All published articles of this journal are available on ScienceDirect.

Knowledge, Attitudes, and Practice about Teeth Bleaching Among Subpopulation in Saudi Arabia: A Cross-sectional Study
Authors Info & Affiliations
Abstract
Background
One of the most popular cosmetic dental procedures is teeth whitening. The public's comprehension of its safety and appropriate use, however, is still lacking. The purpose of this study is to assess knowledge, attitudes, and practices about teeth whitening among the population in Saudi Arabia.
Methods
Using a validated questionnaire, 500 persons in Saudi Arabia participated in a cross-sectional survey. The survey evaluated participant knowledge, opinions, and teeth-whitening behaviors in addition to demographic information. SPSS was used to analyze the data, and a significance level of p < 0.05 was considered significant.
Results
Most participants (88%, n=440) understood that getting a dental consultation was necessary before getting teeth whitening. On the other hand, only 29.2% (n=146) thought the bleaching was safe, while 53.6% (n=268) were unsure. Better attitudes and understanding about teeth whitening were substantially correlated with higher educational attainment (p < 0.001). While most people knew that smoking causes tooth discoloration (94.8%, n=474), fewer people knew that other factors, such as too much fluoride, can also cause it (59%, n=295).
Conclusion
Most people in Saudi Arabia understand how important it is to get professional advice before bleaching their teeth. However, there are still false beliefs about its safety, especially among the less educated. It is advised to implement focused educational programs to raise public awareness and encourage safer teeth-whitening procedures.
1. INTRODUCTION
Many people, specifically those in the entertainment sector and young ladies, are quite demanding for their teeth appearance and good look, which is why many of them choose to have dental aesthetic procedures. Additionally, this has a significant effect on society. As a result, one of the most alluring aspects of helping people gain patient satisfaction is cosmetic dentistry. Bleaching is one of the conservative methods to treat stained teeth in order to improve their appearance. Intrinsic and extrinsic discolorations are two categories of tooth discoloration, which can occur during or after tooth development. Excessive fluoride consumption, tetracycline use, or metal exposure at the time of tooth development are the main factors that lead to internal staining. These stains have resistance to home bleaching methods, while extrinsic stains frequently respond well to home bleaching agents, which can be caused by metal exposure, tobacco usage, and certain fluids like tea or coffee [1, 2]. As early as 1868, vital teeth were bleached using oxalic acid or pyrozone, and later, hydrogen peroxide became a common agent. By 1911, applying concentrated hydrogen peroxide along with a heating device or light source was considered an acceptable practice in dental clinics [3-5]. With the recent progress in adhesive and advanced restorative techniques, there are more chances than ever to give patients and dentists the best conservative approaches to improve good appearance of teeth through cost-effective and less invasive procedures [6]. The development of teeth bleaching techniques represents a significant advancement in restorative and cosmetic dentistry. There are two types of bleaching: one is internal bleaching for nonvital teeth, and the other method is for vital teeth with external bleaching [7]. Also known as teeth whitening, it involves either bringing the natural color of teeth back or going lighter than that [8, 9]. Additionally, it involves debriding the teeth or removing the debris. Nevertheless, the bleaching procedure could expose enamel cracks. Saliva fastens the remineralization process for some of these cracks, while biological waste fills other crevices once more [10]. In the early 1900s, hydrogen peroxide (H2O2) was employed as a bleaching agent. In 1895, the American Journal of Dental Science reported both this method and the hydrochloric acid microabrasion technique. The media and its commercials have contributed to a rise in people's anxieties about their appearance in recent years. Furthermore, the ease of use and quick outcomes of teeth whitening contribute to better patient perceptions and attitudes regarding cosmetic dentistry [8, 11]. As a result, tooth whitening has gained prominence as a popular aesthetic dentistry procedure for improving the appearance of people's teeth. Unfortunately, despite the benefits of teeth whitening, several negative effects do exist, including weakening the dentin and tooth sensitivity [12, 13]. Moreover, gingival and mucosal irritation are also considered side effects of the bleaching procedure [14]. Overbleaching causes damage to tooth enamel and decreases dentin strength [15]. Although teeth whitening is one of the most common aesthetic procedures, public awareness regarding its type, mechanism, duration of effects, and potential side effects is limited. Studies show a significant increase in demand for teeth whitening, driven by the desire for an attractive smile [16, 17]. Teeth bleaching has become a commonly performed procedure in contemporary dental practice, addressing one of the most prevalent concerns related to tooth color and aesthetics. This study aims to assess the knowledge, attitudes, and practices among the Saudi subpopulation regarding teeth bleaching.
