All published articles of this journal are available on ScienceDirect.

The Influence of Impacted Mandibular Third Molar in Health-related Quality of Life
Authors Info & Affiliations
Abstract
Background
Quality of Life (QoL) is defined as “a person's view of their status in life, shaped by the cultural and value systems surrounding them, along with their goals, expectations, standards, and worries.” The literature lacks information supporting the effect of impacted third molars on Oral Health-Related Quality of Life (OHRQoL). Impacted third molars could affect the function of mastication, which consequently affects quality of life.
Aim
This study aimed to evaluate the impact of impacted third molars on oral health quality using the Oral Health Impact Profile (OHIP-5) questionnaire.
Materials and Methods
A cross-sectional study was conducted to investigate the effect of impacted third molars on Oral Health-Related Quality of Life (OHRQoL). The participants were interviewed using an Arabic version of the Oral Health Impact Profile with five items (OHIP-5).
Results
In 148 participants aged 19 to 70 years, the Oral Health Impact Profile (OHIP) score indicates that participants with impacted teeth had higher scores than the control group (no impaction), with a statistically significant p-value of less than 0.05. This confirms the effect of third molar impaction on quality of life.
Conclusions
Impacted third molars significantly affect OHRQoL due to pain, infections, functional and aesthetic issues, psychological stress, economic pressures, and accessibility to care. Examining these factors is crucial for developing strategies to mitigate their negative effects. Proper management can enhance the well-being and quality of life of those impacted.
1. INTRODUCTION
Quality of life is defined as “an individual's perception of their life situation based on the values and cultures of the society in which they live as well as their objectives, expectations, standards, and worries [1]. The term quality of life was first introduced in 1920 by a British economist. Since then, the definition of quality of life has been further expanded to include the medical and dental fields [2]. A person's oral health (OH) is a critical indicator of their general health as well as a direct correlation between their overall health and their oral health-related quality of life (OHRQoL) [3]. Moreover, several researchers proposed that an individual's overall health-related quality of life is associated with their perception of how several sets of factors, such as functional aspects, psychological factors, social factors, and pain and discomfort experiences, affect their well-being [4]. It has been determined that all children, adults, and dentate elderly people display the same level of OHRQoL when they are evaluated with the OH impact profile (OHIP) questionnaire [5]. In dentistry, impacted teeth are defined as those that can not and do not reach a functional position.
The third molars are the most commonly impacted teeth, the last permanent teeth to emerge into the oral cavity. Key contributors to tooth impaction include insufficient space, restricted skeletal development, larger crown dimensions, and delayed maturation of third molars [6]. Third, molar impaction is categorized using the Pell & Gregory classification method based on its depth level relative to the second molar's occlusal surface vertically in classes A, B, and C and Position A. The highest portion of the third molar is on a level with the occlusal plane, Position B. The highest portion of the tooth is between the occlusal plane and the cervical line of the second molar, Position C. The highest portion of the tooth is on a level with the cervical line of the second molar and its relationship to the Ramus body horizontally in classes I, II, and III. Class I impactions refer to situations in which adequate space exists between the ramus and the distal aspect of the second molar to accommodate the mesiodistal diameter of the third molar. Class II impactions refer to instances in which the spatial distance between the distal aspect of the second molar and the ramus of the mandible is smaller than the mesiodistal diameter of the third molar. Class III impactions occur when the third molar is predominantly located in the ramus of the mandible (Pell and Gregory, 1933).
The prevalence of tooth impaction has been assessed across various populations. A recent study conducted in Yemen revealed that third molar impaction is more frequent in males and primarily affects the mandibular arch. Additionally, the angulation and severity of impaction seem to be more intricate in the maxillary arch [7]. Another study in the UAE revealed that class II, level B, and mesioangular impactions are the most common patterns of impaction [7]. Numerous other studies have evaluated teeth impaction across different populations, showing a higher incidence of third molar impaction in the mandible compared to the maxilla and in females compared to males [7].
The literature reported that the prevalence of impacted third molars in Riyadh City was 58.3% [7]. A retrospective study was conducted in Jeddah, Saudi Arabia, to evaluate the most frequent angles of the third molar based on Winter's classification among 768 patients. Based on their findings, the most prevalent angulation in mandibular third molars was mesio-angular (41.8%), followed by horizontal (32.6%), vertical (23.9%), and the least common was distoangular (1.6%) [8]. According to a study carried out in the central region of Saudi Arabia, there is a high rate of third molar impaction. There is no gender predilection, as it more frequently occurs in the maxilla than the mandible. Most of the patients were referred to the clinic for elective asymptomatic reasons.
