All published articles of this journal are available on ScienceDirect.

Integration of Health Behaviour Theories in Dentistry: A Systematic Review
Abstract
Background
Oral diseases, such as dental caries, periodontal disease, and tooth loss, can cause physical discomfort and contribute to functional limitations, which in turn affect psychological well-being and self-esteem. However, many of these oral health issues are largely preventable through regular oral hygiene practices and routine dental care. Various interventions based on health behavior theories have been proposed to enhance self-care and treatment compliance. In this systematic literature review, we aimed to evaluate the efficacy of these theoretical frameworks in enhancing preventative dental care practices and improving treatment outcomes.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic search was conducted using PubMed, Embase, Scopus, and the Cochrane databases for studies published between January 2000 and December 2023. The search targeted studies applying health behavior theories in dental settings to enhance oral health outcomes. Inclusion criteria comprised randomized controlled trials, cross-sectional studies, and quasi-experimental designs with no geographical restrictions. The protocol was registered in PROSPERO (reg. no. CRD42024590108). Two independent reviewers assessed paper quality using standard criteria, categorizing and screening the bias risk based on Scores.
Results
The search yielded 9,896 records, of which 39 studies met the inclusion standards following screening and full-text review. These studies demonstrated diverse applications of health behavior theories across various populations and settings, ranging from motivational interviewing to the Health Belief Model (HBM) and Theory of Planned Behavior (TPB). The use of these theory-based interventions resulted in significant enhancements in oral health behaviors and clinical outcomes.
Conclusion
Interventions grounded in health behavior theories show promise in improving oral health outcomes and patient behaviors. Although our review focused on three primary theories (HBM, TPB, and SCT), theories such as HBM and TPB have been shown to have a more significant impact compared to other theories. While these findings highlight the value of evidence-based psychological frameworks, the conclusions should be interpreted with caution.
1. INTRODUCTION
Oral health is a fundamental component of overall health and well-being, influencing nutrition, speech, self-esteem, and quality of life. Despite being largely preventable, oral diseases, such as dental caries and periodontal disease, remain highly prevalent worldwide, particularly among vulnerable populations such as children and pregnant women [1, 2]. Furthermore, poor oral health has been linked to several serious systemic conditions, including cardiovascular disease, diabetes complications, respiratory infections, dementia, and Alzheimer’s disease [3-6]. As a result, treatments for oral health and their associated conditions contribute to considerable spending globally [7, 8]. As a result, the World Health Organization (WHO) identified oral health as a vital component of overall well-being and quality of life [9, 10].
An estimated three and a half billion people, nearly half of the world’s population, are thought to suffer from some oral disease [9]. Poor oral health often results from a combination of factors, including inadequate oral hygiene, high sugar consumption, tobacco and alcohol use, limited access to dental care, chronic illnesses such as diabetes, and a lack of awareness or education about proper oral care. Most oral health conditions can be prevented by following good oral hygiene, routine dental care, and reducing the intake of sugar, alcohol, and tobacco. However, this requires education to increase awareness and interventions to change unhealthy habits. Various theoretical models have been proposed to better understand the complex factors that influence health behaviors. These theoretical models provide structured frameworks for designing effective interventions that promote positive behavior change and improve overall health outcomes [11]. The most common framework used to promote oral health is the health belief model. This framework is used to understand and predict health behaviors by examining how individuals perceive a health threat and the value they place on taking preventive action. It suggests that people are more likely to act if they feel personally at risk, believe the action will be effective and can manage any obstacles to taking that action. Other commonly used models in health behavior change include Motivational interviewing, Health Action Process Approach (HAPA), Theory of Planned Behavior (TPB), Self-Efficacy Theory and the Social Cognitive Theory (SCT). The TPB is based on the fact that behavior is guided by intentions, which are shaped by a person’s attitude toward the behavior, perceived social expectations, and their sense of control over the behavior. The HAPA method emphasizes the mechanisms related to the role of social cognition and self-regulation. Further, motivation interviewing focuses on counselling to drive health behavior change. SCT explores the interaction between personal factors, the environment, and behavior, highlighting the roles of observational learning, reinforcement, and confidence in one’s ability to take action [12]. Studies have shown that the use of psychological interventions can enhance oral health behaviors. However, Werner et al. (2016) showed that psychological interventions alone are not sufficient to prevent conditions like plaque and gingivitis [2]. Therefore, a multifaceted approach that combines psychological interventions with clinical care is essential for long-lasting adherence to practices that are conducive to oral health [12, 13].
In this systematic literature review, we aimed to evaluate the impact of various interventions grounded on behavioral theories such as TPB, SCT, and HBM on increasing adherence to good oral health practices and, ultimately, oral health outcomes [2]. The outcomes of this literature review could be used to guide dental practitioners on how best to apply behavioral theories to enhance oral health practices and as a basis for future research.
2. METHODS
2.1. Search Strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, and the protocol was registered to PROSPERO (no. ID: CRD42024627302). Our search was structured around the PICO framework to precisely target studies that involved (1) Populations across all age groups under study, (2) Interventions employing a wide array of health behavior theories, (3) Comparators comprising groups not receiving theory-based health behavior interventions; and (4) Outcomes related to dental care behaviors (such as dietary habits, oral hygiene practices, and dental visitation patterns) and measurable clinical outcomes (including the DMFT score, the Papillary Bleeding Index, and the Gingival Index) (Table 1). PubMed, Scopus, Embase, and the Cochrane Library were searched to identify relevant studies.
| Category | Keywords |
|---|---|
| Oral Health / Dentistry Terms | “oral health education”, “oral health promotion”, “oral disease”, “oral health program”, “oral health evaluation”, “oral health program”, “oral health intervention” |
| MeSH keywords | “Psychological Theory”, “Nursing Theory”, “Models, Theoretical” |
2.2. Inclusion and Exclusion Criteria
All cross-sectional, randomized controlled trials (RCTs) or quasi-experimental studies evaluating the effectiveness of health behavior theories in promoting oral health outcomes published between January 1999 and December 2023 were included in the study. Systematic reviews, meta-analyses, qualitative studies, non-English publications, grey literature, and research papers with inaccessible full texts were excluded.