2. MATERIALS AND METHODS
2.1. Study Design, Setting, and Participant
A descriptive study using a survey design was conducted to measure the public's knowledge, attitudes, and practices about teeth whitening in the Saudi Arabian subpopulation. The study population was made up of physically and mentally fit individuals living in Saudi Arabia who were at least eighteen years old. People under the age of eighteen, people who did not live in Saudi Arabia, and people with unusual physical or mental conditions that would make it difficult for them to understand or complete the survey were among the exclusion criteria. The present study recruited N=500 participants during the data collection period of 3 months. Non-probability, convenient sampling technique was used to gather the data. With express permission, the study used a validated questionnaire from the study done by Eyyd et al. [18]. There were 22 questions on the survey, which were divided into four categories: demographic, knowledge, practice, and attitude questions. The demographic section included six questions about age, nationality, residence region, gender, education level, and monthly income level. The knowledge section included five questions to gauge knowledge about bleaching (such as whether bleaching will remove a thin layer from tooth structure, whether bleaching is safe, whether excessive bleaching product use is harmful, and whether bleaching agents should come into contact with the gingiva). The attitudes section included five questions about bleaching safety, information from advertisements about bleaching, consultation before bleaching, color stability after bleaching, and relapse effect), and six questions about bleaching practices (have you ever sought advice regarding bleaching, how bleaching affects teeth and restorations, whether smoking and drinking should be avoided following bleaching, how effective bleaching remedies are, what kind of discoloration can be resolved through bleaching, and how bleaching can improve the odor of the oral cavity). Google Forms, a widely available and user-friendly tool that allowed for quick and effective data collecting, was used to distribute the questionnaire electronically. Social media platforms, such as (X and WhatsApp) were used to disseminate Google Forms. Data was collected from June, 2024 to August, 2024
2.2. Ethical Considerations
Before starting data collection, a thorough application for ethical permission was made to the University of Hail's Research Ethics Committee, which follows the regulations of the Helsinki Declaration of 1975, as revised in 2013, and approval (H-2024-348) was received. The ethical application contained detailed information regarding the goals, design, and any dangers to participants of the study. Furthermore, each subject gave their informed consent. The goal of the study, its methodology, and any possible risks or rewards for participation were all discussed in detail in the consent form. Participants received assurances about the privacy of their answers, and their personal information was anonymised.
2.3. Study Variables
In this study, the primary outcomes were the knowledge, attitudes, and practices (KAP) regarding teeth bleaching. The key independent variables included gender, region, level of education, and income, which were analysed as potential predictors of KAP. These variables were selected to explore their influence on public perceptions and behaviours related to teeth bleaching.
2.4. Statistical Analysis
The Statistical Package for Social Sciences (SPSS) program for Windows version 21 was used to methodically arrange, evaluate, and analyse the data that had been gathered. p-values less than 0.05 were deemed statistically significant using the Pearson’s Chi-square test.
