All published articles of this journal are available on ScienceDirect.

Association between Body Mass Index and Decayed, Missing, and Filled Teeth (DMFT) in 12-year-old School Children
Abstract
Introduction
The body mass index (BMI) helps assess weight and height. Tooth decay is a multifactorial and infectious disease that causes demineralization of the teeth and has a high worldwide prevalence. The study aimed to evaluate the association between the body mass index (BMI) and the decay, missing, and filled teeth index (DMFT) in schoolchildren from the Bellavista parish, Cuenca, Ecuador.
Methods
A cross-sectional study with a quantitative approach was conducted. Data regarding age, sex, weight, and height, were collected from 426 school children in the Bellavista parish, according to WHO standards.
Results
The whole sample mean of BMI was 20.91 (SD 4.2) and the mean DMFT was 2.44(SD 2.3). The analysis conducted using the Fisher-Freeman-Halton test, did not show a significant association between BMI and the DMFT index (p=0.648). When segmented by sex, no relevant differences were found with (p=0.634 for males; p=0.420 for females). Despite the lack of statistical significance, it was observed that schoolchildren who were underweight were the most affected by dental caries with DMFT value of 2.88 (DS 1.73) while obese were the less affected by dental caries with DMFT 2.00(SD 1.98).
1. INTRODUCTION
The body mass index (BMI) is a tool used to determine whether a person's weight is proportional to their height. It is calculated by dividing weight in kilograms by the square of height in meters (kg/m2). In children and adolescents, BMI values are interpreted based on age and sex. BMI measurement provides a critical perspective on health and well-being of a human body, as deviations from expected values can indicate significant impacts on growth, quality of life, and overall health in children.
Dental caries, an infectious oral disease characterized by the demineralization of tooth tissue, has a prevalence exceeding 80%. Globally, it is estimated that 3.5 billion people are affected by oral diseases. Caries is particularly common among children, regardless of socioeconomic background or dietary habits [1-3].
Studies highlight the public health importance of oral hygiene and nutrition due to their significant impact on overall health and well-being. As a result, these topics remain a focal point for health professionals [4]. In a study conducted in Mexico City, it was determined that the majority of people who were examined had dental caries, with a prevalence of 91%. In contrast, 14.5% of the population was affected by overweight or obesity. Interestingly, women were the most affected by these conditions [5]. The prevalence of caries in the same country is shown as one of the highest, with a study conducted between 2010 and 2019 reporting a rate of 94.5%. From 2020 to 2021, this figure decreased to 88.5%. Dental caries is clearly linked to various biological, behavioral, and socioeconomic factors [2]. In a 2022 study in Ecuador, Mena Paola et al. estimated that caries outcomes were directly related to the body mass index (BMI). This finding confirmed the complex relationship between dental caries and obesity, suggesting that dental caries were linked to the habits children develop throughout their lives [6].
Research in Brazil, of a similar nature, has shown that malnutrition is linked to dental caries among low-income children. The study found that 60% of these children had decayed teeth and a higher-than-average PUFA index [7]. While the direct association between BMI and DMFT in children remains inconclusive in some studies, associations have been found that suggest an influence on disease predisposition. These results highlight the potential for policy interventions in oral care and nutritional development to improve child health [2-9].
The DMFT index in a community indicates an average of the individual sum of decayed, missing, and filled teeth, classifying them into different stages according to their severity: very low (0 to 1.1), low (1.2 to 2.6), moderate (2.7 to 4.4), high (4.5 to 6.5), and very high severity (6.6 or >6.6) [10].
The present study aims to answer the following question: is there a correlation between BMI and DMFT in 12-year-old school children in the Bellavista-Cuenca parish? This is a topic that has not been extensively studied in the local context. The study involves forming an association by collecting data from the specified area to evaluate the relationship between BMI and DMFT in 12-year-old school children in the parish of Bellavista-Cuenca.