In most cases, mesio-angular impaction is found in the mandible, whilst vertical angulation is usually found in the maxilla. It has been determined that both arches have a depth of C level and a class I Ramus relationship [7]. In addition, a study in the Asir Region of Saudi Arabia found that tooth impaction is more prevalent in the maxilla than the mandible, with a higher incidence of third-molar impaction in males than females [6]. A recent systematic review found that females exhibited a greater prevalence of canine impactions than males. Furthermore, canine impactions were more prevalent in the maxilla than the mandible, with a higher frequency noted on the left than on the right side [6].
There are various symptoms for impacted third molars, which include Jaw pain or swelling, bleeding of the periodontal tissues, unpleasant breath or taste, and difficulty in mouth opening. All these symptoms could lead to a negative influence on the OHRQoL. However, there is a lack of information available in the literature on the effect of third molar impaction on the OHRQoL. Therefore, our study aimed to quantify the effect of impacted third molars on quality of life using (OHIP-5). Based on the clinical observation and literature review about the signs and symptoms of impactions, we hypothesized that third molar impaction would negatively affect the quality of life.
2. MATERIALS & METHODS
This cross-sectional study investigates the effects of horizontal and mesioangular impacted third mandibular molars on the quality of life among adult dental patients who visited university dental hospitals in Umm Al-Qura University and Taibah University from March to June 2023. The ethical approval was obtained from the Institutional Review Board (IRB) at Umm al-Qura University with reference number (HAPO-02-K-012-2023-02-149), and all participants provided informed consent and were fully debriefed. All the participants were in good health and were classed as (American Society of Anesthesiologists Risk Classification I). They were also at least 18 years old and free of significant periodontal disease (American Academy of Periodontology I, II). Patients with acute pericoronal infections were excluded. Patients with systemic disorders such as diabetes, immunological compromise, bleeding diathesis, and dyspepsia were also excluded from the study. The (OHIP-5) (Table 1) was completed for each participant,
| Q1- Have you had difficulty chewing any foods because of problems with your teeth, mouth, dentures, or jaw? | Never | Hardly ever | Occasionally | Fairly often | Very often |
| Q2- Have you had painful aching in your mouth? | Never | Hardly ever | Occasionally | Fairly often | Very often |
| Q3- Have you felt uncomfortable about the appearance of your teeth, mouth, dentures, or jaw? | Never | Hardly ever | Occasionally | Fairly often | Very often |
| Q4- Have you felt that there has been less flavor in your food because of problems with your teeth, mouth, dentures, or jaw? | Never | Hardly ever | Occasionally | Fairly often | Very often |
| Q5- Have you had difficulty doing your usual jobs because of problems with your teeth, mouth, dentures? | Never | Hardly ever | Occasionally | Fairly often | Very often |
and the responses were recorded on a 5 Likert scale: “A technique for the measurement of attitudes” ranging from never to very often (score is 0 to 4). After calculating the total score of all domains, the higher score indicates poor OHRQoL, and the lower score indicates good OHRQoL [9].
Data were collected at a dental teaching hospital during patient registration. Each patient underwent a comprehensive dental exam conducted by trained dentists using a dental mirror, explorer, and orthopantomogram X-ray (OPG). In addition, to address uncertainties, bitewing X-rays were taken as necessary. The full-mouth examinations assessed all teeth and surfaces for decay, missing teeth, fillings, sound teeth, or pulpal involvement, along with evaluating pain, swelling, abscesses, or oral pathology. Clinical records were reviewed, and dental health indicators were collected from dental records. Orthopantomographs were examined to determine whether the oral cavity had third permanent molars. This clinical and radiographic examination was followed by the study questionnaire that takes 3-5 minutes to complete.
The questionnaire was written in Arabic (Arabic version of the OHIP-5 questionnaire (Table 1). The questionnaire had a short introduction describing the purpose of the study and ensuring that the patient’s responses would be confidential. The participants were required to complete all sections of the questionnaire, and questionnaires were to be filled out entirely. The first section of the questionnaire was regarding patients’ demographic characteristics. The demographic data (Fig. 1) collected were (gender, nationality, level of education, age, and socio-economic indicators). The second section (Table 1) included questions about (difficulty chewing, painful aching, discomfort about appearance, less flavor in food, and difficulty doing usual jobs).
