All published articles of this journal are available on ScienceDirect.

Influence of Glide Path on Apically Extruded Debris in Curved Root Canals During Root Canal Preparation Using Three Different Single-file Instrumentation Systems with Improved Alloy Technology: An In Vitro Study
Abstract
Background
The apically extruded debris (AED) is an unwanted complication during root canal preparation, especially in curved canals.
Purpose
This study aimed to assess the impact of the glide path on the quantity of AED during root canal preparation with three different single-file systems with improved alloy technology in extremely curved canals.
Materials and Methods
One hundred and twenty maxillary first molar teeth with mesiobuccal root curvature (25°-45°) were randomly assigned to six groups (n=20). No glide path was created in three groups, whereas in the remaining three groups, a glide path was established in the mesiobuccal canals. Root canal instrumentation of the mesiobuccal canals was performed using three single-file systems: Reciproc Blue (RCB), WaveOne Gold (WOG), and TruNatomy (TN). AED was collected in pre-weighed Eppendorf tubes, which were subsequently stored in an incubator at 37 °C for two weeks. The weight of the dry extruded debris was determined by subtracting the pre-instrumentation weight from the post-instrumentation weight of the Eppendorf tubes. Statistical analysis was conducted using the Kruskal-Wallis test followed by Dunn’s post-hoc test with Holm correction (p<0.05).
Results
RCB and WOG without glide path extruded significantly more debris than other groups (p<0.05). The canal preparation required significantly less time in teeth with a glide path than the teeth without a glide path (p<0.05).
Discussion
Glide path preparation enhances shaping efficiency and significantly reduces apically extruded debris, especially in curved canals. The results of this in vitro study, along with existing literature, support the incorporation of glide path preparation into routine protocols to improve clinical outcomes. These findings may be translated into clinical practice to enhance endodontic treatment predictability and safety.
Conclusion
Within the limitations of this in vitro study, all tested instruments caused debris extrusion. A glide path significantly reduced the amount of AED and the preparation time. TN files extruded less debris compared with RCB and WOG.
1. INTRODUCTION
Patient-related factors, such as preoperative pain, occlusal trauma, microbial virulence, and operator-related variables, influence postoperative pain [1]. Shaping, cleaning, and obturation are the three main phases of root canal treatment. While all these phases are closely interrelated, shaping the root canal system is often considered the most critical step in endodontic therapy, as it directly impacts the effectiveness of the cleaning and obturation processes [2]. During root canal shaping, debris—including dentin particles, pulp tissue, microorganisms, and irrigants—can be extruded beyond the apical foramen, resulting in apically extruded debris (AED).
AED during root canal procedures can have significant clinical implications, primarily due to its association with postoperative pain, inflammation, and delayed periapical healing. The extrusion of debris can trigger an inflammatory response, potentially leading to postoperative discomfort and complications. Several studies have highlighted these concerns. For instance, research indicates that apical extrusion of debris is an inherent occurrence during root canal treatment and can lead to undesirable consequences such as postoperative pain and delayed periapical healing [3]. Scientific literature emphasizes that extrusion of debris may induce postoperative pain and inflammation, potentially inhibiting periapical healing [1, 4, 5].
The quantity of AED varies depending on the specific design features and material properties of rotary file systems, such as cross-sectional shape, flute depth, kinematics, and alloy composition [6, 7]. Although instrument cross-section and kinematics play an essential role, a glide path may reduce AED during canal preparation [8-11]. West defined the glide path as a consistent and smooth pathway extending from the root canal's orifice to its physiological endpoint, i.e., the apical terminus [12]. Furthermore, the same author quoted about the glide path, “its minimal size should be a ‘super loose No. 10 endodontic file’, and “The glide path must be discovered if already present in the endodontic anatomy or prepared if it is not present. The glide path can be short or long, narrow or wide, essentially straight or curved” [12]. During glide path preparation, coronal pre-flaring and canal enlargement reduce the curvature-related difficulty level of instrumentation, minimizing the risk of AED and helping prevent procedural errors such as instrument separation, shaping mishaps, and taper lock [13-15].