The quality of the included studies was assessed utilizing a standardized assessment tool PICO (population, intervention, comparison, outcomes) that considered factors such as study category, number of participants, and validity of the measurements. The search strategy for this systematic review was meticulously crafted to capture a comprehensive range of studies exploring the application of health behavior theories within the realm of dentistry. Utilizing three primary databases—PubMed, Scopus, Embase AND, OR the Cochrane Library—our strategy incorporated a series of complex search terms and Medical Subject Headings (MeSH) to ensure a thorough retrieval of relevant literature. We focused on identifying research that integrated health behavior theories such as the HBM, TPB, SCT, Transtheoretical Model, Theory of Reasoned Action (TRA), and Salutogenesis Theory in dental care practices.
2.3. Study Selection
The titles and abstracts of all articles retrieved through the search strategy were independently screened by two reviewers to exclude clearly irrelevant studies. Any disagreements between the reviewers were resolved through discussion and, when necessary, by consultation with a third reviewer to reach a consensus. This initial screening was followed by a full-text review of potentially eligible articles to assess their relevance based on predefined inclusion and exclusion criteria.
2.4. Data Extraction and Analysis
For each included study, key information was extracted and documented in an Excel spreadsheet, including author(s), year of publication, country of origin, participant characteristics, the specific health behavior theory applied, study design, outcome measures, and main findings.
Data extraction was conducted by a single reviewer, with any uncertainties or discrepancies resolved through discussion or, when needed, by involving the third reviewer. To enable structured comparison across theoretical models, each study was categorized according to the behavioral theory it employed.
2.5. Quality Assessment
The quality of the included papers was assessed by 2 independent reviewers using the same criteria used in similar health behaviour theories, as shown in Table 2 [2-4,12]. The risk of bias in every paper was characterized on the basis of the overall sum groupings received as 0-5 (weak), 6-7.0 (moderate), and 7.1-10 (clear).
| Category | Score Range | Description |
|---|---|---|
| Weak | 0–5 | Lack of evidence or poorly considered study methodology. |
| Moderate | 6–7.0 | Weak methodology with limited information provided on the intervention strategies or outcomes. The conclusions are not well supported. |
| Clear | 7.1–10 | Robust and well-structured study with comprehensive methodology and reporting |
3. RESULTS
3.1. Search Strategy Results
The results of the search strategy are summarized in the PRIMSA flowchart (Fig. 1). The initial search strategy revealed a total of 9,896 articles. After the removal of duplicates, 4,161 articles remained for consideration. In the first screening round, a total of 3,980 papers were deemed ineligible for the study. The subsequent full-text analysis led to the exclusion of an additional 129 papers and 13 disagreements. Ultimately, 39 articles were included in the systematic review.
3.2. Characteristics of the Studies
The characteristics of the study are summarized in Table 3. Most studies (n 15, =38.4%) were published after 2020. Studies conducted between 2019 and 2015 (n =13, 33.3%) were also included, and the rest studies were prior to 2015 (n=11, 28.2%). This review included studies conducted across various countries. The majority of the studies were conducted in Iran (10 studies), followed by China (4 studies), Canada (3 studies), and Belgium (3 studies). The United States, the United Kingdom, and Saudi Arabia conducted 2 studies each. Additionally, one study was conducted in each of the following countries: Turkey, Sweden, Sri Lanka, Malaysia, India, Norway, Finland, Spain, Japan, Egypt, Australia, Hong Kong, and Romania. The number of participants in the study ranged from 30 to 1328, which indicates a wide range of variation in the engagement and intervention scope between studies. The most common study design was cross-sectional, used in 18 studies (46.1%), followed by randomized clinical trials, which accounted for 14 studies (35.5%). Each design offered distinct insights into the application and effectiveness of health behavior theories within dental health contexts. A significant portion of the research (n=6, 15.4%) primarily targeted adolescents and young adults, reflecting a concentrated effort to influence oral health behaviors at a formative stage. A variety of sampling techniques were used across the studies, with many adopting stratified or cluster random sampling to enhance the representativeness of participant groups. However, several studies lacked transparency in reporting their sampling methods, which hindered the ability to generalize their findings to broader populations.
3.3. Types of Interventions and Outcomes
The main behavioural theories used to improve oral health were motivational interviewing, HBM, HAPA, TBH, salutogenic theory, and self-efficacy theory. These models served as the foundation for interventions aimed at modifying oral health knowledge, attitudes, and behaviors (Fig. 2). The outcomes of the interventions were measured through various clinical and self-reported indicators such as tooth brushing frequency, dental visitation habits, and oral hygiene indices. The outcomes reported by the studies were multifaceted, with some demonstrating significant improvements in oral health behaviors and clinical outcomes post-intervention. These findings suggest that theory-based educational and motivational strategies can promote better oral health. However, the diversity in outcome measures and reporting standards used across studies made it difficult to compare findings.
3.4. Motivational Interviewing
Five studies made use of motivational interviewing as an interventional approach to address several oral health issues, including oral hygiene and dental attendance [14-18]. Compared to traditional didactic approaches, motivational interviewing (MI) has demonstrated greater success in improving oral hygiene behaviors, with participants showing significantly increased toothbrushing frequency and a corresponding reduction in plaque index scores. However, for pregnant females, it was observed that the effects were similar to health education aimed at improving dental attendance. Our findings provide strong evidence that patient-centered communication leads to better outcomes than standard advice-giving, especially in facilitating lifestyle changes. MI stands out for its collaborative and person-focused nature, which aims to enhance intrinsic motivation toward healthier behaviors. This method helps individuals resolve ambivalence and make informed decisions, supporting long-term behavior change [19, 20].