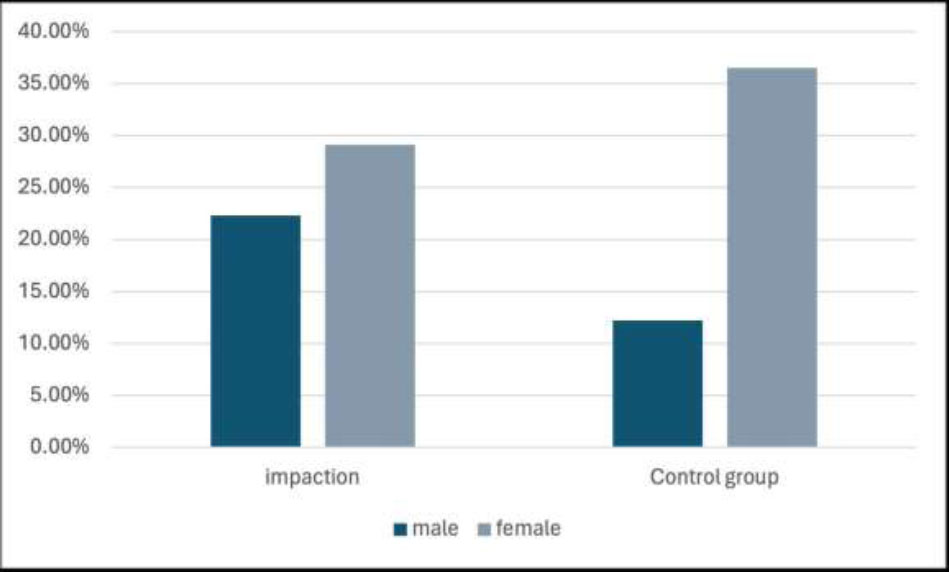
Demographic data compare the proportions of males and females between the third molar impaction group and the control group. The X-axis represents the demographic categories, and the Y-axis shows their respective proportions. Dark blue represents males, and gray represents females.
Demographic characteristics and oral health-related quality-of-life profiles were summarized using descriptive statistics. The primary outcome, total OHIP-5, was calculated by summing responses across all five items, yielding scores from 0 to 20, where higher scores indicate a more significant negative impact on oral health-related quality of life. A sample size of 124 (62 per group) achieves 80% power to detect a mean of differences of 0.2 with an estimated standard deviation of differences of 0.9 and with a significance level (alpha) of 0.05 and effect size = 0.253 using a two-sided student t-test. All statistics were calculated using STATA software (version 14.1; Stata, College Station, Tex), with two-tailed tests interpreted at the 0.05 significance level. Participation was voluntary and private, with permission to use the data granted through responses to the questions [10, 11].
3. RESULTS
A total of 148 participants (76 with an impacted third molar tooth and 72 as a control group) were registered in the screening clinic between March and June 2023. The participants ranged in age from 19 to 70. Female participants with third molar impaction constituted 29.1% of the sample, female participants as a control group constituted 36.5%, male participants with third molar impaction constituted 22.3%, and male participants as a control group constituted 12.2% of the sample.Regarding each question in the (OHIP-5) questionnaire (Table 1), For Question 1 (Q1), the third molar impaction group had a mean score of 25.0. In contrast, the control group had a mean score of 22.4, indicating a greater frequency of chewing difficulties among those with impacted third molars (p < 0.05). For Q2, the third molar impaction group had a mean score of 16.8 compared to 14.4 in the control group, reflecting more frequent experiences of pain (p < 0.05). For Q3, the mean score was 15.2 in the third molar impaction group and 14.6 in the control group (p < 0.05), suggesting that impacted third molars affect patients' comfort with their dental appearance. However, both Q4 and Q5 showed no significant difference between the third molar impaction group and the control group.
The total scores were calculated by summing all domains of (OHIP-5); the higher the score, the more negative impact on the OHRQoL, and the lower the score, the less negative impact on the OHRQoL. When all five items were used to compute summary scores (Figs. 2-4), there was a tendency for the percentage reporting that the third molar impaction group was higher than the control group. 35.1% of subjects with impacted third molar reported OHIP score > 0. The OHIP mean score for the participants with impacted teeth was 3.3 (SD, 3.7), and the control group was 2.2 (SD, 2.6). p-value <0.05 showed a significant difference, confirming the effect of impacted third molars on the QoL.