Minimizing AED is, therefore, a critical objective in modern endodontics, as it can reduce the incidence of postoperative complications and promote favorable healing outcomes [16]. Research suggests that the choice of instrumentation system and the use of a glide path can influence the amount of debris extruded apically. A well-established glide path has been shown to enhance instrument control, reduce resistance during canal shaping, and contribute to a smoother cutting action, ultimately limiting the amount of debris forced beyond the apical foramen [17]. By integrating techniques and systems that minimize AED, clinicians can lower the risk of postoperative discomfort and enhance patient-centered outcomes in endodontic therapy.
An engine-driven NiTi rotary PathFile (Dentsply, Maillefer, Ballaigues, Switzerland), launched in 2009, was the first rotary instrument specifically designed to produce an initial mechanical glide path [18]. The purpose of introducing the rotary PathFile was to eliminate the need for more rigid manual stainless-steel files to create glide paths. The instrument has a square cross-section with 0.02 taper and three different tip sizes: ISO 13, 16, and 19. Because of superior metallurgy, unique cross-section, and physical characteristics such as shape memory, the PathFile is less prone to procedural errors [19]. The manufacturer recommends using the initial PathFile directly after a No. 10 hand K-file has been employed to explore the root canal to its full working length.
Reciproc Blue (RCB; VDW Dental, Munich, Germany), which is a single-file shaping system, was designed as an advanced version of the M-wire Reciproc (VDW Dental) system, with enhanced resistance to cyclic fatigue. The instrument is subjected to a proprietary heat treatment that forms a blue titanium oxide layer on its surface [20].
WaveOne Gold (WOG, Dentsply Sirona, Charlotte, NC) is a single-file shaping system fabricated from M-wire. Its characteristic gold appearance is due to the repeated heating and cooling of the raw wire. The file features a multi-tapered design along its length and an off-centered parallelogram-shaped cross-section [20]. It operates using a reciprocating motion with a 170° counterclockwise (CCW) cutting action and a 50° clockwise (CW) motion. The system is available in four sizes: Small (size 20, 0.07 taper), Primary (size 25, 0.07 taper), Medium (size 35, 0.06 taper), and Large (size 45, 0.05 taper).
A recently introduced heat-treated NiTi instrument, TruNatomy (TN; Dentsply Sirona, Charlotte, NC), is developed using a uniquely thin NiTi wire featuring a flute diameter of a maximum of 0.8 mm, as opposed to the conventional 1.2 mm found in other file systems [20]. Additionally, it has an off-centered cross-section featuring a parallelogram shape, enhancing debris removal efficiency. The system comprises five specific instruments. It has been suggested that TN can maintain canal anatomy and tooth structure, particularly in extremely curved canals, because of its reduced shape memory, regressive slim taper, and NiTi alloy, which has undergone specialized heat treatment [21, 22].
Despite advancements in NiTi instrumentation, limited research has compared the performance of single-file systems in curved canals (25°–45°), particularly regarding apically extruded debris (AED) and preparation time. Most studies focus on straight canals, overlooking the impact of severe curvature and glide path preparation on shaping efficiency and debris extrusion. Reciproc Blue (RCB), WaveOne Gold (WOG), and TruNatomy (TN) utilize different NiTi alloys and motion kinematics, yet their comparative performance in curved canals remains unclear. RCB and WOG employ reciprocating motion, which may influence debris extrusion differently than TN’s continuous rotation. Additionally, TN’s slim NiTi wire and regressive taper may enhance dentin preservation and debris removal. This study addresses this gap by evaluating the effect of glide path preparation on AED and preparation time across these three instrumentation systems in curved canals, providing insights into optimal instrument selection for complex endodontic cases.
According to our knowledge, no study has directly compared the root canal preparation time and the amount of AED produced by the aforementioned single-file endodontic instrumentation systems in extremely curved canals. Consequently, this study was designed to assess the influence of glide path on preparation time and AED during root canal preparation in curved canals using single-file instrumentation systems with improved alloy technology (RCB, WOG, and TN).
The null hypothesis tested was that no significant difference would be observed in the quantity of apically extruded debris or the canal preparation time among the evaluated root canal instrumentation systems with and without glide path preparation.
2. MATERIALS AND METHODS
2.1. Sample Selection and Preparation
The study protocol was approved by the Committee of Research Ethics, Deanship of Graduate Studies and Scientific Research, Qassim University, Saudi Arabia (registration no. 24-08-04). This study included 120 mesiobuccal roots of maxillary first molar teeth extracted due to periodontal reasons. The included teeth had mesiobuccal canal curvature ranging from 25° to 45° and less than 6mm radius, as verified using image analysis software (AxioVision 4.5; Carl Zeiss Vision, Hallbergmoos, Germany) [23, 24].