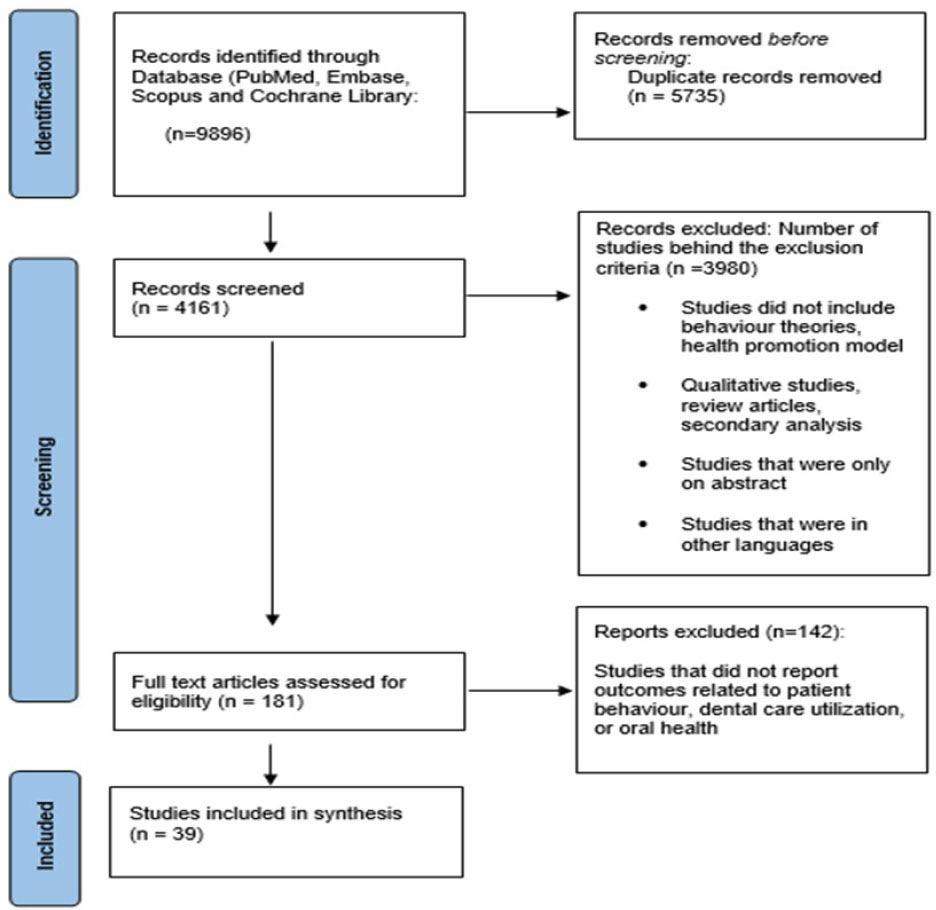
PRISMA flowchart.
| Author, Year, Country/Refs. | Characteristics of Study Participants | Health Behavior Theory Type/ Study Design | Outcome Measurement | Results |
|---|---|---|---|---|
| Dermen et al, 2014, USA [14] | 15-minute exam and 30-minute intervention. Not to brush on day of exam. 30 in Intervention and 30 in control arm | MI, compared to traditional, didactic control intervention / Randomized Controlled Trial - Longitudinal | Improvement OH, health care utilization, and health outcomes among individuals in inpatient treatment for AUDs | MI participants significantly more frequent toothbrushing during follow-up than control |
| Scheerman et al, 2019, Iran [36] | Adolescents (N = 791) 12–17 years, recruited from high schools in Qazvin city. Adolescent as intervention (A group; n = 253), an adolescent + mother intervention (A + M; n = 260), and control group (n = 278). | HAPA/Cluster randomized controlled trial | Psychosocial variables, toothbrushing behaviour, Visual PI, and Community Periodontal Index (CPI) | ↑ In adolescent toothbrushing at one, 6-month follow-ups in both intervention groups compared to control group. Adolescents in A + M group showed significant greater improvements in their toothbrushing behaviour, Visual PI, and CPI scores than adolescents in A group. |
| Sanaeinasab et al, 2022, Iran [21] | 112 children ages 6–12 years old in public dental clinic; 56 (Intervention) and 56 (Control arm) | Intervention group, 5 consecutive weekly educational sessions based on HBM, control group received only routine education delivered by dental clinic/ Randomized Controlled Trial |
DMFT score, BI, and responses to HBM questionnaire | All HBM domains were improved at follow-up in intervention compared to control. Highest change in perceived susceptibility, whereas smallest changes were in perceived severity and perceived benefits. Significant change in BI from baseline to follow-up in intervention. All components of DMFT score except missing teeth also improved in intervention compared to controls. |
| Shi et al, 2021, China [41] | 414 students in third-grade from 10 classes of Mingqiang Primary School, Shanghai. | TPB/ Cross-sectional study | TPB variables, oral health knowledge and past oral health behaviors. Exploratory factor analysis using and analyzing TPB items. | Attitudes, subjective norms, perceived behavioral control, and past oral health behaviors were associated with intention to improve oral health behaviors. |
| Amin et al, 2019, Canada [54] | 274 newcomer parents with child aged 1 to 12 years who had lived in Canada for 10 years or less participated | TPB/ Cross-sectional study | Measure their DMFT, and parents completed a self-administered questionnaire. Parental attitudes, subjective norms, PBC, & intention were examined using Structural Equation Modeling as predictors of dental attendance behavior and caries experience | Attitude and PBC significantly predicted the intention; Intention significantly predicted behavior, but behavior could not predict caries experience. |
| Riedy et al, 2015, Canada [16] | 400 women; (1) prenatal MI followed by postnatal MI (n=145), (2) prenatal MI followed by postnatal HE (n=59), (3) prenatal HE followed by postnatal MI (n=146), and (4) prenatal HE followed by postnatal HE (n=50) | MI/ Randomized Controlled Trial | Primary outcomes were dental attendance during pregnancy for mother and for child by age 18 months. | MI did not lead to greater attendance when compared to HE alone |
| Martin et al, 2020, USA [43] | Child 6–36 months/caregiver dyads from 10 Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) centers and 10 pediatric medical clinics; Community Health Worker (CHW) intervention and usual care. 18-23 dyads from each of 20 sites (clinic or WIC center) for total of 420 caregiver/child dyads |
TPB; intervention is oral health support from CHWs delivered in 4 visits to individual families over one-year / Cluster-randomized controlled trial |
Data on brushing frequency, plaque, and other oral health behaviors are collected at three timepoints: baseline, 6-, and 12-months | Intervention overall improved child’s oral health status by increasing brush frequency and improvement in plaque score. |
| Armoon et al, 2021, Iran [53] | 160 staff in Baqiyatallah Hospital. 6 hospital wards were selected using randomized multi-stratified sampling frame; 80 participants in intervention arm and 80 in control group | TPB/ Pre-post intervention study | TPB model (attitudes, subjective norms, perceived behavioral control intentions). | Significant variations ↔ groups immediately after educational intervention concerning attitudes, subjective norms, perceived behavioral control, intentions to seek treatment, oral health behavior, DMFT, bleeding on probing. |
| Yekaninejad et al, 2012, Iran [33] | 392 school-children in 6 schools ↔ September 2010 to March 2011. Three groups’ schools: comprehensive focussed on children, their parents, and school staff (n=131), student (n=127), and control (n=134). | HBM/ Randomized Controlled Trial | Change in oral-health behaviors (brushing and flossing). Changes in OH and Community Periodontal indices and in HBM components. | Comprehensive intervention group brushed and flossed significantly more frequently compared with those in student intervention group |