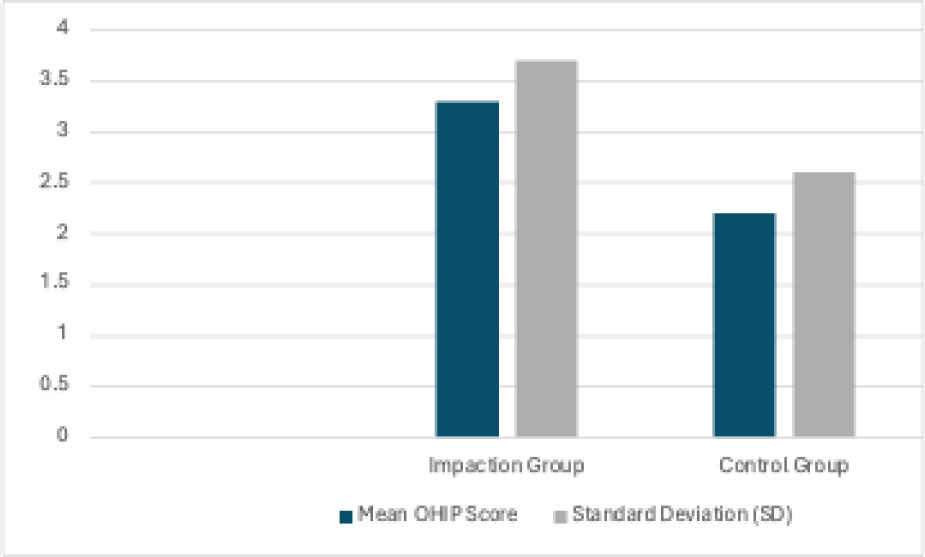
This figure presents the mean Oral Health Impact Profile (OHIP) scores and standard deviation (SD) for both the third molar impaction group and the control group. X-axis: The two study groups, Impaction Group and Control Group. Y-axis: OHIP-5 scores, measuring the impact of oral health on quality of life. A higher score indicates poorer OHRQoL. Dark blue bars: Mean OHIP scores for each group. Gray bars: Standard deviation SD, representing variability in responses within each group.
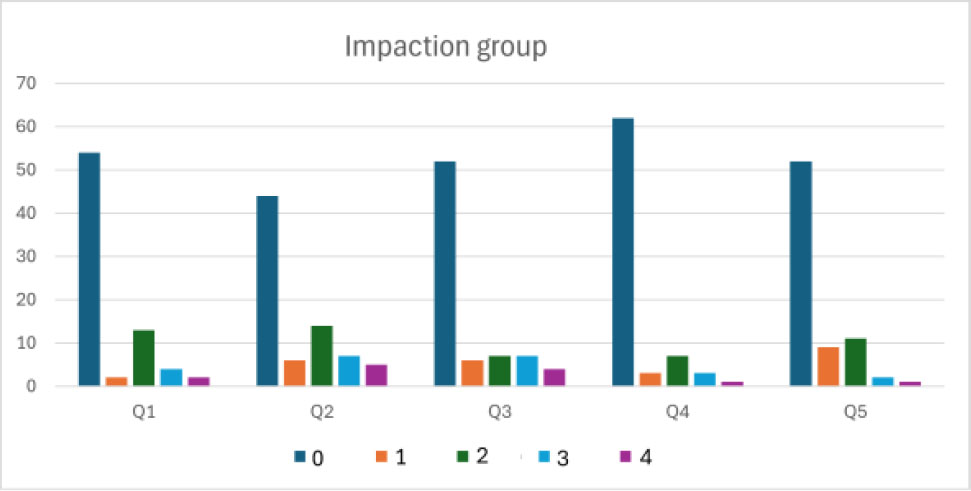
Total responses to the five questions for the impaction group. Y-axis = Total response on a 5 Likert scale. X-axis = 5 Questions and their answer ranging from never to very often (score is 0 to 4). After calculating the total score in each domain, The higher score indicates poor OHRQoL and the lower score indicates good OHRQoL.
