All published articles of this journal are available on ScienceDirect.

Differences in Niti and Glide Path Rotary System: Preparation of Canal Centering and Transportation in Double-curved Root Canals
Authors Info & Affiliations
Abstract
Background
The primary goal of root canal preparation is to eliminate infected pulp and necrotic tissue within the root canal to facilitate the healing of periapical lesions. Shaping and cleaning are critical success factors in endodontic treatment. The complexity of root canal anatomy makes shaping difficult, which raises the risk of procedural errors and insufficient disinfection.
Objective
This study aimed to evaluate the differences between Niti rotary systems with glide paths on centering and transportation of double-curved root canals.
Methods
Thirty-six stained double-curve resin root canal samples were divided into six groups (n=6), Proglider+M3 Pro Gold, Proglider+Protaper Gold, Proglider+Protaper Ultimate, Protaper Slider+M3 Pro Gold, Protaper Slider+Protaper Gold, and Protaper Slider+Protaper Ultimate. Glide paths were created using ProGlider (PG) and ProTaper Slider (PS) prior to further preparation to an apical size of 25, using three different rotary continuous systems: M3 Pro Gold (M3PG), ProTaper Gold (PTG), and ProTaper Ultimate (PTUlt). Images were taken before and after treatment for superimposition. Measurements were taken using concentric circles at 1 mm intervals. Perpendicular lines were drawn from the prepared surface to define ten measurement points.
Results
Significant differences in centering ability were observed at points 2 and 6 (p < 0.05). At point 2, significant differences were found between the PG+M3PG group and the PG+PTUlt group, as well as between the PG+PTUlt group and the PS+M3PG group. At point 6, significant differences were observed between the PG+PTUlt group and the PS+M3PG group. Significant differences in canal transportation were found at points 0, 2, and 9 (p < 0.05). At point 2, significant differences were found between the PG+M3PG group and the PG+PTUlt group, as well as between the PG+PTUlt group and the PS+M3PG group. At point 9, significant differences were observed between the PG+M3PG group and the PG+PTUlt group. All systems exhibited canal transportation, and none demonstrated perfect centering ability.
Conclusion
The Protaper Slider+M3 Pro Gold combination showed better centering ability compared to Proglider+Protaper Ultimate in two-thirds of the root canal. When used with ProGlider, the M3 Pro Gold system demonstrated better prevention of canal transportation in the apical third compared to ProTaper Ultimate but showed inferior performance in the coronal third. M3 Pro Gold can be a good choice in curved root canals, while both Protaper Gold and Protaper Ultimate can be a good choice in straight root canals or calcified root canals.
1. INTRODUCTION
Root canal preparation is fundamentally designed to remove infected pulp and necrotic tissue in the root canal, thereby promoting the healing of pre-existing periapical lesions or preventing infection of periradicular tissues [1, 2]. Both conventional and modern endodontic instrumentation aim to thoroughly eliminate microorganisms and tissue debris by enlarging the canal to an adequate size, facilitating a root canal shape that allows a three-dimensional seal [3, 4]. The process of shaping and cleaning contributes to the success of endodontic treatment and is closely linked to disinfection and filling procedures [4].
Straight and uncurved root canals are rarely observed, as the majority of teeth display some degree of curvature in their root canals, with many showing multiple curvatures [5]. Zhang defined a double-curved root canal as one with more than one curvature, each exceeding 10 degrees. Yan et al. reported that 2.7% of double-curved root canals were found in the Western Chinese population [6]. The intricate anatomy of root canals increases the difficulty of shaping, potentially resulting in inadequate disinfection and procedural errors [7]. Dentin removal during root canal treatment poses the risk of straightening the root canal, eliminating curvature and ledge formation [8].