| Variable | N (%) |
|---|---|
| Age-group | |
| Older than 18 years | 500 (100%) |
| Nationality | |
| Saudi | 493 (98.6%) |
| Non-Saudi | 7 (1.4%) |
| Region | |
| Riyadh | 31 (6.2%) |
| Makkah | 10 (2.0%) |
| Qassim | 13 (2.6%) |
| Hail | 390 (78.0%) |
| Eastern | 29 (5.8%) |
| Other | 27 (5.4%) |
| Gender | |
| Male | 111 (22.2%) |
| Female | 389 (77.8%) |
| Level of Education | |
| High school | 37 (7.4%) |
| Diploma | 89 (17.8%) |
| University | 374 (74.8%) |
| Income | |
| Less than 2000 | 123 (24.6%) |
| 2000-5000 | 84 (16.8%) |
| 5000-10000 | 123 (24.6%) |
| More than 10000 | 170 (34.0%) |
3. RESULTS
This study included a total of 500 adult participants, all aged 18 years or older. The majority of the sample, 98.6% (n=493), identified as Saudi citizens. The proportion of non-Saudi participants in the sample was quite low, at 1.4% (n = 7). Regarding the participants' regional distribution, the majority of them, or 78.0% (n=390) of the entire sample, were from Hail, with 6.2% (n=31) of participants coming from Riyadh, which was the second most represented region, followed by the Eastern Region with 5.8% (n=29). Makkah had the lowest representation, with only 2.0% (n=10) of participants, followed by Qassim with 2.6% (n=13) and participation from other locations with 5.4% (n=27). The gender distribution showed 111 participants (22.2%) were male out of the total 500 participants, and 389 participants (77.8%) were females. The majority of participants (74.8%, n=374) had a university education, only 17.8% (n=89) of the sample had a diploma, and 7.4% (n=37) had finished high school. There was a noticeable variation in the participants' income distribution. Moreover, 34.0% (n=170) of the sample's income was over 10,000 SAR per month, making up the largest income category. Less than 2,000 SAR and between 5,000 and 10,000 SAR were reported by an equal percentage of participants (24.6%, n=123). Furthermore, in 16.8% (n=84) of individuals, the monthly income ranged between SAR 2,000 and $5,000 (Table 1).
The data presented in Fig. (1) highlights key factors associated with public knowledge regarding tooth discoloration. Smoking and tea/coffee intake were the most widely recognized causes, with 94.8% and 95.4% of participants, respectively, agreeing that these contribute to tooth discoloration. High awareness was also observed regarding the role of excessive fluoride in drinking water (59%) and inherited factors (59.2%). Additionally, 71.8% of respondents identified bacteria as a contributing factor. While these findings demonstrated a high level of awareness for certain causes, other factors, such as the impact of antimicrobial mouthwashes (40.2%) and endodontic materials (30.8%), showed lower levels of recognition.
In Fig. (2), it was observed that 404 participants (80.8%) knew about bleaching, and 96 participants (19.2%) were not aware of bleaching.
A total of 395 (79%) participants agreed with the statement that bleaching removes a thin layer from the tooth structure, whereas 105 (21%) disagreed. Just 29 (5.8%) respondents disagreed with the vast majority, 471 (94.2%), who acknowledged that using bleaching products excessively could be hazardous. Furthermore, 388 (77.6%) individuals agreed, while 112 (22.4%) disagreed, that bleaching agents should not come into contact with the gingiva. Regarding opinions on safety, 268 (53.6%) respondents were unsure whether bleaching is safe, whereas 146 (29.2%) thought it was, and 86 (17.2%) disagreed (Fig. 3).
A total of 440 (88%) participants said they were skeptical about getting information about tooth whitening from advertisements, and an equal number of 440 (88%) agreed that seeing a dentist before beginning any at-home bleaching was crucial. The idea that the color obtained after bleaching will endure forever was generally disapproved by 454 (90.8%), with only 46 (9.2%) of respondents holding this belief. Regarding relapse, 197 (39.4%) disagreed with 303 (60.6%), who said that in the event of a relapse, the teeth would be a darker shade than they were initially. In terms of getting expert guidance, 277 (55.4%) respondents had visited a dentist for information about bleaching compared to 223 (44.6%) who had not. Of the participants, 224 (44.8%) thought that bleaching might make existing restorations and teeth whiter, while 276 (55.2%) did not think so. Furthermore, 434 (86.8%) of respondents said that smoking and consuming tea or coffee should be avoided after teeth whitening, and 416 (83.2%) said that some home treatments might be successful in lightening teeth. However, only 145 (29%) respondents thought that bleaching could treat any kind of tooth discoloration, and 178 (35.6%) said that bleaching could make the oral cavity smell better (Table 2).