2. MATERIALS AND METHODS
The present study is observational with a quantitative approach since the dental caries index (DMFT) and its association with the body mass index (BMI) were determined using a data collection technique based on cards. This study was carried out between 2023 and 2024 on schoolchildren in Ecuador, in the city of Cuenca, parish Bellavista. The research complies with the bioethical approval and confidentiality norms. The institutional ethics committee approved the study for research on the Catholic University of Cuenca whose code is CEISH - UCACUE- 013, issued on May 18, 2023, and the legal representatives were duly informed of the study. The study corresponded to all 12-year-old schoolchildren in the different educational units belonging to the Bellavista parish of the canton of Cuenca in Ecuador, and different public schools with morning and afternoon sections, where it was possible to collect complete data on the population studied.
2.1. Ethical Aspects
This study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki (1975), as revised in 2013. Informed consent was obtained from the parents of all participants, and assent was secured from the adolescent participants. Additionally, the study protocol was reviewed and approved by the Ethics Committee of the Catholic University of Cuenca.
2.1.1. Population
The inclusion criteria were: school children 12 years of age, with the consent of the representatives for enrollment in the study, and being students of the Bellavista parish. Exclusion criteria were, school children with orthodontics, patients with systemic diseases, and patients taking medication for over three months. The study was conducted on all patients who met the inclusion criteria; therefore, no sample size calculation was performed. Initially, they were 458 school children, while in the second time for data collection, there were 426 students legally enrolled in the educational centers from 2023 to 2024 since they freely consented before the legal representatives signed informed consent. For this research, age, sex, weight, and height were recorded. They comprise the standardization criteria to avoid selection bias.
2.1.2. Calibration
The examiners were calibrated. They were first instructed on diagnosing dental caries (DMFT) and body mass index (BMI) by professionals. As for the body mass index, measurements were taken according to WHO guidelines [10].
2.1.3. Examination
Before starting the study, the necessary permissions were obtained from the educational centers, they were duly informed, and a dental examination was carried out in different classrooms using natural and artificial lighting provided by the various academic centers. It was carried out with all the biosafety barriers: gown, cap, gloves, and mask, in addition to the previously sterilized instruments that consisted of an oral mirror, an explorer, a periodontal probe, and a field was placed to locate the material and proceed to examine the oral cavity of the schoolchildren as soon as they were seated, using a form designed for this research.
According to the World Health Organization, the sum of decayed, missing, and filled teeth (DMFT), including extracted teeth indicated as dental caries, is calculated as follows: the average of the sum of the total number of decayed, missing and filled teeth in the population examined over the total number of persons examined [10-13].
We calculated the body mass index (BMI = weight in kilos/height in meters2) and thus determined the nutritional status of the students examined. The DMFT is described in Table 1. The researchers were organized into two teams, one working in the morning with ten researchers and the other in the afternoon with ten members. We were responsible for collecting all the information required for the study. We divided each group into pairs to speed up the data collection process. One of the researchers checked the children through clinical examination while the other researcher wrote down the corresponding card, allowing us to carry out the procedure efficiently and accurately.
| Caries | |
|---|---|
| 0 | Sound |
| 1 | Caries |
| 2 | Obturing+Caries |
| 3 | Obturing |
| 4 | Lost due to Carie |
| 5 | Lost for other Reason |
| 6 | Restrained |
| 7 | Crownfixed Prosthetics |
| 8 | Not Erupted |
| 9 | Not Regrooved |
| T | Traumatized |
For the calculation of weight, calibrated scales (CAMRY) with a capacity of 0kg to 120kg were used, and for height, measuring tapes calculating 160 cm and 30 cm possibly by a school-sized ruler fixed to the wall were used. The size was taken with the student upright, head and neck aligned, trunk and ankles close to the wall without shoes. According to the WHO, weight is classified according to standard deviations (SD) as follows: 0 SD= Normal, +1 SD= Overweight risk, +2 SD= Overweight, +3 SD= Obese, -1 SD= Underweight, -2 SD= Very underweight [11].
