All published articles of this journal are available on ScienceDirect.

Threaded Bone Expanders in Implantology: A literature review
Abstract
In the field of implantology, we require numerous surgical instruments and specialized kits for cases where the available bone lacks ideal quantity and quality. Threaded bone expanders are among the specialized tools with broad applications that can address issues related to bone deficiency or density.
This research aimed to provide a thorough review of threaded bone expanders, encompassing their historical use, types, mechanism of action, and clinical applications in the context of dental implants.
An internet search was conducted on the internet using search, engines such as Google, Research Gate, PubMed, and PubMed Central. The search utilized keywords including Bone expander, Bone Spreader, Bone condenser, Screw-type expander, and Threaded bone expander.
Out of the initial 96 articles identified in the search, 29 studies met the inclusion criteria established for this review. Two reviewers independently conducted the evaluation of eligibility and data extraction.
Threaded bone expanders are essential tools in the field of implant dentistry, particularly in cases where the available bone lacks ideal density and quantity. These versatile tools are successfully used in procedures, such as bone expansion, bone splitting, Transalveolar sinus lift, implant bed preparation, and bone density enhancement.
1. INTRODUCTION
During the past decades, many surgical instruments have been invented to solve problems related to insufficient bone to dental implant placement, or for the purpose of facilitating the surgical procedure, making it more comfortable for the patient, and reducing the rate of complications. In situations where the quantity and quality of bone are suitable, standard implant kits are employed solely for the preparation of the implant bed. However, in other cases, alternative tools must be located to prepare the implant bed and adjust the shape and quality of the bone.
Threaded bone expanders (TBEs), bone spreaders, or screw-type expanders are important, indispensable tools with wide uses in dental Implantology. TBEs have many shapes and sizes, but in general, they are screw-like shapes, conical or cylindrical instruments with sharp or blunt tips. Due to their multiple uses, TBE kits have become an essential part of every dental implant system. This literature review enumerates all the details related to threaded bone expanders and their uses in implantology.
Threaded bone expanders were used first as an alternative to osteotomes in cases of expansion of the atrophic alveolar ridge [1]. Their use subsequently developed for many purposes, such as preparing the implant bed to increase initial stability and bone density and to elevate the sinus floor [2, 3]. Threaded bone expanders make it possible to rehabilitate complex areas, reversing the process of bone loss through the three-dimensional remodeling of the bone tissue architecture both qualitatively and quantitatively [4].
Generally, TBE kits include expanders of different diameters, point drills for initial marking, pilot drills for initial preparation of osteotomy, manual knob, handpiece latch adaptor, circular drill, and ratchet wrench extender (Fig. 1). Conical TBEs are preferred in expansion and splitting procedures, while cylindrical or straight TBEs are preferred in sinus lift and bone density-increasing procedures (Fig. 2) [4].
2. MATERIALS AND METHODS
2.1. Objective
The research aimed to provide a thorough review of threaded bone expanders, encompassing their historical use, types, mechanism of action, and clinical applications in the context of dental implants.
2.2. Research Design
A search was conducted on the internet using search engines, such as Google, Research Gate, PubMed, and PubMed Central. The search utilized keywords including bone expander, bone spreader, bone condenser, screw-type expander, and threaded bone expander. Articles meeting the criteria were included for review in (Table 1).
2.3. Inclusion & Exclusion criteria
2.3.1. Inclusion Criteria
Studies published in the English language and studies published until April 2024. Clinical studies, including randomized clinical trials, cohort studies, case reports, case series, and pilot studies, which included the use of threaded bone expanders in any dental implantology application.
3. RESULTS
Out of the initial 96 articles identified in the search, 29 studies met the inclusion criteria established for this review. These studies, which are listed in (Table 1), were thoroughly examined. Additionally, the full-text articles and reference lists of related studies were assessed to enhance the search process. Two reviewers independently conducted the evaluation of eligibility and data extraction.

General components of modern bone expander's kit.

Conical & cylindrical bone expanders (NX-BES, NexGen BioMedical, India).
4. DISCUSSION
4.1. Mechanism of Threaded Bone Expanders
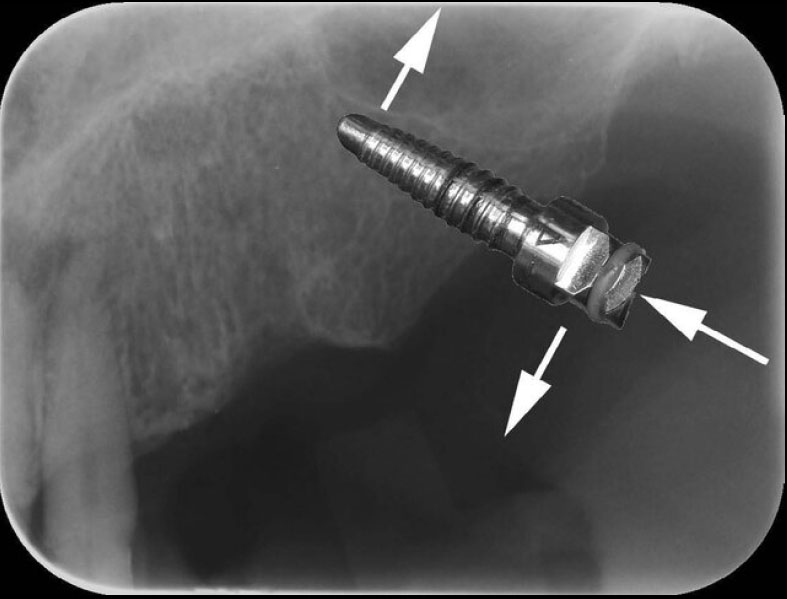
The operation principle applicable to TBEs is rotary and lever, that is, purely mechanical. The torque exerted on the square drive is transferred throughout the body of the instrument to the proximal end that operates in the surgical site, compacting the bone tissue [5]. The axial force applied to the expander causes a decomposition of the force's vector to two vectors: The axial vector and the other one is the tangent vector [6]. The axial vector leads to an apical progression of the expander, while the tangent vector leads to compression, expansion of bone plates, and increase of bone density (Fig. 3) [6].