| Shahnazi et al, 2014, Iran [32] | 56 mothers with 3-6 Years old Children. Divided into experimental and control randomly | HBM/ Quasi-experimental study | HBM constructs - mother’s knowledge, perceived benefits and barriers, perceived susceptibility and perceived severity | Mean score of all aspects of HBM in experimental group had significant difference in comparison with control group. |
| Wickremasinghe, 2017, Sri Lanka [31] | 3 groups of 15-year-old school children; 208 in each group. Intervention group received HBM based HE intervention. One control group received didactic education intervention while other acted as an inactive control group. | HBM/ Randomized Controlled Trial | Oral health related perceptions, oral health related behaviours and oral health status |
All outcome improved significantly in HBM group while only level of plaque and use of fluoride toothpaste improved in didactic education group. |
| Ab Malik et al, 2017, Malaysia [55] | 10 public hospitals; 5 hospitals as test group (277 registered nurses) and 5 as control (270 registered nurses). Intervention - Web-based continuing professional development program on providing OH care to stroke patients using TPB | TPB/ Cluster Randomized Controlled Trial | TPB Domains: “attitude,” “subjective norm” (SN), “PBC, “general intention” (GI), and “knowledge” related to providing OH care | Significant difference in changes in scores of attitudes and subjective norm but not other TPB domains at 1 month. Significant differences in changes in scores of GI, attitudes, SN and knowledge were reported at 6 months ↔ groups. |
| Uguz et al, 2023, Turkey [18] | 156 healthy early adolescents aged ↔ 10–12 years; Basic OH (n = 39), video monitored (n = 39), plaque disclosed method (PDM) (n = 39), and MI (MI) (n = 39) groups. | MI/ Randomized Controlled Trial | Change in levels of knowledge, attitude and behavior related to oral health. | Slight ↑ was reported in knowledge and attitude levels in PDM and video groups, there was higher ↑ in behavior and attitude levels in MI group. PI score reduction was greater in MI group than in other groups |
| Shmarina et al, 2022, Sweden [40] | 146 individuals, aged 60 years and older, participated in a population-based epidemiological study 2011–2012 | SI/ Cross-sectional study | Number of remaining teeth, DMFT-index and risk assessment, and salutogenic factors as artifactual-material, cognitive-emotional and valuative-attitudinal. | Significant associations ↔ outcome variables and salutogenic factors were reported |
| Alhazmi et al, 2021, Saudi Arabia [30] | 406 middle and high school’s students, and first-year students at Jazan University | HBM/ Cross-sectional study | 27 items to examine the constructs of HBM | Perceived barrier score was high with low self-efficacy scores; family income, perceived susceptibility, and risk severity constructs predict use of fashion braces. |
| Van, et al. 2013, Belgium [38] | 1157 parents of 5year-old children, answering questionnaire measuring 3 behaviours (dietary habits, oral hygiene, dental attendance) and determinants (attitude, subjective norms, perceived behavioural control, intention). | TPB/ Cross-sectional study | Behaviours related to oral health and their determinants | TPB components were significant predictors of intentions and behaviours |
| Defranc et al, 2008, Belgium [49] | Measure the determinants of oral health related behaviour in health care workers, based on TPB Behaviour; 201 health care workers for initial validation and 966 other health care workers for a replication. |
TPB/ Cross-sectional study | Oral health behaviour and attendance | Scale scores accounted for a significant proportion of variance in intention to avoid sweet snacks, to brush teeth, and to attend dental check-ups, and of frequency of consumption of sweet drinks and brushing. |
| Dumitrescu et al, 2011, Norway [48] | 153 first-year undergraduate medical students, University of Medicine and Pharmacy “Carol Davila” | TPB/ Cross-sectional study | Intentions, attitudes, subjective norms, perceived behavioral control, oral health knowledge, and current oral hygiene behaviors |
Attitude, perceived behavioral control, and oral health knowledge were reported to be predictors of intention to improve oral health behaviors |
| Rajeh MT, 2022, Saudi Arabia [42] | 1,328 adults living in the Jeddah city | TPB/ Cross-sectional study | Behavioral intention, oral health knowledge and TPB constructs (attitudes, perceived behavioral control, and subjective norms) | TPB model explained 72% of variance in oral health behavioral intentions; TPB constructs of attitudes, subjective norms and perceived behavioral control were significant predictors of OHBI, |
| Xiang et al, 2020, China [29] | 1207 Grade 2 students from 12 secondary schools in Hong Kong | HBM/ Cross-sectional study | Oral health behaviors, HBM constructs and dental anxiety | Stronger perceived susceptibility, greater severity of oral diseases, less performing of oral health behaviors and a higher score of DMFT were directly related to ↑ dental anxiety level. |
| Karimy et al, 2020, Iran [46] | 356 sixth-grade students at single sex primary schools in Saveh city. Intervention group received oral HE consisted of 4 one-hour sessions (180 experimental & 176 control) | TPB/ Pre-post intervention study | Action plan and coping plan constructs | Significant improvements were reported in Action and coping plan constructs in the Intervention arm compared to control. |
| Van et al, 2015, Belgium [37] | Parents of 1,057 children born ↔ October 2003 and July 2004 in two regions in Flanders. |
TPB/ Cross-sectional and prospective design over a 5-year interval |