The range of 25°–45° was selected based on Schneider’s classification, where moderate to severe canal curvatures pose significant instrumentation challenges, including an increased risk of canal transportation, instrument fatigue, and apical debris extrusion [23, 25]. This curvature range is clinically relevant, as it represents difficult anatomies where glide path preparation and file system selection play a crucial role in shaping the efficiency and amount of AED [26].
The root surfaces of selected teeth were debrided, and the samples were then submerged in a 1% sodium hypochlorite solution at 4°C for 24 hours and stored in a saline solution [27]. Digital periapical radiographs were taken, and the teeth with anatomic irregularities, root defects, canals with calcifications, and Vertucci type II configurations were excluded. Grouping the teeth following canal radius and curvature angle ensured a balance between the groups. Teeth were randomly distributed into six groups (n = 20) using the computer software (https://www.random.org). The sample size (n = 20 per group) was determined based on previous in vitro studies evaluating apically extruded debris and preparation time in endodontic instrumentation research. This sample size is commonly used in similar studies to ensure statistical reliability while maintaining feasibility [17, 28-30]. While formal power analysis is not commonly applied in laboratory-based studies, the chosen sample size was sufficient to detect significant differences among groups. The mean curvature angle value was 29.4071°± 5.01147, with a radius of 4.06031±0.91025 mm. The homogeneity of radii and curvature angles (p = .997 and p = 1.03, respectively) was evaluated by an analysis of variance.
Using water as a coolant, a high-speed handpiece and bur (Diatech, Coltene Whaledent, Altstätten, Switzerland) were used to section the molar teeth in the furcation area, separating the mesiobuccal roots. Access cavities were prepared for endodontic access, and the crowns of teeth were flattened to obtain a uniform working length of 19 mm. The patency of root canals was confirmed under 20X magnification using a Zumax OMS2350 operative microscope (Zumax Medical Co, Ltd, Jiangsu, China). After the investigator could see the tip of the file from the apical foramen, the file length was calculated, and 1 mm was subtracted from this length to obtain the final working length. Only teeth with an apical diameter less than or equal to size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) were included.
2.2. Collection of Debris
We used an experimental model similar to the one previously described by Myers and Montgomery, with modifications suggested by Kfir et al. [31, 32]. Pawar et al. used the modified version of this model in their experiment to assess AED during root canal shaping of primary teeth [5]. Eppendorf tubes were used to collect the extruded debris during root canal instrumentation. An electronic microbalance (AUW-220D; Shimadzu, Tokyo, Japan) with a 0.00001 g precision was used to weigh each tube individually five times before the experiment started. The mean weight values were recorded for each tube. Eppendorf tubes were placed into the glass vials. A round hole was created in the silicone rubber cap of the vial. Each root specimen was put into the silicone rubber cap inside the Eppendorf tube up to the cementoenamel junction and was fixed with flowable composite (Filtek Supreme; 3 M ESPE, St Paul, MN, USA) to prevent the leakage of the irrigant externally. The air pressure inside the tubes was maintained comparable to the outside by inserting a 27G irrigating needle (NaviTip; Ultradent Products, South Jordan, UT) through the rubber stopper. The Eppendorf tubes were fitted into glass vials to prevent contamination during root canal preparation. To secure and stabilize each Eppendorf tube, we used silicone impression material (Coltène/Whaledent AG, Altstätten, Switzerland) to form a small holding mold at the base of the vial. This setup ensured that the root tip remained inside the Eppendorf tube without making contact with its walls.
To prevent the operator from being able to view the debris extrusion during root canal preparation, we covered the vials using a rubber dam (Coltene Hygenic ® Dental Dam Coltene/Whaledent GmbH, Altstaetten, Switzerland) (Fig. 1).
2.3. Root Canal Instrumentation
Straight-line access was performed for all the specimens. Following this, six groups of specimens were formed. In groups 1, 2, and 3, a glide path was prepared to the working length following the manufacturer’s instructions using PathFiles (P1, P2, and P3). In groups 4, 5, and 6, no glidepath was prepared.