2.2. Statistical Analysis
We established the percentile categories with the data suggested by the WHO, depending on the BMI of boys and girls. The percentiles established for boys and girls from 5 to 19 years old are as follows: a percentile lower than 3 means meager weight, and between 3 and 15 means low weight. If the percentile falls on the curve between 15 and 50 percentile, it is a healthy weight; if the percentile is between 50 and 85, it is still normal; if it is between 85 and 97, it is overweight; and if it is higher than 97, it is an obesity percentile [12-14].
The data collected during the research were recorded in a file designed for this study. These data were then entered into the Epi info V.7.2.6.0 program. After quality control of the database, it was exported to the SPSS 29 software, using which the statistical analysis was performed. All data were qualitative, so descriptive statistics used frequencies and percentages, while inferential statistics used the Fisher-Freeman-Halton test with 95% reliability to evaluate the association between BMI and DMFT.
3. RESULTS
During the years 2023 and 2024, 458 schoolchildren from various schools in the Bellavista sector were examined, with data collection carried out in two stages: one at the end of the school year and the other at the beginning of the school year and categorized by the sex of the 458 schoolchildren, data of 32 students were lost because some children changed schools, and others decided not to continue, and some schoolchildren over the age of 12 no longer met the criteria for inclusion in the study. Finally, the research focused on 426 children with complete information, classified by gender. The mean BMI for the entire sample was 20.91 (SD = 4.2), and the mean DMFT score was 2.44 (SD = 2.3). Among the BMI categories, very underweight individuals had a DMFT score of 2.88 (SD = 1.73), underweight individuals had a DMFT score of 2.83 (SD = 2.42), and normal-weight individuals had a DMFT score of 2.69 (SD = 2.43). Overweight individuals showed a DMFT score of 2.37 (SD = 2.37), while obese individuals were the least affected, with a DMFT score of 2.00 (SD = 1.98).
Table 2 shows the different nutritional levels classified according to the WHO. This reflects that in the female group, according to nutritional status, the risk of being overweight in women is more prevalent at 28.5% than in men; this group is more prevalent at the overweight level with 28.2%.
The results indicate that there is no difference at the DMFT level between male and female children as shown in the statistical test X2p= 0.3934 (Table 3).
There is no significant association between DMFT levels and nutrition levels, as reflected in the Fisher-Freeman-Halton exact test p= 0.648. The same occurs when evaluating this association in each sex group (Table 4).
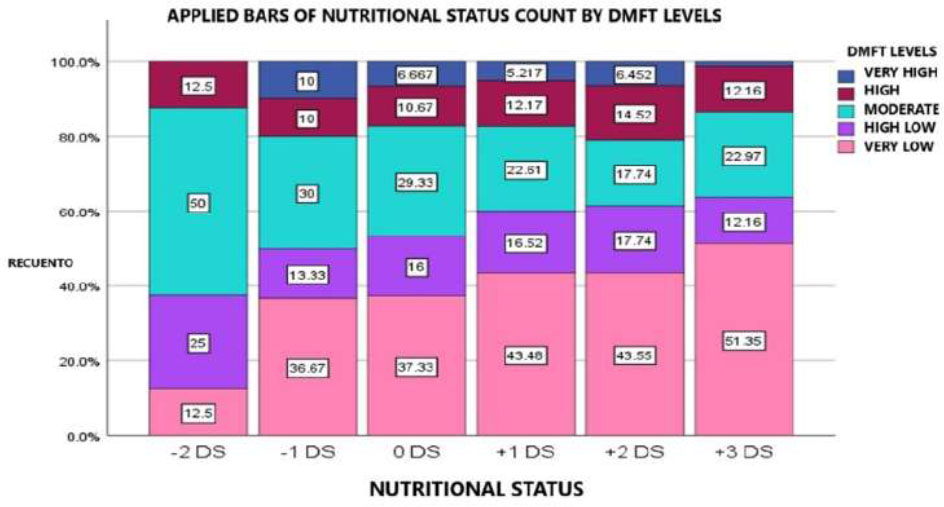
Fig. (1) illustrates a trend where higher BMI levels correspond to higher DMFT levels, while lower DMFT levels are observed at healthier BMI levels. Conversely, the highest levels of caries experience tend to cluster at the extremes of BMI.