The primary goal of root canal instrumentation is to achieve preparation that maintains the root canal anatomy, ensuring that the foramen remains as small as possible without deviating from the natural canal curvature [9]. Various techniques and instruments have been developed to minimize canal straightening and root canal transportation [10]. Canal centering is an instrument’s ability to remain in the canal’s center during preparation, indicating that dentin removal in the area that has been prepared by the instrument is evenly distributed [11, 12]. Apical root canal transportation refers to the removal of the root canal wall structure on the outer curve of the apical half of the root canal due to the file’s tendency to return to its original shape during canal preparation [13]. This can result in the accumulation of debris and microorganism residues due to inadequate root canal cleaning and potential procedural errors such as zipping, ledging, or perforation. Wu et al. suggested that apical transportation exceeding 0.3 mm can reduce the sealing ability of filling materials and adversely impact treatment outcomes [14].
A glide path is defined as an unimpeded pathway from the canal orifice to its physiological ends, serving as the pathway for shaping files [15, 16]. Glide path preparation can be performed manually with stainless steel K-files or using rotary instruments [17]. However, K-files have disadvantages, including technique sensitivity, risks of canal transportation, alteration of the original canal anatomy, and increased debris extrusion [18]. Rotary glide path preparation, on the other hand, offers advantages such as reduced instrumentation time, better preservation of canal anatomy, decreased operator fatigue, and minimized apical debris extrusion [19].
Nickel-titanium (NiTi) rotary files have emerged as better tools for glide path creation [17]. The Proglider (PG) was launched in 2014, followed by the introduction of the Protaper Ultimate Slider (PS) in 2022. Both instruments utilize M-wire technology [20, 21]. Notably, PS features a shorter active area, fewer blades, and a parallelogram cross-section, whereas the Proglider is characterized by a square horizontal cross-section [15].
Rotary NiTi instruments have improved the efficiency of root canal shaping, outperforming stainless steel in flexibility and cutting efficiency, all while preserving canal geometry [22]. Gold treatments were introduced in 2014 when Dentsply Maillefer launched ProTaper Gold™ (PTG), an M-Wire instrument that undergoes a post-grinding heat treatment process. PTG system (Dentsply Maillefer, Ballaigues, Switzerland) is a heat-treated gold instrument, which is heat-treated after the file is made. PTG has convex triangular cross-sections, shaping files with progressive taper and finishing files with variable taper. This system includes 3 shaping files (#19.04, #18.02, dan #20.04) dan 3 finishing files (#20.07, #25.08, and #30.09]) [23, 24].
The Protaper Ultimate™ (PTUlt) system (Dentsply Maillefer, Ballaigues, Switzerland) represents a more recent innovation in gold heat-treated instruments. The shaping files have progressive tapers, starting at 5.5% at D4, increasing to 6% at D8, and then decreasing to 4.7% at D12 and 1.7% at D16. These files have cross-sections of 85° parallelogram from D0 to D8, and gradually increase to 80° parallelogram at D8 to D10 and remain at 80° from D10 to D16. Finishing files in this system exhibit specific taper profiles. F1 has a fixed taper of 7% from D0 to D3, which reduces to 6.5% at D4 and gradually decreases to 3.5% at D16. F2 tapers from 8% to 7%, then to 6.5% at D4, and further narrows to 3.3% at D16. F3 tapers from 9% to 8% [24, 25].
M-wire contains 508 Nitinol, which has been thermomechanically treated with specific temperature and tensile stress. M-wire is not completely austenite phase but has small amounts of martensite and R-phase depending on its manufacturing process [26]. M-wire exhibits higher flexibility, greater resistance to cyclic fatigue, and better mechanical properties compared to conventional NiTi [27, 28].
In 2018, United Dental Group, Shanghai, China, introduced the M3 Pro Gold (M3PG) system, which is a heat-treated gold Control Memory wire (CM wire) file. It has a non-cutting tip and a convex triangular cross-section. This system includes 5 files (#17.08, #20.04, #25.04, #25.06, dan #35.04). Control Memory Wire (CM-Wire) is NiTi with a lower nickel content (52%) compared to conventional NiTi. CM-Wire is preferred as a rotary instrument over conventional NiTi. It offers enhanced flexibility and resistance to cyclic fatigue while lacking the superelasticity of conventional NiTi [29].