2.3.1. Group 1 (n=20)
Instrumentation of the root canals using Reciproc Blue (RCB; VDW, Munich, Germany): After glide path preparation, we used a Reciproc R25 (25/.08) file in the “Reciproc All” mode. Instrumentation was done following manufacturer instructions. We used a slow in-and-out pecking motion to operate the file. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
2.3.2. Group 2 (n=20)
Instrumentation of the specimens using WaveOne Gold (WOG; Dentsply Maillefer): After Glide path preparation, the WOG primary file (size 25, 0.07 taper) was used with the “WaveOne All” mode of a VDW silver endodontic motor (VDW, Munich, Germany). The manufacturer's instructions were followed, and the file was used with a slow in-and-out pecking motion until the working length was reached. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
2.3.3. Group 3 (n=20)
Instrumentation of the specimens using TruNatomy (TN; Dentsply Sirona, Charlotte, NC): After Glide path preparation, a TN prime file (26/.04) was used at 500 rpm speed and 1.5Ncm torque. Instrumentation was done following manufacturer instructions. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
2.3.4. Group 4 (n=20)
Instrumentation of the root canals using Reciproc Blue (RCB; VDW, Munich, Germany): We used a Reciproc R25 (25/.08) file in the “Reciproc All” mode. Instrumentation was done following manufacturer instructions. The file was operated in a slow in-and-out pecking motion. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
2.3.5. Group 5 (n=20)
Instrumentation of the specimens using WaveOne Gold (WOG; Dentsply Maillefer): the WOG primary file (size 25/ 0.07 taper) was used with the “WaveOne All” mode of a VDW silver endodontic motor (VDW, Munich, Germany). The manufacturer's instructions were followed, and the file was used with a slow in-and-out pecking motion until the working length was reached. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
2.3.6. Group 6 (n=20)
Instrumentation of the specimens using TruNatomy (TN; Dentsply Sirona, Charlotte, NC): a TN prime file (26/0.04) was used at 500 rpm speed and 1.5Ncm torque. Instrumentation was done following manufacturer instructions. The canal was irrigated, and the instrument’s flutes were cleaned with gauze after every three pecks.
Root canal preparation in all specimens was performed using suction (high vacuum). Irrigation was performed using 10mL bi-distilled water with a 27 G side-vented needle (NaviTip; Ultradent Products, South Jordan, UT) placed up to 2mm short of the working length. During instrumentation, the patency of the canal was verified using a size 10 K-file.
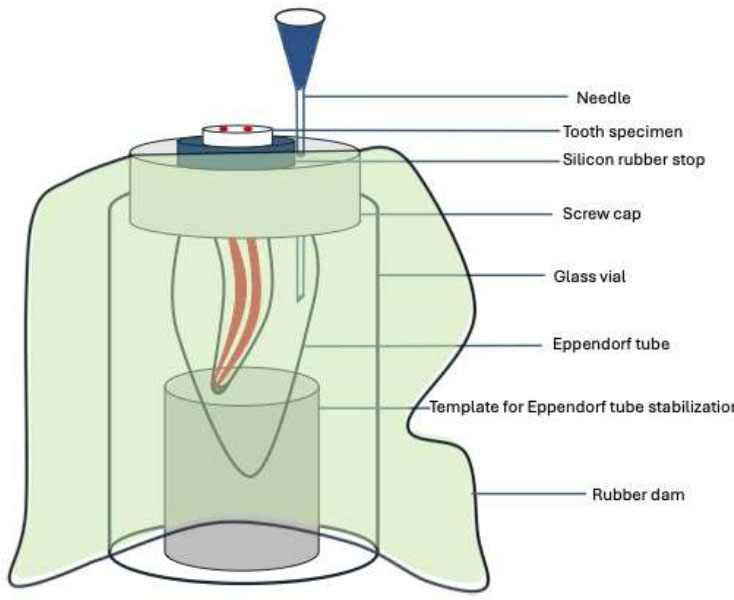
Schematic illustration of the experimental setup demonstrating the placement of extracted teeth in Eppendorf tubes, secured with silicone rubber caps, to isolate extruded debris.