4. DISCUSSION
The study was carried out in the urban area of Cuenca, Ecuador. Previously, there was no study conducted of this type in this region. The BMI index given by the WHO was used for both males and females with an average age of 12 years due to the stage of completion of tooth replacement and the DMFT index, in addition to the fact that the WHO follows this age to use indexes, make international comparisons and carry out epidemiological surveillance in oral health. This result is similar to a study carried out in Mexico in 2020, where in children from 8 to 12 years of age who had obesity, the risk of caries was not that high, however, children without obesity had the highest caries risk because they were daily consumers of sugar [15].
| Nutrional Status | |||
|---|---|---|---|
| - | Sex | - | |
| Level | Female | Male | Total |
| - | n% | n% | n% |
| -2SD | 4(1.6) | 4(2) | 8(1.6) |
| -1SD | 13(5.1) | 17(8.4) | 30(6.6) |
| 0SD | 42(16.4) | 33(16.3) | 75(16.4) |
| +1SD | 73(28.5) | 42(20.8) | 115(25.1) |
| +2SD | 67(26.2) | 57(28.2) | 124(27.1) |
| +3SD | 34(13.3) | 40(19.8) | 74(16.2) |
| Total | 233(91) | 193(95.5) | 426(93) |
| DMFT Level | Female | Male | Total |
|---|---|---|---|
| Very low | 104(40.6) | 96(47.5) | 200(43.7) |
| Low | 44(17.2) | 31(15.3) | 75(16.4) |
| Moderate | 57(22.3) | 47(23.3) | 104(22.7) |
| High | 34(13.3) | 20(9.9) | 54(11.8) |
| Very high | 17(6.6) | 8(4.0) | 25(5.5) |
| Total | 256(100.0) | 200(43.7) | 458(100.0) |
| Nutritional Status | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | DMFT | -2DS | % | -1DS | % | 0DS | % | +1DS | % | +2DS | % | +3DS | % | Total | % | SIG* | ||
| Female | Very Low | 0 | 0.0% | 6 | 46,2% | 12 | 28,6% | 32 | 43,8% | 28 | 41,1% | 16 | 47,1% | 94 | 40,3% | 0,420 | ||
| Low | 1 | 25,0% | 0 | 0,0% | 5 | 11,9% | 15 | 20,5% | 11 | 16,4% | 6 | 17,6% | 38 | 16,3% | ||||
| Moderate | 2 | 50,0% | 4 | 30,8% | 14 | 33,3% | 13 | 17,8% | 12 | 17,9% | 8 | 23,5% | 53 | 22,7% | ||||
| High | 1 | 25,0% | 2 | 15,4% | 6 | 14,3% | 9 | 12,3% | 11 | 16,4% | 4 | 11,8% | 33 | 14,2% | ||||
| Very High | 0 | 0.0% | 1 | 7,7% | 5 | 11,9% | 4 | 5,5% | 5 | 7,5% | 0 | 0,0% | 15 | 6,4% | ||||
| - | 4 | 100% | 13 | 100% | 42 | 100% | 73 | 100% | 67 | 100% | 34 | 100% | 233 | 100% | ||||
| Male | Very Low | 1 | 25,0% | 5 | 29,4% | 16 | 48,5% | 18 | 42,9% | 26 | 45,6% | 22 | 55,0% | 88 | 45,6% | 0,634 | ||
| Low | 1 | 25,0% | 4 | 23,5% | 7 | 21,2% | 4 | 9,5% | 11 | 19,3% | 3 | 7,5% | 30 | 15,5% | ||||
| Moderate | 2 | 50,0% | 5 | 29,4% | 8 | 24,2% | 13 | 31,0% | 10 | 17,5% | 9 | 22,5% | 47 | 24,4% | ||||
| High | 0 | 0,0% | 1 | 5,9% | 2 | 6,1% | 5 | 11,9% | 7 | 12,3% | 5 | 12,5% | 20 | 10,4% | ||||
| Very High | 0 | 0,0% | 2 | 11,8% | 0 | 0,0% | 2 | 4,8% | 3 | 5,3% | 1 | 2,5% | 8 | 4,1% | ||||
| - | 4 | 100% | 17 | 100% | 33 | 100% | 42 | 100% | 57 | 100% | 40 | 100% | 193 | 100% | ||||
| Total | Very Low | 1 | 12,5% | 11 | 36,7% | 28 | 37,3% | 50 | 43,5% | 54 | 43,5% | 38 | 51,4% | 182 | 42,7% | 0,648 | ||