Dietary habits, OH habits, dental attendance, and their psychological determinants based on TPB (attitude, subjective norms, PBC, intention) | Attitudes, subjective norms and PBC towards intention, and of intention and PBC towards frequency of consumption of sugared snacks and drinks, tooth brushing and dental attendance were reported to be significant associated with TPB |
| Bashirian et al, 2021, Iran [52] | 988 elementary school children in Hamadan city. Theoretical models were examined using structural equation modelling | SCT/ Cross-sectional study | brushing and flossing behaviors |
SCT explained 50% of variance in brushing with fluoridated toothpaste and 55.6% of variance in flossing behaviors; SCT, self-efficacy and family environment were strongly associated with brushing and flossing behaviors |
| Lin et al, 2019, China [44] | 20–45 years with PD; 158 & 139 patients as experimental group (EG) & control group (CG); Both groups received leaflet, EG also received brief one-on-one counselling session | TPB/ Randomized controlled trial | TPB measures | EG exhibited significantly higher levels of action and coping planning than the CG. |
| Kaur et al, 2017, India [45] | 200 children ↔ age groups of 4–8 years belonging to a public school and their mothers from Punjab; | SI/ Cross-sectional study | Relationship ↔ Mother’s Sense of Coherence (SOC) and Dental caries of children | Children caries gets influenced by mother’s SOC level. An inverse relationship ↔ mother’s SOC level and their children caries status. |
| Blake et al, 2015, United Kingdom [51] | 3 primary schools. 150 children (aged 9-12 years). Intervention. Children received a 60-minute theory driven classroom-based interactive educational session |
TPB/ Cohort study with pre-test –post-test design |
Oral health–related knowledge and self-reported oral health–related behaviors | Dental knowledge significantly improved following intervention; Significantly more children reported using dental floss 6 weeks after intervention compared with baseline |
| Dziaugyte et al, 2017, Canada [47] | 15- to 16-year-old adolescents from 4 public schools; 5 sessions were given for intervention group and one for control; 2 schools (n=112) in intervention and 2 schools (n=94) in control arm | Theory of Self-efficacy/ Cluster randomized trial | Oral self-care skills and oral self-care practice | Self-efficacy theory-guided intervention was superior to conventional dental instruction to improve oral self-care in adolescents |
| Coulson & Buchanan, 2002, United Kingdom [50] | 224 students undergraduate Psychology or Education |
TTM/ Cross-sectional study | Intention and behaviour in relation to dental check-ups | 13.7% precontemplation, 31.5% in contemplation, 8.2% in preparation, 39.3% in action 7.3% in maintenance phase. |
| Dumitrescu et al, 2014, Romania [35] | 172 first-year medical students at University of Medicine and Pharmacy ‘Carol Davila’ | HBM, TRA, TPB and motivational process of HAPA/Cross-sectional study | Toothbrushing, flossing, mouth rinsing | TPB and health action process approach were best predictor of intentions to engage in both behaviours. |
| Solhi et al, 2010, Iran [28] | 12-year-old girl students (n-291), central district of Tehran; 147 and 144 students (intervention and control arm). | HBM/ Quasi-experimental study | Perceptions, oral behaviors, OH and DMFT index | All oral health perceptions significantly increased; Correct brushing and flossing are influenced by ↑perceptions. |
| Abbasgholizadeh et al, 2019, Iran [27] | 170 pregnant women in city of Ardabil (85 each in intervention and control arm) | HBM/ Randomized controlled trial | Questions related Perceived sensitivity (7), severity (6), benefits (7), barriers (8), practical guide (10) self-efficacy (6). | Proportion of pregnant mothers who used dental flossing significantly improved after intervention. |
| Shamsi et al, 2013, Iran [26] | 21-35 years women with pregnancy; 130 pregnant women from health centers in Arak (65 each in intervention and control arm) | HBM/ Quasi-experimental study | Perceived susceptibility, Severity, benefits, barriers and oral health behavior | HBM Model variables scores were significantly ↑ in intervention group compared to controls |
| El-Maghawry et al, 2022, Egypt [25] | 100 pregnant women visiting Obstetrics and Gynecology Outpatient Clinic, Zagazig University Hospitals (50 each in intervention and control) |
HBM/ Quasi-experimental study | Perceived susceptibility, Severity, benefits, barriers, performance and cues to action related to oral health behaviors |
HBM-based education as teaching intervention positively affects oral health behavior of pregnant women in interventional group |
| He et al, 2023, China [15] | 70 patients (periodontitis proposed for implant restoration) with 35 each in Intervention and control arm; Routine OH was given to control and Intervention group received MI and routine care | MI based on TTM/ Randomized controlled trial | Oral cleaning behavior and periodontal health status | MI based on TTM can effectively improve oral cleaning behavior and periodontal health of implant-restored patients with periodontitis |
| Xiang et al, 2022, China [24] | 1184 students, 12 Schools, aged 13 years in Hong Kong, (6 schools with 587 students) or control groups (6 schools with 572 students) | HBM, SCT/ Cluster Randomized Controlled Trial | Brushing, flossing, oral health related quality of life (OHRQoL) after 6-month follow-up | Brushing, flossing, and OHRQoL improved more in experimental group than control group at |