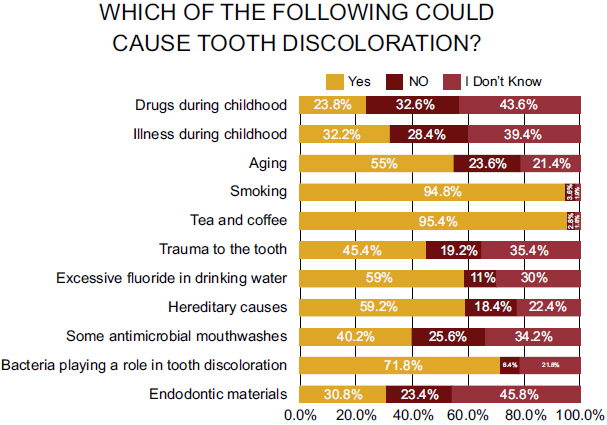
Knowledge of causes of tooth discoloration among participants.
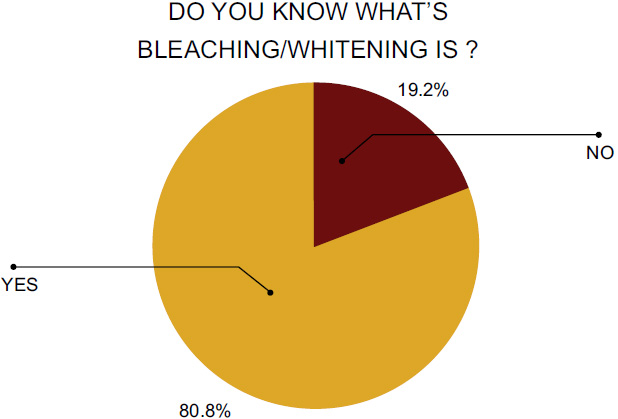
Knowledge of dental bleaching among participants.
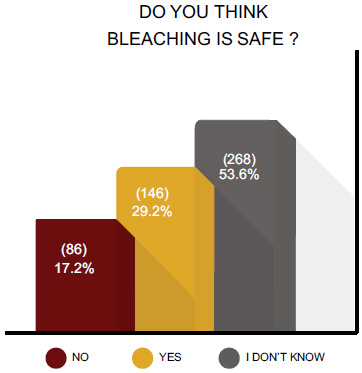
Perception of the safety of dental bleaching among participants.
| S. No. | Knowledge, Attitude, and Practice Questions | Yes | No |
|---|---|---|---|
| N (%) | N (%) | ||
| 1 | Bleaching will remove a thin layer from the tooth structure. | 395 (79.0%) | 105 (21.0%) |
| 2 | Excessive use of bleaching products could be harmful. | 471 (94.2%) | 29 (5.8%) |
| 3 | Bleaching agents should not come in contact with the gingiva. | 388 (77.6%) | 112 (22.4%) |
| 4 | I should not rely on the information mentioned in advertisements on tooth bleaching. | 440 (88.0%) | 60 (12.0%) |
| 5 | I should consult a dentist before starting any type of home bleaching. | 440 (88.0%) | 60 (12.0%) |
| 6 | The color achieved after bleaching will last forever. | 46 (9.2%) | 454 (90.8%) |
| 7 | In case of relapse, the color of the teeth will be darker than the original. | 303 (60.6%) | 197 (39.4%) |
| 8 | Have you ever consulted a dentist to gain information about bleaching? | 277 (55.4%) | 223 (44.6%) |
| 9 | Bleaching can whiten both the teeth and old restoration. | 224 (44.8%) | 276 (55.2%) |
| 10 | Smoking and drinking tea and coffee should be avoided after bleaching. | 434 (86.8%) | 66 (13.2%) |
| 11 | Some remedies can be effective for tooth bleaching. | 416 (83.2%) | 84 (16.8%) |
| 12 | All types of tooth discoloration could be treated by tooth bleaching. | 145 (29.0%) | 355 (71.0%) |
| 13 | Dental bleaching can improve the smell of the oral cavity. | 178 (35.6%) | 322 (64.4%) |
The degree of education was found to be significantly correlated with the presence of smoking as a cause of tooth discoloration; 357 participants with a university education (71.4%) agreed, compared to 82 participants (16.4%) with a diploma and only 33 participants (6.6%) with a high school education (p < 0.001). With 244 participants (48.8%) from the Hail region and 10 participants (2.0%) from Riyadh, respectively, participants from the Hail region had the highest awareness of the negative effects of excessive fluoride in drinking water (p = 0.007). Gender was found to be substantially linked (p = 0.047), with 296 female participants (59.2%) agreeing, 92 (18.4%) disagreeing, and 112 (22.4%) unclear about hereditary reasons for discolouration. Endodontic materials were found to be a significant cause of tooth discoloration in both age groups (p = 0.008) and regions (p = 0.045). Of the participants, those from Hail had the highest awareness (22%), with 30.8% having more knowledge than those over the age of 18. In relation to bleaching, there was a strong correlation found between participants' understanding of the detrimental effects of excessive use of bleaching products and their education level (p < 0.001) and gender (p = 0.010). Those with a university education were the most aware; 362 (72.4%) agreed, whereas only 30 (5.9%) of those with a high school education disagreed (Table 3).