2.4. Evaluation of Debris Extruded Apically
Specimens were removed from the Eppendorf tubes, and debris accumulated on the external surface of the root tip was washed into the tube with 1 mL of bi-distilled water. The tube containing the irrigation solution was placed in an incubator at 37°C for two weeks to allow the solution to evaporate. Subsequently, five additional weight measurements were taken for each tube, and the mean value was computed. The actual weight of extruded debris was obtained by calculating the difference between before and after instrumentation mean weight values in grams. In all teeth, the root canal instrumentation was performed by a single operator. A second examiner, blinded from the groups in the experiment, assessed the apically extruded debris.
2.5. Evaluation of Preparation Time
The time spent in glide path preparation and root canal shaping and cleaning was recorded by an assistant using a digital timer. The time spent in irrigation, recapitulation, cleaning of instrument flutes, and changing of instruments was also recorded. Finally, for each tooth, the total root canal preparation time in minutes and seconds was recorded.
2.6. Statistical Analysis
Data was statistically analyzed using IBM SPSS 29.0 software (IBM Corp, Armonk, NY). After confirming that data does not have a normal distribution (Shapiro-Wilk test (p < 0.05), analysis was conducted using the Kruskal-Wallis test, followed by Dunn’s post-hoc test with Holm correction at a 5% significance level.
3. RESULTS
The mean and standard deviation values of the apically extruded debris for all groups are shown in Table 1. All instrumentation systems generated AED (Fig. 2).
| Group | n | Mean (g) ± SD |
|---|---|---|
| Reciproc Blue | 20 | 0.01071 (0.00025) a |
| WaveOne Gold | 20 | 0.00913 (0.00068) a |
| TruNatomy | 20 | 0.00063 (0.00061) b |
| Glide Path+ Reciproc Blue | 20 | 0.00058 (0.00041) b |
| Glide Path+ WaveOne Gold | 20 | 0.00062 (0.00033) b |
| Glide Path+ TruNatomy | 20 | 0.00057 (0.00028) b |
The Kruskal-Wallis test revealed a significant difference (p < 0.05) in AED among the groups. Dunn’s post-hoc test with Holm correction indicated that Reciproc Blue (RCB) and WaveOne Gold (WOG) without a glide path extruded significantly more debris than all other groups (p < 0.05). No statistically significant differences were found among the remaining groups (p > 0.05).
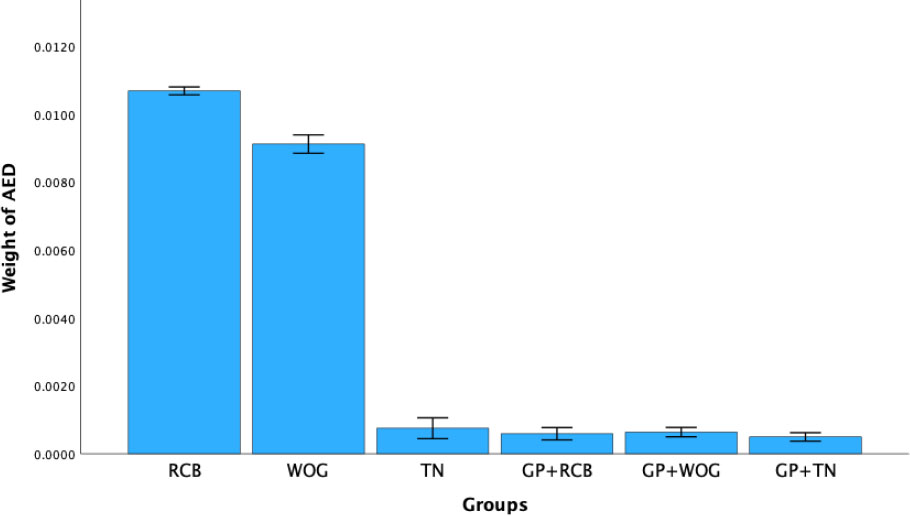
Mean weight (in grams) of apically extruded debris (AED) across instrumentation groups. Error bars represent 95% Confidence Intervals (CI). Abbreviations: RCB = Reciproc Blue; WOG = WaveOne Gold; TN = TruNatomy; GP = Glide path; AED = Apically extruded debris; RCB = Reciproc Blue; WOG = WaveOne Gold; TN = TruNatomy; GP = Glide path; AED = Apically extruded debris.