Currently, there is a lack of research that directly compares the efficacy of the three leading systems, M3PG, PG and PTUlt, in terms of their ability to maintain canal centering and prevent root canal transportation. This study aimed to evaluate the capability of the aforementioned three systems after making a glide path using PG and PS in preserving canal centering and preventing root canal transportation.
2. MATERIALS AND METHODS
2.1. Sample Preparation
This study utilized samples in the form of acrylic blocks with double-curved canals ISO#10, 0.02-tapered (Dentsply Maillefer, Ballaigues, Switzerland). The double-curved canals had a 30° coronal curve and a 20° apical curve [2, 15, 30-32].
2.2. Sample Size Calculation
To determine the sample size in this experimental research, the sample size was obtained from the calcluation using the Lemeshow formula. The average for each group (0.37 and 0.29) and the standard deviation (± 0.0316) used were obtained from previous research with a similar study design by Neto et al. [33] Based on the calculation results, the minimum number of samples for each group tested is 5 samples. The number of samples in this study is 6 samples.
2.3. Photographic Procedures
Pre-preparation and post-preparation images of the samples were taken under standardized conditions for distance, angle, and background using a DSLR camera (EOS 700D, Canon Inc., Japan) with a 100 mm macro lens (100 mm, Canon Inc., Japan). To enhance color contrast, all canals were injected with blue ink (Snowman, Seiko Seisakusho Co., Ltd., Japan) before instrumentation.
2.4. Root Canal Preparation
The double-curved endodontic blocks were explored using a #10 K-file with a watch-winding motion (15–30°) until the working length was reached and randomly divided into six groups (n = 6) as follows (Table 1):
| Group | Glidepath | Rotary System | n |
|---|---|---|---|
| 1 | ProGlider | Protaper Gold | 6 |
| 2 | M3 Pro-Gold | 6 | |
| 3 | Protaper Ultimate | 6 | |
| 4 | Protaper Ultimate Slider | Protaper Gold | 6 |
| 5 | M3 Pro-Gold | 6 | |
| 6 | Protaper Ultimate | 6 |
2.4.1. Group 1
PG and PTG group. Glide path was created using PG followed by preparation with PTG file.
2.4.2. Group 2
PG and M3PG group. Glide path was created using PG followed by preparation with M3PG.
2.4.3. Group 3
PG and PTUlt group. The glide path was created using PG, followed by preparation with the PTUlt file.
2.4.4. Group 4
PS and PTG group. The glide path was created using PS, followed by preparation with a PTG file.
2.4.5. Group 5
PS and M3PG group. The glide path was created using PS, followed by preparation with an M3PG file.
2.4.6. Group 6
PS and PTUlt group. The glide path was created using PS, followed by preparation with the PTUlt file.
The preparation used 3 types of rotary systems depending on the test group up to size #25 using an endomotor (X-Smart Endodontic Motor, Dentsply Sirona, USA) and continuous motion until the working length was reached. Irrigation with 2 mL of distilled water was carried out between each file change, with a distance of 2 mm from the apical foramen via a 30-gauge side-vented needle syringe, then dried using a paper point.
The pre- and post-preparation images were combined and superimposed. Measurements were taken using concentric circles at 1 mm intervals. Perpendicular lines were drawn from the prepared surface to define 10 measurement points (Fig. 1A-C). Image contrast, color, and sharpness were adjusted, and measurements were taken to determine differences in the inner and outer canal walls, as well as the canal diameter after preparation at each reference line. This study was conducted using Adobe Photoshop CS6 (Adobe System Inc, USA) and Digimizer (Medcalc Software Ltd, Belgium) to measure the transportation and centering of each group.
2.5. Analysis of Centering Ability and Canal Transportation
The shaping ability of the systems was evaluated quantitatively by the following method [31]:
• Root canal transportation was calculated using the formula = (X1-X2). Positive results indicated transportation to the outer side of the apical curve. Negative results indicated transportation to the inner side of the apical curve.
• The ability of the root canal centering was calculated using the formula = (X1-X2) / Y. Centering ability closer to zero means perfect centering.