| Sumita et al, 2022, Japan [23] | 748 underwent dental check-ups at Okayama University | HBM/ Cross-Sectional Study | Health belief model, absolute risk aversion, and willingness to undergo regular check-ups | Willingness undergo regular dental check-ups was associated with oral health behaviors and health belief model, but not with absolute risk aversion. |
| Buglar et al, 2010, Australia [22] | Public dental hospital (n = 80) and private dental clinic (n=12) | HBM/ Cross-Sectional Study | Brushing, Flossing | Partial support only was found for HBM with barriers emerging as sole HBM factor influencing brushing and flossing behaviours. Self-efficacy significantly predicted both OH behaviours |
| Syrjälä et al, 2001, Finland [69] | 149 patients’ insulin dependent IDDM at diabetes clinic of the Department of Internal Medicine, University Hospital of Oulu. | TRA/ Cross-Sectional Study | Frequency of tooth brushing, dental caries, HbA1c level and diabetes adherence | Firmer intention to brush teeth was related to a higher reported frequency of tooth brushing; e attitude to and subjective norm of tooth brushing were related to intention to brush |
| Rigau-Gay et al, 2018, Spain [17] | 106 orthodontic patients, 12-25 years, wearing fixed appliances in both arches. | TTM/ Cross-Sectional Study | PI and Gingival index | 2/3 of patients reported being at less advanced stages of change (63%), being most frequent stage preparation (40%) |
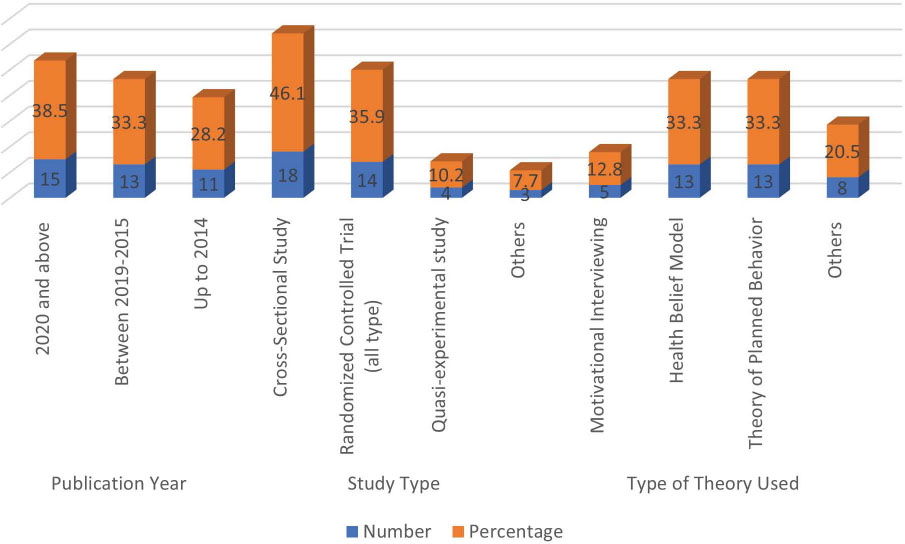
Characteristics of the studies in relation to publication year, type of the study and theory.
3.5. Health Belief Model
Twelve studies made use of the HBM to improve oral health in children, mothers, adolescents, or pregnant women [21-33]. Several studies have demonstrated that educational programs based on the HBM may be more effective than traditional methods in promoting optimal oral health practices among children and their parents. Implementing such interventions, particularly in school settings, has shown potential in preventing dental caries in school-aged children [21]. For example, Yekaninejad et al. (2012) reported improvements in oral hygiene behaviors following the introduction of an HBM-based program [33]. Similarly, Shahnazi et al. found that educational sessions significantly increased knowledge scores in the intervention group, leading to better oral health behaviors among mothers for their children [32].
Alhazmi et al. showed that the integration of oral health education into school and university curricula enhances awareness and preventive practices among Saudi youth [30]. Didactic interventions grounded in the HBM framework appear to encourage individuals to adopt and maintain proper oral hygiene routines, particularly in high-risk populations, such as pregnant women. Given their vulnerability, there is a recognized need for targeted and cost-effective preventive strategies, including community-based health education and prioritization of dental care before pregnancy [27]. Studies have shown that HBM-based educational interventions for pregnant women contribute to positive changes in oral health behaviors [25]. Overall, HBM-driven interventions have demonstrated effectiveness in improving oral health outcomes across various age groups and during pregnancy.
3.6. HAPA Intervention
The Health Action Process Approach (HAPA) is a theoretical framework designed to explore the mechanisms underlying health behavior change and the factors that influence it. Central to the model is the distinction between two phases of behavior change: the motivational phase, in which intentions are formed, and the volitional phase, which involves planning, action, and maintenance [34]. Two studies are included in this review; these studies provided detailed explanations of how HAPA affects oral health outcomes. Dumitrescu and colleagues (2014) evaluated how well several social-cognitive models could explain current health behaviors and predict future intentions regarding toothbrushing, flossing, and mouth rinsing. This study simultaneously measured the health belief model (HBM), theory of reasoned action (TRA), theory of planned behavior (TPB), and the motivational processes of the health action process approach (HAPA) using a sample of 172 medical students. The HAPA model incorporates susceptibility, severity, outcome expectancy, and self-efficacy. These factors accounted for an additional 27.5%, 43.2%, and 66.2% of the variance in intentions to brush teeth more often, floss more, and rinse more, respectively. Though the newest and least-studied model, this one has proven useful in predicting flossing habits [35]. In 2020, Scheerman and colleagues investigated the effectiveness of a theory-based program delivered via Telegram, an online social media platform, to improve oral hygiene among Iranian adolescents, using the HAPA as a framework. The study assessed psychosocial variables, toothbrushing practices, Visual Plaque Index scores (VPI), and Community Periodontal Index (CPI) scores. The study used HAPA factors to assess mediation effects on toothbrushing, finding that intention, self-efficacy, perceived social support, self-monitoring, and coping planning all significantly mediated the intervention's effect, suggesting a complex interplay influencing behavioral change. The study of Iranian adolescents shows that a theory-based online program, engaging both teens and their mothers via social media, significantly boosts the effectiveness of toothbrushing habits [36].