| S. No. | Knowledge Questions | Region | Gender | Level of Education | Income |
|---|---|---|---|---|---|
| 1 | Do you know what bleaching/whitening is? | 0.808 | 0.023* | 0.045* | 0.042* |
| 2 | Bleaching will remove a thin layer from the tooth structure. | 0.29 | 0.215 | 0.887 | 0.767 |
| 3 | Excessive use of bleaching products could be harmful. | 0.274 | 0.010* | 0.001* | 0.739 |
| 4 | Bleaching agents should not come in contact with the gingiva. | 0.114 | 0.004* | 0.812 | 0.747 |
| S. No. | Attitude Questions | Region | Gender | Level of Education | Income |
|---|---|---|---|---|---|
| 1 | Do you think bleaching is safe? | 0.314 | 0.001* | 0.349 | 0.018* |
| 2 | I should not rely on the information mentioned in advertisements on tooth bleaching. | 0.661 | 0.223 | 0.823 | 0.12 |
| 3 | I should consult a dentist before starting any type of home bleaching. | 0.09 | 0.375 | 0.094 | 0.071 |
| 4 | The color achieved after bleaching will last forever. | 0.734 | 0.937 | 0.026* | 0.477 |
| 5 | In case of relapse, the color of the teeth will be darker than the original. | 0.321 | 0.472 | 0.096 | 0.63 |
Significant correlations were found between the attitudes of participants about teeth bleaching and a number of demographic variables, such as gender, income, and educational attainment. The study found a significant relationship between perceptions of the safety of teeth whitening and income (p = 0.018) and gender (p < 0.001). This suggests that persons with different income levels and genders hold differing opinions about the safety of tooth bleaching. In particular, 86 people (17.2%) did not think bleaching was safe, 268 participants (53.6%) were unclear, and 146 participants (29.2%) thought it was. Of the participants, 101 (20.2%) with a university education thought bleaching was safe, compared to 11 (2.2%) with only a high school education. With 109 out of 390 individuals (27.9%) from Hail believing bleaching to be safe, participants from that region had the highest level of skepticism regarding its safety (p = 0.090). When it comes to the veracity of tooth-whitening commercials, participants' wealth (p = 0.071) and geography (p = 0.090) demonstrated significance, indicating that their levels of skepticism may vary slightly. There were no significant connections found between opinions toward contacting a dentist prior to starting at-home bleaching, regardless of income, education level, gender, or region. Nonetheless, there was a trend toward a higher chance of seeking expert help among individuals from Hail and those in higher income groups (p > 0.05). There was a strong correlation (p = 0.026) between participants' expectations regarding the durability of teeth bleaching treatments and their education level. The majority of the 46 individuals (9.2%) who thought bleaching results would persist indefinitely were college graduates (Table 4).