X1 is the resin prepared on the outer wall, and X2 is the resin prepared on the inner wall, Y is the final diameter of the root canal after instrumentation (Fig. 2).
2.6. Statistical Analysis
Statistical analyses were conducted using SPSS (version 26, Chicago, IL, USA). The normality test was assessed with the Shapiro-Wilk test, and homogeneity was tested using Levene’s test. The data tested was normally distributed, and one-way ANOVA was used to compare the means value of the 6 groups in 10 measurement points. Homogeneous data were further analyzed with Post Hoc Tukey to compare the means value of each group in 10 measurement points. The level of significance was set at p<0.05 for all tests. (Suppl. material, Appendix 1).
3. RESULTS
3.1. Canal Transportation
Transportation data analysis was conducted using a one-way ANOVA test. The results indicated significant differences between groups at points 0, 2, and 9 (p<0.05), so a post-hoc Tukey test was performed (Fig. 3). The post-hoc test at point 0 revealed significant differences between the PG+PTG group and the PG+PTUlt group. At point 2, significant differences were found between the PG+M3PG group and the PG+PTUlt group, as well as between the PG+Ult group and the PS+M3PG group. At point 9, significant differences were observed between the PG+M3PG group and the PG+PTUlt group. The results of the post-hoc test on transportation between other groups at other points did not show significant differences (Table 2).
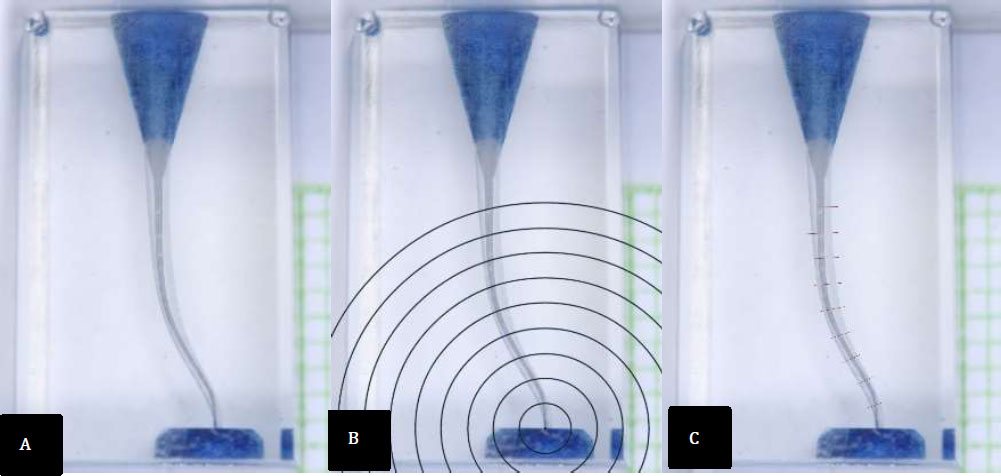
The creation of 10 measurement points process using Adobe Photoshop CS6. (A) Images combined and superimposed. (B) Concentric circles at 1 mm intervals. (C) Perpendicular lines were drawn from the prepared surface.
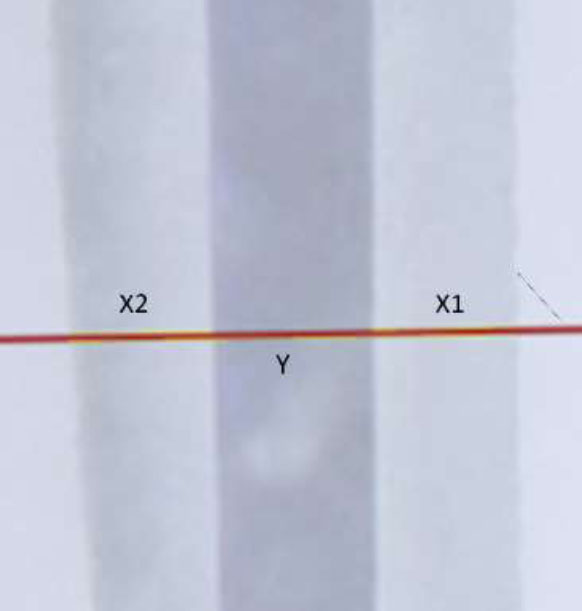
Line of measurement. (X1) the resin prepared on the outer wall. (X2) the resin prepared on the inner wall. (Y) the final diameter of the root canal after instrumentation.