| Low | 2 | 25,0% | 4 | 13,3% | 12 | 16,0% | 19 | 16,5% | 22 | 17,7% | 9 | 12,2% | 68 | 16,0% | ||||
| Moderate | 4 | 50,0% | 9 | 30,0% | 22 | 29,3% | 26 | 22,6% | 22 | 17,7% | 17 | 23,0% | 100 | 23,5% | ||||
| High | 1 | 12,5% | 3 | 10,0% | 8 | 10,7% | 14 | 12,2% | 18 | 14,5% | 9 | 12,2% | 53 | 12,4% | ||||
| Very High | 0 | 0,0% | 3 | 10,0% | 5 | 6,7% | 6 | 5,2% | 8 | 6,5% | 1 | 1,4% | 23 | 5,4% | ||||
| Total | 8 | 100% | 30 | 100% | 75 | 100% | 115 | 100% | 124 | 100% | 74 | 100% | 426 | 100% | ||||
Association of nutritional status and DMFT levels.
On the other hand, in Saudi Arabia in the year 2020, they introduced in their research the association between obesity and dental caries in children between 12 and 15 years old, since they are known to be global health problems. In their study, they observed that children with high caries belonged to the obesity group; it was more prevalent in males than in females. In the present study, the prevalence of caries according to DMFT also shows an inclination for the male sex. Therefore, it is understood that preventive policies should be taken into account to control these diseases [16].
In many countries, caries is a neglected problem. Therefore, there are always high prevalence reported in some studies. The DMFT index of 12-year-old children recorded in the year 2021 in the study by Olivan Gonzalo et al. showed that in Ecuadorian children residing in Spain, untreated caries was more prevalent with 25.4% in comparison with children of other nationalities. Also, there is no direct association of the nutritional status with the BMI [17].
On the other hand, according to a study in Mexico in 2014, an association between caries and body mass index dental caries was higher in school children who were overweight and obese [18]. Likewise, in the same country, another study was conducted in the year 2023 where a population of children from an area in the east of the country was studied, and the data highlighted in the same way an association between DMFT and BMI in the two groups having both male and female children affecting the level of obesity, however the DMFT index was presented only in the male group, that is where the importance of adequate information on nutrition, promotion and prevention programs in schools guiding to new eating habits and likewise avoiding caries is reflected [19].
In El Salvador, a study conducted in 2022 by Salgero Jennifer et al., who investigated the association of body mass index with the caries index, lost and filled, and reported that there was a direct association between them. This research was conducted in mixed dentition, the results indicated that in the permanent dentition, the prevalence of caries was 70, 5% and the caries index in primary dentition was 94.9%. This finding related to the BMI was prevalent in children in the overweight and obese group. This number indicates that more prevention and information on general and oral health should be instilled in the population of this country [20].