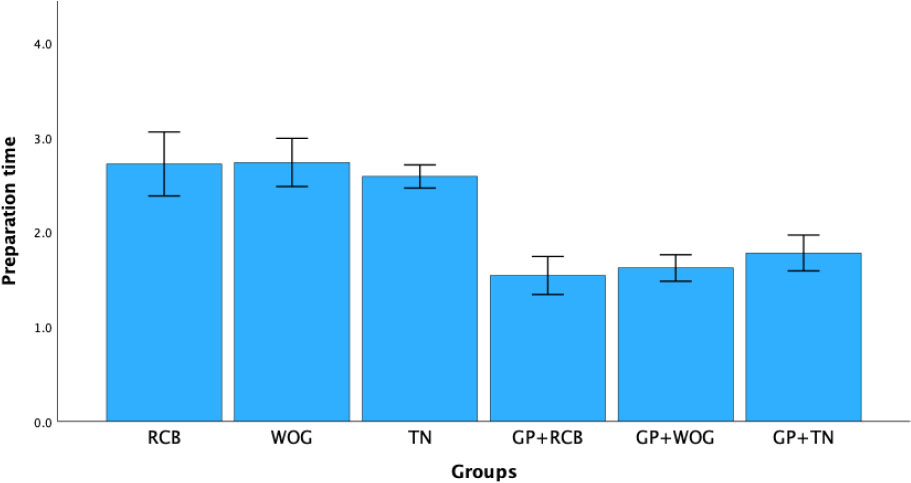
Mean preparation time (in minutes and seconds) across instrumentation groups. Error bars represent 95% Confidence Intervals (CI). Abbreviations: RCB = Reciproc Blue; WOG = WaveOne Gold; TN = TruNatomy; GP = Glide path; AED = Apically extruded debris; RCB = Reciproc Blue; WOG = WaveOne Gold; TN = TruNatomy; GP = Glide path; AED = Apically extruded debris.
Table 2 and Fig. (3) present the canal preparation time for each group. The Mann-Whitney U test showed that the presence of a glide path significantly reduced preparation time compared to groups without a glide path (p < 0.05). However, no significant difference in preparation time was found among the tested systems within the glide path and non-glide path groups (p > 0.05).
| Group | n | Mean ± SD |
|---|---|---|
| Reciproc Blue | 20 | 2.581 (0.682) a |
| WaveOne Gold | 20 | 2.598 (0.561) a |
| TruNatomy | 20 | 2.735 (0.361) a |
| Glide path + Reciproc Blue | 20 | 1.518 (0.401) b |
| Glide path + WaveOne Gold | 20 | 1.616 (0.394) b |
| Glide path + TruNatomy | 20 | 1.802 (0.386) b |
4. DISCUSSION
The null hypothesis was rejected, as all groups extruded debris in varying amounts, and the canal preparation time was different among the tested single-file instrumentation systems with and without glide path preparation. This study examined three distinct single-file instrumentation systems to assess the amount of AED and the time required for root canal preparation in curved canals, both with and without creating a glide path. We included the newer TruNatomy system due to the limited amount of literature comparing it with other systems that use different motion types. Furthermore, there is a significant lack or complete absence of research comparing the TruNatomy file system to other rotary systems, mainly when the presence or absence of a glide path is considered in extremely curved canals [2].
When prepared, the glide path preserves the canal's natural anatomy and reduces the risk of iatrogenic errors such as root perforation, apical transportation, and ledge formation [19, 33]. Such procedure-related mishaps are not uncommon in canals with severe curvature [34]. Despite the manufacturers of single-file NiTi systems proposing that the clinical protocols for these systems do not necessitate the preliminary creation of a glide path before their use in canal preparation [26], Ni-Ti instruments exhibit improved performance in the presence of a glide path [35]. We tested Reciproc Blue, WaveOne Gold, and TruNatomy.
Variations in dentine microhardness values and the absence of pulpal tissues are limitations associated with laboratory-based studies evaluating debris extrusion. The former condition is associated with more debris extrusion than in vivo, and the latter condition affects the results because of the difference in the density of the root canal space [3]. We used bi-distilled water for canal irrigation to avoid the likely crystallization of sodium hypochlorite after the separation of the irrigant during its evaporation procedure [36]. To avoid the irrigant and debris absorption and resultant debris quantification-related errors, we did not simulate the resistance of periapical tissue with floral foam [26].