| Point of Measurement | Group | PG+PTUlt | |
|---|---|---|---|
| Point 0 | PG+PTG | Mean diff. | -0.081333 |
| Sig. | 0.008* | ||
| Point 2 | PG+M3PG | Mean diff. | 0.111000 |
| Sig. | 0.003* | ||
| PS+M3PG | Mean diff. | 0.093333 | |
| Sig. | 0.015* | ||
| Point 9 | PG+M3PG | Mean diff. | 0.111667 |
| Sig. | 0.022* | ||
3.2. Canal Centering
Data analysis for centering was also conducted using a one-way ANOVA test. The results showed significant differences between groups at points 2 and 6 (p<0.05), thus a Tukey post-hoc test was performed (Fig. 4). The post-hoc test at point 2 showed significant differences between the PG+M3PG group and the PG+PTUlt group, as well as between the PG+PTUlt group and the PS+M3PG group. At point 6, significant differences were observed between the PG+PTUlt group and the PS+M3PG group. No significant differences were identified between other groups at other points (Table 3).
| Point of Measurement | Group | PG+PTUlt | |
|---|---|---|---|
| Point 2 | PG+M3PG | Mean diff. | -0.211 |
| Sig. | 0.007* | ||
| PS+M3PG | Mean diff. | 0.1965 | |
| Sig. | 0.014* | ||
| Point 6 | PS+M3PG | Mean diff. | -0.167833 |
| Sig. | 0.025* | ||
4. DISCUSSION
The primary objective of root canal preparation is to remove infected pulp tissue and necrotic tissue in the root canal. Another critical aspect is maintaining the original shape of the root canal while preserving healthy root dentin, ensuring a good long-term prognosis [2]. The process of shaping and cleaning are essential to the success of endodontic treatment, as they directly impact disinfection and filling procedures [4]. The complex anatomy of root canals makes shaping challenging, increasing the risk of inadequate disinfection and procedural errors such as canal transportation, ledges, zipping, and perforations [2]. Changes in the root canal morphology are often linked to unfavorable treatment outcomes [19].
The increased flexibility of NiTi instruments has contributed to shorter treatment times and reduced procedural errors, including zipping ledges and canal transportation. NiTi instruments have undergone various modifications, including heat treatments, to enhance their elasticity, flexibility, and resistance. NiTi alloys exhibit three distinct microstructural phases: austenite, martensite, and R-phase, depending on temperature. Austenitic NiTi is strong and rigid, while martensitic and R-phase NiTi are soft, elastic, and malleable. Thermomechanical treatment can stabilize the alloy in the martensitic phase, R-phase, or a mixed phase by changing transformation temperatures, thereby modifying the alloy’s characteristics [34, 35]. The gold color of Gold heat-treated instruments results from the heat treatment applied to the alloy and the titanium oxide layer that coats the instrument’s surface. This titanium oxide layer has a thickness of 100–140 nm [2, 27].
This study utilized three different types of gold-treated NiTi instruments. The M3PG system (United Dental Group, Shanghai, China) is a gold heat-treated file made of CM wire with a non-cutting tip and a convex triangular cross-section [29]. The PTG system (Dentsply Maillefer, Ballaigues, Switzerland) is also a gold heat-treated instrument, with heat treatment applied after the file is manufactured. PTG has a progressive taper and a convex triangular cross-section [24]. The PTUlt system (Dentsply Maillefer, Ballaigues, Switzerland) is a recently introduced gold heat-treated instrument. Its Shaper and Finisher files have an off-centered
The instrument has a parallelogram cross-section, while the other instruments in the system retain a convex triangular cross-section [25].
