 27, 28].
In the current study, the removal of root canal filling was performed using rotary files with reciprocating motion, without the use of solvent, as concerns have been raised regarding the cytotoxicity of solvents. Some studies reported that rotary instruments without solvent shortened the time of retreatment [29], while other studies showed that when solvents were utilized, a thin coating of softened gutta-percha would adhere to the dentin walls of the root canals, increasing the time needed for the removal of filling materials [6].
Moreover, the solvent did not play a significant role in the cleanliness of the root canal wall, as it resulted in an increased percentage of gutta-percha and sealer remnants inside the dentinal tubules of the root canal walls, which may impede adherence to new filling materials on the dentin walls [4, 6].
The type of instrument motion significantly influences the removal of root filling materials. In the present study, the reciprocating motion was used. Numerous investigations have revealed that the adaptive reciprocating motion removes a greater percentage of filling materials from root canals compared to continuous rotational movement [25, 30, 31]. However, the results were conflicting regarding the efficiency of reciprocating motion in removing root canal filling materials. Rodig et al. [32] stated that no statistically significant variations were observed between Reciproc and ProTaper Universal in the context of retreatment. Kfir et al. [33] established that reciprocating SafeSider files were as successful as ProTaper Universal retreatment equipment.
The results of the present study showed that with contracted access and BC sealer, there was a significant difference between the root levels, as the coronal level showed the highest volume of remaining obturating material (Figs. 1 and 2). In agreement with our findings, Hess et al. [34], and others concluded that more sealer remnants were found with BC sealers than resin-based sealers [16, 35, 36]. Moreover, according to various studies, bioceramic sealer becomes harder after setting, due to its greater penetration inside the dentinal tubules, so the retreatability is reduced [14, 15].
In contrast to our results, as reported by Jurić Kaćunić et al. [36] and others, who concluded that BioRoot RCS showed better retreatability than AH Plus [37-41]. Contrary to these results, other studies reported no significant difference in the quantity of remaining filling material during the retreatment procedure between bioceramic sealer and AH Plus sealer, and these results agreed with those of other studies [42, 43]. The discrepancies in results can be attributed to the differing protocols of the employed methodology, including variations in access design, the different retreatment files evaluated, and the evaluation methodologies that utilize two-dimensional or three-dimensional methods.
The results of the present study showed that the percentage of residual filling materials left was higher in the coronal thirds of the root canal in the contracted access design (Fig. 3). This finding was in agreement with Elsheref et al. [25], who found that the coronal segment showed the highest mean value of remaining filling materials using the Reciproc file. The results of this study can be attributed to the presence of more coronal interferences in the contracted access and to variations in tooth morphology. These results are in agreement with previous studies [16, 30], which attributed their findings to the absence of Gates-Glidden drills. However, the results of the present study contradict other reports that found a greater quantity of residual filling material in the apical region of root canals. Those studies explained their outcomes by citing the difficulty of engaging rotary instruments in the apical third [40-43].
5. STUDY LIMITATIONS
The shortcomings of this study include the use of an ex vivo model, which doesn’t mimic clinical situations. Therefore, more studies should be conducted to focus attention on long-term clinical studies to evaluate and compare different techniques and/or materials. Additionally, the application of μ-CT would yield more accurate results and is recommended for further studies. More research on larger samples is required to validate the results obtained from this study.
CONCLUSION
Within the limitations of this study, it can be concluded that the use of the reciproc retreatment system was not efficient in completely cleaning the oval canals, regardless of the design of the access cavity or the sealer used. The remaining filling material left in canals obturated with BC sealer was more than AH plus. The single-rooted teeth with a contracted endodontic access cavity and used BC sealers in obturation showed the highest time needed for retreatment, mostly due to their constricted nature.
The volume of remaining filling material was highest in the coronal third of the root. However, remnants of obturation materials were observed on the root canal dentin regardless of the retreatment system or access cavity design used.
Further research should be conducted to evaluate the effectiveness of various instruments and techniques in facilitating retreatment procedures for oval-shaped canals with a contracted access cavity design.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| Ex Vivo | = Latin for 'out of the living' |
| CEC | = Contracted Endodontic Cavity |
| TEC | = Traditional Endodontic Cavity |
| NiTi | = Nickel Titanium |
| NaOCl | = Sodium Chlorite |
| EDTA | = Ethylenediaminetetraacetic acid |
| CBCT | = Cone Beam Computed Tomography |
| 3D | = Three Dimensions |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The current study was approved by the Institutional Biomedical Research Ethics Committee of Umm al-Qura University (IRB Approval No. HAPO-02-K-012-2023-06-1664 & Date: 20/6/2023).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