All instruments extruded debris in this study. The TruNatomy files extruded significantly less debris than Reciproc Blue and WaveOne Gold in canals without a glide path. The results of the present study are in agreement with Abduljalil et al., who assessed the apically extruded debris associated with several contemporary endodontic instrumentation systems (TruNatomy, 2Shape, Protaper Next, WaveOne Gold, and Reciproc Blue) in single-rooted teeth with straight canals [37]. They concluded that the TruNatomy extruded significantly the least amount of debris apically. Their results indicate that Reciproc Blue causes significantly more debris extrusion than WaveOne Gold and TruNatomy. Our results are consistent with Kharouf et al. [38], who compared two different irrigation protocols and evaluated apically extruded debris associated with various instruments (One Reci, One Curve, Protaper Next in continuous rotation and reciprocating motion, and WaveOne Gold). In their study, WaveOne Gold extruded significantly more debris than other instruments in all subgroups. The enhanced cutting efficiency of rotary NiTi instruments is generally linked to improved cleaning performance; however, when used with a reciprocating motion, it may also increase debris transport toward the apex.
While the findings of this study are in agreement with Abduljalil et al. [37] and Kharouf et al. [38], discrepancies exist when comparing our results to other studies that observed no significant differences in debris extrusion between endodontic instrumentation systems [39]. One possible explanation for this variation is the differences in experimental methodologies, including variations in root canal curvature, instrumentation sequence and types, and debris collection protocols [28, 39].
Moreover, the absence of standardized glide path protocols across studies may contribute to conflicting outcomes. Some studies incorporated manual glide path preparation [4], while others used engine-driven rotary systems [10, 19], which may influence instrument control, stress distribution, and debris evacuation efficiency [8]. These variations highlight the need for standardized methodology when evaluating the impact of instrumentation on apical debris extrusion.
Conversely, continuous rotation by operating similarly to a screw conveyor may encourage the transport of dentin chips and debris toward the coronal region [40], which explains less debris extrusion with TruNatomy files as compared with WaveOne Gold and Reciproc Blue systems. Besides instrument cross-section, another reason for significantly less debris extrusion with TruNatomy prime files could be their 4% taper, which is smaller than the 7% and 8% tapers of WaveOne Gold primary and Reciproc Blue R25, respectively. The bigger taper indicates the presence of a greater contact area with the root canal dentine, hence the production of more debris. This also explains a non-significant difference in the amount of apically extruded debris between all instruments with a prepared glide path.
The superior performance of TruNatomy in reducing apically extruded debris (AED) can be attributed to its unique design features, including a slim NiTi wire, off-centered parallelogram cross-section, and regressive taper [21]. These characteristics enhance flexibility, reduce canal wall engagement, and improve debris removal efficiency, thereby minimizing the apical compaction of debris. Furthermore, the regressive taper design preserves dentin while preventing excessive instrumentation forces near the apex, contributing to reduced debris extrusion and improved shaping efficiency [41].
Our results of less time consumption to prepare the canal in the presence of a glide path are consistent with the literature. Berutti et al. [10] studied the effects of glide path preparation on the preservation of canal curvature following the canal shaping procedure with WaveOne primary file. Their results show lesser packing motions are required when a glide path is present. The presence of a glide path might be the reason for less time consumed in overall canal preparation in the present study. Kirici et al. [42], in their study, performed the glide path preparation in mandibular molars using WaveOne Gold Glider and ProGlider files and found significantly less time required to prepare the canals than the control group. Zheng et al. [13] studied the effects of different glide path preparation techniques on preparation time in curved canals. They concluded that the working time was shorter when a glide path was prepared using engine-driven instruments than the hand files (control group). In a recent literature review that included 14 studies, Lup et al. [2] concluded that rotary glide path preparation reduces canal shaping time compared to glide path preparation with hand files or no glide path groups.