3.7. TPB, Salutogenic Theory, Self-efficacy Theory
This review includes 21 studies that examined the impact of the TPB, SCT, and self-efficacy theory on oral health outcomes [35-55]. The findings indicate that interventions grounded in TPB, self-efficacy theory, and salutogenic models, as well as those focused on preventive oral health education and promoting adherence to self-care behaviors, were associated with positive behavioral changes. The studies targeted both school-aged children and mothers, with several also considering contextual factors such as family environment and resource availability. Interventions based on TPB were particularly effective in influencing behavioral intentions and led to significant improvements in oral health practices.
4. DISCUSSION
To our knowledge, this is the first literature review to systematically explore a broad range of psychological models within the context of oral hygiene, offering a unique and valuable contribution to the field based on papers published till 2023.
Oral diseases remain among the most common chronic conditions globally despite being largely preventable. Traditional educational approaches have shown limited long-term effectiveness in changing oral hygiene behaviors. In recent years, several interventions based on behavior change theories are increasingly being used to improve oral health. In this literature review, we aimed to evaluate the behavioral theory-driven interventions aimed at improving oral health outcomes.
The search strategy revealed a total of 39 articles. Overall, the findings revealed significant improvements in oral healthcare practices when health behavior theories, particularly those grounded in the HBM, were implemented. These findings are consistent with those of Solhi et al., who reported improved oral health perception following an educational intervention based on the HBM [28]. Similarly, an independent study conducted in Iranian institutions observed significant improvements in community periodontal indices and oral hygiene, along with positive changes in all HBM constructs during the initial follow-up period [28]. Furthermore, Vichayanrat et al., investigated a multilevel oral health intervention informed by self-efficacy theory, HBM, and other behavioral models, and their findings support the structured development and evaluation of theory-based oral health programs [56].
A systematic review also confirmed the effectiveness of HBM in enhancing adherence to oral hygiene instructions among adults with periodontal disease [57]. Similarly, Ghaffari et al. also found that HBM-guided education can improve oral hygiene behaviors among their study population [58]. In line with the current review, the HBM framework appears to facilitate positive behavioral change by addressing key cognitive factors such as perceived susceptibility, perceived severity, perceived barriers, and self-efficacy. The HBM framework helps individuals understand the risk of developing oral disease and recognize the severity of the condition while enhancing their confidence in their ability to take preventive actions necessary to improve oral health [59]. The impact of HBM-based interventions was most pronounced during the early follow-up period. The difference between the intervention and control groups diminished over time. This decline suggests that health beliefs may shift, potentially reducing the long-term effectiveness of a single intervention. Such findings underscore the need for reinforcement strategies or booster sessions to maintain behavioral gains. These observations also highlight a distinguishing feature of the HBM when compared to other models that emphasize continuous engagement or social reinforcement.
An important finding of our study was that interventions based on the TPB led to significant improvements in oral health outcomes. Notably, the effectiveness of TPB-based interventions appeared to increase with longer follow-up durations, suggesting that behavioral intentions and changes are reinforced over time. Developed by Icek Ajzen, the TPB provides a framework for predicting and understanding human behavior across various contexts based on the premise that intention is the most immediate determinant of behavior. According to the theory, intention is influenced by three key constructs: attitude toward the behavior, subjective norms, and perceived behavioral control [60]. These elements collectively shape an individual's motivation to perform a specific health-related behavior. TPB has been widely applied in health promotion research and has consistently proven effective in enhancing understanding and influencing health behaviors [61].
Several studies included in this review highlight the relevance and predictive strength of the Theory of Planned Behavior (TPB) in oral health promotion. Dumitrescu et al. (2014) identified significant correlations between oral health knowledge, current behaviors, subjective norms, perceived behavioral control, intention, and attitude, reinforcing the comprehensive nature of TPB constructs in understanding oral health behavior [48]. Similarly, Daniel et al. found that attitude was the strongest predictor of toothbrushing frequency, with awareness, subjective norms, and perceived behavioral control also playing important roles [62].
Ebrahimpoiur et al. (2016) further supported the utility of TPB by demonstrating that a TPB-based intervention led to significant improvements in knowledge, attitudes, subjective norms, perceived control, and behavioral intentions within the intervention group compared to the control group [63]. Likewise, the study by Buunk-Werkhoven et al. confirmed that TPB variables accurately predicted oral health behaviors, suggesting the model’s applicability across diverse populations [64]. Christina et al. extended the TPB framework by showing that incorporating subjective norm–focused messaging could effectively influence individuals to schedule and attend dental appointments. Their findings underscore the importance of social influence and communication strategies in behavior change interventions.
Interventions based on the TPB theory were also more likely to improve the oral health of young adults. Studies based on TPB have shown that social expectations can significantly influence oral health in young adults [65, 66]. Even students who are consistent with their oral hygiene routines at home may experience changes in behavior when their environment shifts, such as moving into a dormitory. Factors including reduced privacy, changes in daily structure, or limited access to personal hygiene products can affect their ability to maintain these routines. Additionally, daytime fatigue may diminish motivation and energy levels, making it more difficult for students to brush and floss their teeth before going to bed [67].