The final diameter of the files used in this study is size #25. Akhlaghi et al. reported that the size #25 files did not show a significant difference in bacterial reduction compared to files with larger apical diameters [36]. However, Buchanan et al. stated that as the apical diameter increases, the risk of root canal transportation also rises [37].
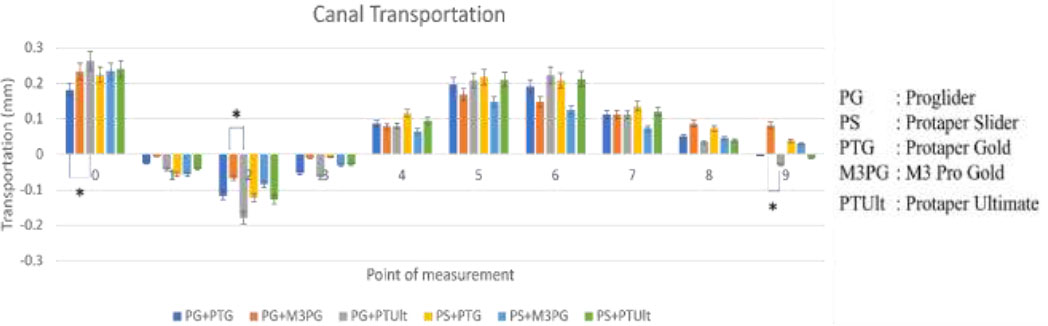
Mean value of canal transportation after instrumentation with different types of glide path and NiTi system. Note: (*) significant (p<0.05).
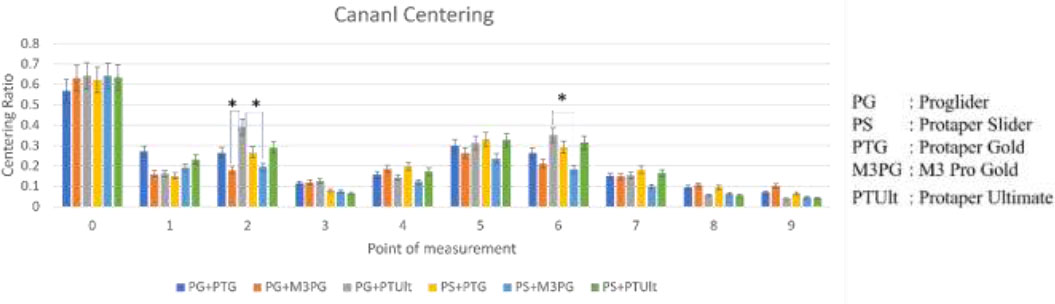
The mean value of centering ratio after instrumentation with different types of glide path and NiTi systems. Note: (*) significant (p<0.05).
Glide path files facilitate the enlargement of the root canal, improving shaping efficiency [31]. Recently introduced rotary NiTi files have proven to be more efficient and effective for creating glide paths. This study utilized two different glide-path files, PG and PS. PG is a rotary instrument made with M-wire technology and features a square horizontal cross-section. PS shares similarities with PG in tip size, surface finish, and helix angle. However, the PS has a shorter active area, fewer flutes, and a parallelogram cross-section, distinguishing it from the PG [15].
The superimposition method was used in this study to evaluate the shaping ability of each file group. This method was chosen due to its validity based on the body of evidence [31]. This study used double-curved endodontic blocks (#10.02, Dentsply Maillefer, Ballaigues, Switzerland). Acrylic resin blocks are validated experimental models for analyzing root canal preparation, offering standardized curvatures, and facilitating imaging before and after treatment [32, 38].
Extracted teeth were not selected in this study due to their non-standardized dentin hardness and irregular anatomy, which would hinder repeatable testing [30]. However, acrylic resin blocks have a limitation: the heat generated during preparation can soften the resin, increasing the risk of instrument fracture. Irrigation was performed after each file change, and recapitulation with a #10 file was conducted to reduce heat and clear resin debris [15]. Root canal transportation exceeding 0.3 mm is considered detrimental to the prognosis of root canal treatment. In this study, all groups exhibited canal transportation; however, none exceeded the 0.3 mm threshold [39].