Because of the fewer complexities involved, straight canal instrumentation was more often done and reported in most previous studies [37, 43, 44]. However, technical challenges, including a higher risk of debris extrusion, are more frequent in multirooted teeth with curved canals [28, 45]. Therefore, we used posterior teeth with curved root canals in this experiment to mimic such clinical situations [26, 46]. The glide path preparation, root canal shaping, and cleaning procedures were standardized to ensure reliable comparisons among the groups evaluated in the present study. Clinically, severely curved canals (25°–45°) in posterior teeth pose greater risks of canal transportation, instrument separation, and procedural errors due to limited access and high torsional stress [2, 34, 47]. These challenges can result in inadequate cleaning and shaping and potentially greater apical extrusion of debris, leading to postoperative complications such as flare-ups and pain. The findings of this study suggest that using a glide path in such anatomies improves shaping safety and reduces debris extrusion, which could contribute to more predictable outcomes and enhanced patient comfort in clinical settings.
In clinical practice, incorporating glide path preparation into routine endodontic procedures can enhance treatment efficiency and minimize apically extruded debris (AED). To establish a glide path, clinicians should first assess canal patency using a #10 K-file, ensuring that it reaches the full working length with minimal resistance. A rotary glide path instrument can then be introduced following the manufacturer's recommended settings to safely create a smooth, reproducible path for subsequent shaping instruments.
The use of a glide path is particularly advantageous in curved canals, as it reduces instrument torsional stress, canal transportation, and procedural errors. In rotary systems, the instruments are designed to follow the natural anatomy without excessive dentin removal, maintaining the integrity of the root structure. Additionally, frequent recapitulation with a small hand file (size #10 or #15) and adequate irrigation help prevent instrument binding and ensure proper debris removal.
Given the findings of this study, the incorporation of glide path preparation into clinical protocols can be recommended for complex and curved canals, as it not only improves shaping efficiency but also significantly reduces AED, leading to better postoperative outcomes.
5. STUDY LIMITATION
A limitation of this study is the inclusion of only three single-file instrumentation systems (RCB, WOG, and TN). While these systems were selected based on their distinct metallurgical properties, cross-sectional designs, and motion kinematics, a broader comparison, including additional file systems, could provide further insights into the influence of different instrumentation strategies on apically extruded debris and preparation time. Future studies should explore a wider range of single-file systems and reciprocating versus rotary instrumentation to comprehensively assess their impact on debris extrusion and clinical outcomes.
Since this is an in vitro study, it lacked the presence of apical resistance offered by periapical tissues in natural dentition, which can be considered a limitation of this study. In a clinical setting, periapical tissues, including the periodontal ligament and surrounding bone, may absorb or redirect extruded debris, potentially reducing its impact on postoperative outcomes. However, the arrangements to simulate the periapical tissue pressure, such as floral foam models, have their own limitations and may incorporate errors in the quantification of apically extruded debris.
Additionally, this study does not account for individual patient variability, including differences in immune response, periapical healing potential, and pre-existing periapical conditions, which may influence the extent of inflammation and postoperative symptoms following debris extrusion [48]. While in vitro studies allow for standardized comparisons by eliminating biological variability, they do not replicate the complex host-microbe interactions that may modulate periapical inflammation and healing [49, 50].
Nonetheless, because of strictly followed criteria, the studies conducted under controlled conditions provide directions for further clinical research [1, 51] and produce reliable results among the groups being compared [6, 52, 53]. Further clinical studies investigating AED in vivo with its impact on treatment outcomes, adverse events, and patient-reported outcome measures are needed to validate our findings in real-world clinical settings.
CONCLUSION
Within the limitations of this in vitro study, all tested root-canal instrumentation systems generated apical extrusion of debris in severely curved root canals. A glide path significantly reduced the amount of apically extruded debris and the preparation time. TN files produced less apically extruded debris compared with RCB and WOG. Future clinical research should focus on validating these findings in in vivo settings, where factors such as periapical tissue resistance, patient variability, and healing responses could influence debris extrusion. Additionally, studies exploring the role of glide path preparation in multi-rooted teeth and its impact on postoperative pain and long-term endodontic success rates would further enhance our understanding of its clinical significance.
AUTHORS’ CONTRIBUTIONS
The author confirms sole responsibility for the following: M.Z.A.: Study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| AED | = Apically Extruded Debris |
| RCB | = Reciproc Blue |
| WOG | = WaveOne Gold |
| TN | = TruNatomy |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Committee of Research Ethics, Deanship of Graduate Studies and Scientific Research, Qassim University, Saudi Arabia (registration no. 24-08-04).
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The author acknowledges the support of Dr. Atif Agwan at the Qassim University College of Dentistry for assisting with a second-time evaluation procedure of debris extrusion in this study.