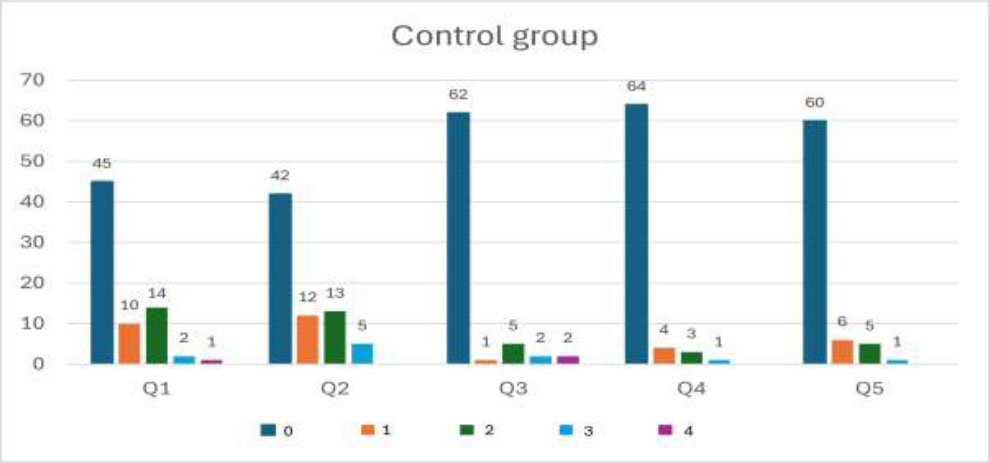
Total responses to the five questions for the control group. Y-axis = Total response on a 5 Likert scale. X-axis = 5 Questions and their answer ranging from never to very often (score is 0 to 4). After calculating the total score in each domain. The higher score indicates poor OHRQoL and the lower score indicates good OHRQoL.
4. DISCUSSION
This study aimed to examine the impact of impacted third molars on the quality of life. The literature demonstrates a lack of information on the effects of the third molar impact on Oral Health-Related Quality of Life (OHRQoL). An overall of 148 patients were interviewed. Participants were divided into two groups, one with impacted third molars and the other without impacted third molars. Consent forms were obtained, and participants were interviewed using the Arabic version of the Oral Health Impact Profile with five items (OHIP-5). Our findings show that patients with third-molar symptoms, such as pain and swelling, adversely affect their quality of life.
The statistical significance of these differences was tested using independent t-tests. Significant differences (p<0.05) for Q1, Q2, and Q3 indicated that impacted third molars considerably worsened OHRQoL in these domains. According to Q4 and Q5, third molar impaction does not significantly impact taste perception and job performance. Additionally, the total QoL score for the control group ranged from 0 to 11. In contrast, the total QoL score for the impacted group ranged from 0 to 14, highlighting a higher total score for the third molar impaction group. This data suggests that the symptoms associated with impacted third molars have a broader and more significant negative impact on patient's quality of life.
This study’s results do not represent all patients in Makkah and Madinah who may experience third-molar symptoms. This study's results are clinically relevant in informing patients about the effects on quality of life that can be expected if they choose to keep their third molars and what to expect if they develop third-molar symptoms. One drawback of (OHIP-5) is that it is not specific, and the impact of oral health on quality of life can be expected due to other oral disorders, such as dental caries on the same side of the impacted third molar. One way to assess whether the pain was because of an impacted third molar or other dental diseases is to remove the third molar, assess the OHRQOL after surgery, and compare it to previous data. We expect to observe improvements in OHRQoL after the post-surgery recovery period.
Some limitations of our present study may include the restricted sample selected, which was only from two Dental Hospitals. Furthermore, the type of questionnaire used (OHIP-5) was well-rounded enough to reflect the actual effect of impacted third molars on health-related quality of life. However, a more comprehensive questionnaire could provide additional data. Moreover, this study was limited to impacted third molars and the extent of their impact on health-related quality of life. Other confounding factors may have been present among the sample participants, potentially negatively affecting their health-related quality of life.
CONCLUSION
Our findings show that in patients with third molar symptoms, their quality of life is adversely affected. These findings highlight that impacted third molars significantly worsen the oral health-related quality of life (OHRQoL). Third molar impaction resulted in a greater frequency of chewing difficulties (p < 0.05), more frequent experiences of pain (p < 0.05), and affected patients' comfort with their dental appearance. However, the overall negative impact on taste perception and daily job performance is less pronounced. The clinical significance of these findings highlights the importance of surgical intervention in these cases to alleviate the negative consequences of teeth impaction. Moreover, it is significant to investigate the factors related to third molars that affect OHRQoL to minimize their unfavorable effect. Further investigations are also required to expand these results and generalize the conclusion.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| QoL | = Quality of Life |
| OHRQoL | = Oral Health-Related Quality of Life |
| OHIP | = Oral Health Impact Profile |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the Institutional Review Board (IRB) at Umm al-Qura University, Saudi Arabia with reference number (HAPO-02-K-012-2023-02-149).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [A.B] upon reasonable request.
ACKNOWLEDGEMENTS
We thank all the participants who contributed their valuable time to this study. The authors declare no competing financial interests.