Mohajeri Amir et al. examined in their study the correlation between obesity and dental caries using regression models considering demographic variables, socioeconomic status, diet, and controlling factors. However, the data indicated that caries and untreated caries were not directly related to BMI-weight, therefore, there are other external causes involved, such as poor hygiene, family habits, etc. It is indicated that dentists should be aware of these factors since they greatly influence the development and prevention of caries [21]. Shi Rou et al. conducted a study in China, investigating dietary habits, hygiene habits, and parental status. The found that BMI and DMFT were negatively related; the underweight group had the highest prevalence with 65.6% than the obese group with 41.1% prevalence of caries [22].
In the study carried out by the government of Cameroon in 2023, in a cross-sectional investigation, six hundred and fifty school children from different primary schools were evaluated. It was revealed that the prevalence of overweight was very high, and the oral pathology that was most related was dental caries, with 60.3%. This meant that overweight children were 1.5 times more likely to develop caries. In our research, we found contradictory results. The analyzed results did not correlate with our findings as children who were overweight did not have any caries [23]. It is well known that nutrition significantly impacts oral health, which is why there are multiple studies analyzing the possible factors, perhaps to plan new strategies. A study conducted in Turkey was similar to our study; however, its study population was 5 to 14 years of age; after all the results were analyzed, it was shown that obesity was a pretty prominent risk factor, and the risk of caries increased in this group of school children examined [24]. Therefore, these two variables had a direct association, which differed from what was found in the present study [25], and the DMFT index is under constant debate. Some studies suggest that the higher the BMI, the greater the experience of dental caries. However, in the study conducted in Iraq, caries-free individuals and patients with caries were from the normal weight group. This differs from the present study, which found that the caries-free children (with very low DMFT level) belonged to the overweight (+2DS) and obese (+3DS) groups [26-28].
Ali Borzabadi et al., identified a possible relationship between malocclusion and caries, with no significant association overall, but in certain subgroups [29]. In another study by the same author, they noted that caries increases with age and is more prevalent in men. Our study, although without significant associations, highlights the importance of a multifactorial approach considering different age groups [30].
On the other hand, another study in Saudi Arabia has reported contradictory results, showing that obese children may have higher DMFT values. These findings suggest that the relationship between obesity and caries is multifactorial and may be influenced by other factors such as age, gender, oral hygiene habits, and diet. It is essential to continue exploring this association in different population settings and with more precise methodologies to better understand the interaction between oral health and nutritional status [31, 32].
The study by F. Eslamipour suggests that obesity may be related to poorer oral hygiene, increasing the risk of caries [30]. Although our study did not find a significant association between BMI and caries, it showed a trend of higher caries with lower BMIs. Both studies highlight that this relationship is multifactorial and should be evaluated considering hygiene, diet, and socioeconomic status, reinforcing the need for a preventive and comprehensive approach [33].
CONCLUSION
According to the analysis of 426 school children from the parish of Bellavista-Cuenca, there was no statistically significant association found between the body mass index (BMI) and DMFT index. This relationship was not reflected in the Fisher-Freeman-Halton test and was maintained even when analysing the data by sex. However, the mean values of the DMFT index tend to be centred at the extremes of BMI, showing a greater experience of caries in both underweight and highly underweight school children. At the same time, the lowest levels of DMFT were recorded in children with obesity. These trends do not have statistical significance but may indicate a non-linear relationship or multifactorial influence useful for future studies.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper: study conception and design: E.V.C.: Data collection; A.J.A.D.: Analysis and interpretation of results; E.V.C., A.J.A.D.: Draft manuscript; E.V.C., A.J.A.D. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| BMI | = Body Mass Index |
| DMFT | = Tooth decay, caries lost and filled teeth |
| SD | = Standard deviation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
On May 18, 2023, the authors received approval from the ethics committee of research in human beings of the Universidad Católica de Cuenca, faculty of Dentistry, (Code: CEISH—UCACUE—013).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the parents of all participants, and assent was secured from the adolescent participants.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [E.V-C] upon reasonable request.
FUNDING
The study was funded by the Catholic University of Cuenca, Cuenca, Ecuador, (UCACUE) for the project approved under code: PICIV-18-05.
ACKNOWLEDGEMENTS
Declared none.