The proportion of subjects intending to consult with a dentist before bleaching did not significantly differ in relation to any demographic variable that was associated with visiting a dentist for information about bleaching (p > 0.05). Similarly, 277 participants (55.4%) consulted a dentist, and 223 participants (44.6%) did not. However, there was a significant correlation between gender and belief that tooth-bleaching bleaches teeth along with all old restorations; 224 participants (44.8%) agreed, and 276 (55.2%) disagreed (p = 0.045). There was a significant association between the belief that some remedies could effectively whiten teeth and education (p = 0.009), with 323 participants in agreement who had a university level of education (83.2%) compared to only 23 high-school educated participants (67.6%). No significant correlations were identified between smoking and consuming tea or coffee as well as with all other variables. Further, there was no significant difference with any of the variables (p > 0.05). Only weak associations were found among beliefs that bleaching was effective in any type of tooth discoloration, and there was no significant correlation (Table 5).
| S. No. | Practice Questions | Region | Gender | Level of Education | Income |
|---|---|---|---|---|---|
| 1 | Have you ever consulted a dentist to gain information about bleaching? | 0.124 | 0.105 | 0.455 | 0.423 |
| 2 | Bleaching can whiten both the teeth and old restoration. | 0.54 | 0.045* | 0.467 | 0.08 |
| 3 | Smoking and drinking tea and coffee should be avoided after bleaching. | 0.311 | 0.167 | 0.97 | 0.798 |
| 4 | Some remedies can be effective for tooth bleaching. | 0.124 | 0.21 | 0.009* | 0.968 |
| 5 | All types of tooth discoloration could be treated by tooth bleaching | 0.201 | 0.366 | 0.191 | 0.389 |
| 6 | Dental bleaching can improve the smell of the oral cavity. | 0.292 | 0.911 | 0.306 | 0.79 |
4. DISCUSSION
The current research study sheds light on the level of knowledge, attitudes, and practices towards dental bleaching among the Saudi subpopulation. The sample group was comprised of 500 people over the age of 18, meaning that these findings are likely to be more reliable as a result of this mature and potentially more aware population. The age restriction permits the study to be more relevant by excluding younger participants who may not have a suitable level of knowledge or exposure to dental procedures, such as bleaching.
The current study showed that 88% agreed that dental consultation was needed prior to bleaching, which was one of the most important findings. Our high percentage of awareness is in agreement with a study done by Alnomay et al., which found a high knowledge indicator (88.4%) about the necessity for consultation before starting the procedure [19]. The consistency of this finding with previous studies indicates that the study population has high trust in professional consultation before dental bleaching, and it also reflects the increasing knowledge that people have of dental health and the dangers of self-treatable procedures. In addition, this study demonstrated that an educational level is an important factor of knowledge on tooth bleaching. In the present study, 302 participants with a university education had more knowledge than their other counterparts (p = 0.045). Consistent with the findings reported by Alnomay et al. [19], it was found that university-educated people are more aware. The association may reflect greater health literacy in those with higher educational attainment who have a better understanding of dental procedures, highlighting education as a key component in raising awareness of the importance of oral health.