This study found that the PTG file combined with PG was significantly better at preventing root canal transportation than the PTUlt file with PG at point 0. This aligns with findings from the study conducted by Sharawy et al., who reported that PTG caused less root canal transportation in the apical third compared to PTUlt [31]. The M3PG file used with PG was significantly better at preventing transportation than PTUlt with PG at point 2; however, its performance was inferior at point 9. This is the first study to compare these files in terms of root canal transportation, and the differences between these two files can be attributed to variations in their alloy type, taper, tapering design, and cross-sectional shapes. PTUlt uses M-wire alloy, while M3PG uses CM-wire alloy. These findings are consistent with research by Biradar et al. and Kishore et al., who found that CM-wire files produced less transportation in the apical and middle thirds of the root canal compared to M-wire files [40, 41]. McSpadden et al. stated that instruments with greater flexibility are less likely to cause transportation [41]. This is supported by the statement of Pongione et al, that CM-wire has superior flexibility and resistance to cyclic fatigue compared to other superelastic NiTi technologies [42]. Additionally, Oh et al. observed that CM-wire retains almost 45º of curvature after being bent and released, whereas M-wire exhibits spring-back behavior after the external force is removed [43-45].
A smaller taper of .06 on the M3PG file may explain its superior ability to prevent root canal transportation in the apical third. Schafer et al. reported that increasing taper reduces instrument flexibility, thereby increasing the likelihood of root canal transportation [46]. On the other hand, the reduced taper from D4 to D16 in the PTUlt file may be the reason for its advantage in preventing transportation in the coronal third compared to the fixed taper of M3PG. In the three groups utilizing PS for glide-path preparation, no significant differences were observed across all measurement points compared to other groups.
Regarding the centering ratio, the M3PG file with PS demonstrated better centering ability than PTUlt with PG at points 2 and 6. While the centering performance of these two files has not been compared before, differences in alloy type, taper size, tapering design, and cross-section likely contribute to the variation. M3PG uses CM-wire alloy, while PTUlt uses M-wire alloy. These findings align with studies by Biradar et al. and Kishore et al., which found that CM-wire demonstrates superior centering ability in the apical and middle thirds of the root canal compared to M-wire [40, 41]. Oh et al. stated that CM-wire is better suited for curved root canals, while gold-treated M-wire performs well in straight or calcified canals [45]. This is attributed to the ability of CM-wire to adapt to root canal anatomy effectively, although it has a lower maximum torque load compared to M-wire [43]. The differences in glide path used in the two groups may also influence the results, as the two glide path instruments used have distinct cross-sectional designs. To date, no studies have compared the maximum torque load and cyclic fatigue of M3PG, PTG, and PTUlt files.
In this study, the use of acrylic resin has a limitation in the form of differences in hardness compared to natural teeth. Therefore, future studies can build on this research by using samples from natural teeth.
CONCLUSION
This study found significant differences in canal centering and root canal transportation. The M3PG file with PS demonstrated significantly better centering ability compared to PTUlt with PG in two-thirds of the root canal. Moreover, the M3PG file with PG showed significantly better performance in preventing root canal transportation than PTUlt with PG in the apical third of the root canal. However, in the coronal third, the performance of the M3PG file with PG was less favorable. In conclusion, M3PG can be a good choice in curved root canals, while PG and PtUlt can be a good choice in straight root canals or calcified root canals.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper: C.R., W.W., T.A.: Study conception and design; C.R.: Data collection; C.R., W.W.. T.A., S.R.L.: Analysis and interpretation of results; C.R., W.W., T.A., S.R.L.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| NiTi | = Nickel Titanium |
| PG | = ProGlider |
| PS | = ProTaper Slider |
| M3PG | = M3 Pro Gold |
| PTG | = ProTaper Gold |
| PTUlt | = ProTaper Ultimate |
| NiTi | = Nickel-titanium |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo Repository at https://zenodo.org/, reference number 10.5281/zenodo.15377361.
ACKNOWLEDGEMENTS
Declared none.