The findings of our study indicated that psychological interventions based on the SCT did not result in significant improvements in oral hygiene, and the observed changes were not statistically significant. This contrasts with several previous studies that highlighted the effectiveness of SCT-based interventions in enhancing self-reported oral health behaviors and reducing plaque accumulation and gingival inflammation [68]. The discrepancy between our findings and those of earlier research may be attributed to differences in study design, population characteristics, or the degree of personalization in the intervention approach [69, 70]. As suggested in prior studies, dental behaviors and attitudes are shaped by a combination of cognitive processes, emotional factors, social support, and early life experiences, all of which can influence the success of behavior change interventions [69].
Self-efficacy has been independently identified as a significant determinant of oral health and hygiene among individuals with diabetes and older adults [70, 71]. Several factors may explain this association. Earlier research has often emphasized specific cognitive elements of the SCT while paying less attention to its environmental and contextual components, which are equally important in shaping health behaviors. Additionally, discrepancies in findings may be influenced by the duration of the intervention or follow-up periods. Although higher levels of self-efficacy have been consistently associated with improved oral hygiene behaviors, it is important to consider that these benefits may not be sustained over time. For example, Pine et al. (2000) observed significant improvements in self-efficacy in managing periodontal disease and oral hygiene status after six months of follow-up, suggesting that while gains are achievable, their long-term maintenance requires further investigation and ongoing support [72].
Overall, our findings indicate that improvements in periodontal health and oral hygiene status were observed for about six months after the intervention, suggesting that while behavioral gains are achievable, their long-term maintenance may require ongoing support and further investigation [72]. Studies have shown that other interventional behavioral theoretical frameworks, including range-frequency theory, communication strategies, and structured health behavior models such as the Wilson and Cleary model, can also enhance the overall effectiveness of oral health interventions. These interventions were more effective in older adults. This review also confirms earlier findings by Reisine et al., which showed that children whose mothers had a stronger external locus of control were more susceptible to dental caries [73]. Locus of control refers to the extent to which individuals believe that their health outcomes are determined by their own actions (internal) versus external forces such as chance, fate, or other people (external). These findings are consistent with the current analysis, which also observed that children with caregivers exhibiting an external LOC were at greater risk of poor oral health. The effectiveness of these interventions was further supported by improvements in clinical outcomes such as reduced dental plaque accumulation, decreased gingival tenderness, and lower incidence of gum bleeding.
This study has several strengths and limitations. In this literature review, we included studies from major medical databases such as PubMed, Scopus, and Cochrane, and assessed research published over a 23-year period to ensure a complete and comprehensive coverage of the existing literature. We also made use of broad inclusion criteria that allowed for the analysis of diverse populations and settings to improve the generalizability of the results. Adherence to PRISMA guidelines ensured transparency and rigor in the processes of study selection, data extraction, and synthesis. As a result, the review presents a strong evidence base supporting the effectiveness of behavior change theories such as HBM and TPB in improving oral health outcomes. Moreover, the findings emphasize the flexibility of these models in informing the development of targeted, context-specific interventions. These insights offer practical guidance for future research and support the implementation of more effective, theory-informed strategies in oral health promotion.
One of the primary limitations of this review is the variability in the methodological quality of the included studies, which may contribute to heterogeneity in the findings and affect the overall interpretation of the effectiveness of health behavior theories in oral health interventions. This variability arises from differences in study designs, sample sizes, and outcome measures, all of which can influence the consistency and comparability of results. Most studies focused on a limited set of well-established health behavior theories, with minimal exploration of newer or less conventional models that may also hold promise for influencing oral health behavior. This narrow focus may lead to the underutilization of emerging theoretical frameworks that offer innovative perspectives on behavior change. Additionally, the findings are largely based on self-reported data, which may not accurately reflect actual behavioral changes or clinical outcomes in oral health. Further research is required to examine the impact of providing targeted information to patients on compliance and outcomes. Future studies should prioritize the accurate measurement of oral health behaviors to facilitate comparison between strategies. Moreover, additional interventional studies grounded in newly established psychological theories are needed to strengthen the evidence base and increase confidence in the effectiveness of these approaches.
CONCLUSION
Integrating oral health interventions grounded in health behavior theories has the potential to enhance patient adherence and improve overall health outcomes. Interventions based on the HBM and the TPB demonstrated the most significant impact. However, the limited scope of the existing interventions may restrict the generalizability of current findings. Future research should focus on exploring a broader range of health behavior theories, comparing their effectiveness, and leveraging technological innovations to facilitate behavior change. Moreover, there is a need for more longitudinal studies to assess the long-term sustainability of behavior modifications resulting from these interventions. Dental health professionals should incorporate interventions based on behavior theories to boost patient engagement and ultimately contribute to better public health outcomes in oral care.
AUTHORS’ CONTRIBUTIONS
The author confirms sole responsibility for the following: M.S.: Study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| OH | = Oral Hygiene |
| AUDs | = Alcohol Use Disorders |
| MI | = Motivational Interviewing |
| HAPA | = Health Action Process Approach |
| HBM | = Health Belief Model |
| TPB | = Theory of Planned Behavior |
| TPA | = Theory of Planned Action |
| SI | = Salutogenesis Theory |
| TRA | = Theory of Reasoned Action |
| TTM | = Transtheoretical Model |
| SCT | = Social Cognitive Theory |
| HE | = Health Education |
| PBC | = Perceived Behavior Control |
| DMFT | = Decayed, Missing, and Filled Teeth |
| SOC | = Sense of Coherence |
| ↔ | = Between |
| BI | = Bleeding Index |
| PI | = Plaque Index |
| ↑ | = Increased |
AVAIALABILITY OF DATA AND MATERIALS
All data supporting the findings of this study are available from the corresponding author [M.S] upon reasonable request.
ACKNOWLEDGEMENTS
We would like to thank TopEdit (www.topeditsci.com) for the English language editing of this manuscript.