Curiously, as for the safety of dental bleaching, a significant difference was found in a study by Alamassi et al. [20], where 65.4% of participants supported the safety of the bleaching method, and only 18.3% were not sure of that. By comparison, the current study identified a much higher level of uncertainty, with 268 participants (53.6%) unsure that bleaching was safe and only 146 participants (29.2%) endorsed its safety. In this regard, the observed marked difference in perception might vary by region due to public awareness of the safety of dental bleaching, or if not, then differences in access to trusted information on dental health may affect opinion. The increased uncertainty seen in this study highlights the importance of the public being further informed about the safety and risks associated with dental bleaching, considering its popularity as a cosmetic procedure. One other main difference between the two studies was the knowledge that participants had about water fluoridation and its associated risk of tooth discolorations. In a study by Alamassi et al. [20], only 16.3% knew that excessive fluoride in drinking water causes discoloration. In contrast, 59% (295 people) in this study correctly identified excessive fluoride in the drinking water as a cause of tooth colour change. This vast discrepancy in awareness could be due to factors, such as local water fluoride concentrations and differences in dental health education initiatives. The increased awareness reported by this study indicates that the study population might be more informed about the effect of fluoride due to health promotion programs or their improved accessibility to dental care.
The researchers also directly measured participants' understanding of the causes of tooth discoloration and compared this measure to earlier studies. The study by Eyyd et al. reported that 35.2% of participants attributed drug use during childhood, while 33.3% thought it was due to illness, and 76.6% attributed smoking as a cause of tooth discoloration [18]. In the current study, 94.8% of the participants indicated that tooth discoloration was related to smoking, significantly more than the 119 (23.8%) that linked discoloration with drug use or the 161 (32.2%) linking it with illness in the current study. Greater recognition of the effect of smoking on tooth color may reflect successful public health campaigns about the risks associated with smoking, including its cosmetic aspects, or more widespread delivery of health information regarding this aspect among smokers in this cohort. Furthermore, as noted in the present study, participants were more knowledgeable about other aetiologies of tooth discoloration as compared to those included in a study by Eyyd et al. [18]. Secondly, most of the participants were not aware that mouthwash, trauma, fluoride, and inherited factors are causes of tooth discoloration. Instead, the current study found much higher levels of awareness in almost every category: trauma (45.4%), fluoride (59%), inheritance (59.3%), and mouthwash use for tooth discoloration (40.2%). The higher percentage reflects that the participants in this research were essentially more aware of the numerous causes of tooth discoloration, presumably as a result of more availability of dental education and health services.
Of the 250 participants (76.7%) in a study by Joshi et al., 76 participants (23.3%) knew that endodontic materials could contribute to tooth discolouration. Nonetheless, the present study revealed that a slightly greater proportion of participants (N=154, 30.8%) knew about the effect of endodontic materials, whereas 117 (23.4%) disagreed and 229 (45.8%) were not sure. This suggests that there is a significant awareness gap between the two groups, which may be due to differences in access to public health or dentistry education [21].
5. LIMITATION
The use of convenience sampling limits the generalizability of the findings, and self-reported data may have introduced response bias. The cross-sectional design captures data from only a single point in time, preventing conclusions about causal relationships. Additionally, while the questionnaire was validated, it may not have fully captured the complexity of participants' understanding of different bleaching procedures and their long-term effects. These factors should be considered when interpreting the study’s results.
CONCLUSION
The majority of people in Saudi Arabia are aware that getting professional advice before teeth whitening is necessary. Yet there are still misconceptions about its safety, according to this study. Better knowledge and attitudes were found to be correlated with higher education levels, suggesting that focused education programs are needed to overcome these inequalities. Increasing public awareness of the dangers and safe procedures related to tooth whitening might encourage safer and better-informed decisions.
AUTHORS’ CONTRIBUTION
M.A. and A.A.S.: Study conception and design; Y.E.A., F.F.A., and S.A.A.: Data collection; M.A., A.A.S., and Y.E.A.: Analysis and interpretation of results; M.A., A.A.S., Y.E.A., F.F.A., and S.A.A.: Draft manuscript.
All authors reviewed the results and approved the final version of the manuscript.
ABBREVIATION
| KAP | = Knowledge, Attitudes, Practices |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical permission was granted by the University of Hail's Research Ethics Committee, Kingdom of Saudi Arabia (H-2024-348).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting information are provided within the article.
ACKNOWLEDGEMENTS
Declared none.