The mechanism of bone expander.
| No | Authors | Year | TBEs Application |
|---|---|---|---|
| 1 | Abdulhalim et al [20] | 2020 | Bone splitting |
| 2 | Albash et al [31] | 2023 | Transalveolar sinus lift |
| 3 | Albash et al [32] | 2023 | Transalveolar sinus lift |
| 4 | Anitua et al [26] | 2017 | tooth autotransplantation |
| 5 | Bassi et al [5] | 2016 | sinus by-pass |
| 6 | Bassi et al [6] | 2016 | sinus by-pass |
| 7 | Cortes et al [16] | 2010 | Bone expansion |
| 8 | Eldibany et al [23] | 2014 | IAN lateralization |
| 9 | Eldibany et al [28] | 2015 | Preparation of one-piece implant sites |
| 10 | Elkholy et al [21] | 2021 | Bone splitting |
| 11 | Elsyad et al [12] | 2017 | Bone expansion |
| 12 | Gupta et al [15] | 2011 | Bone expansion |
| 13 | Hamdan et al [19] | 2021 | Bone splitting |
| 14 | Hamzah et al [22] | 2021 | Bone splitting |
| 15 | Kadkhodazadeh et al [3] | 2020 | Transalveolar sinus lift |
| 16 | Kelly et al [17] | 2013 | Bone expansion |
| 17 | Kim et al [14] | 2014 | Bone expansion |
| 18 | Kurtzman et al [27] | 2012 | Immediate implant placement at septa |
| 19 | Lee et al [1] | 2006 | Bone expansion |
| 20 | Manekar et al [7] | 2022 | ARSE |
| 21 | Nishioka et al [2] | 2009 | Bone spreading |
| 22 | Omar et al [24] | 2020 | Basal implant bed preparation |
| 23 | Rahal et al [13] | 2018 | Bone expansion |
| 24 | Rambla et al [11] | 2006 | Implant bed preparation |
| 25 | Rodriguez et al [10] | 2013 | IAN lateralization |
| 26 | Rodriguez et al [18] | 2015 | Bone expansion |
| 27 | Siddiqui et al [4] | 2006 | Bone expansion |
| 28 | Singhal et al [25] | 2018 | Implant bed preparation in the nasopalatine foramen |
| 29 | Sonick et al [29] | 2020 | Transalveolar sinus lift |
The effect of threaded bone expanders can be classified based on bone response into osteo-condensation and osteo-mobilization [7]. The principle of osteo-condensation, initially described by Tatum and later by Summers [8, 9], involves avoiding bone removal, lateral compression, and condensation of cancellous bone. The osteo-mobilization involves lateral displacement of buccal cortical bone or sinus floor [3, 7]. The osteo-condensation concept is employed in expansion, ARSE, implant bed preparation, and spreading procedures, while the osteo-mobilization concept is employed in splitting inferior alveolar nerve (IAN) lateralization and transalveolar sinus lift procedures [7, 10].
The key factors affecting bone response to threaded bone expanders are the thickness of the cortical bone, especially on the buccal aspect, and the thickness and quality of cancellous bone. Threaded bone expanders carry out the condensation of the cancellous bone as a result of the absorbed part of the centripetal pressure generated by the expander. ARSE classified the mandible into five types based on the thickness of the buccal thickness cortex [7]. The authors suggested that the implant sites of Type 4 are difficult to expand and do not respond to osteo-condensation. Threaded bone expanders, along with osteo-mobilization are recommended in Type 4 alveolar bone. Other types of alveolar bone in the mandible respond well to the threaded bone expanders [7].
4.2. Applications of Threaded Bone Expanders
Threaded bone expanders (TBEs) were initially used for the expansion of narrow ridges with great success because of their atraumatic nature. In addition, the manual technique takes advantage of the natural elasticity of the bone, thus allowing expansion of the ridge and, at the same time, condensation of trabecular bone, which increases bone density, leading to enhanced osteo- integration of dental implants [3, 11]. TBEs are similar in shape to dental implants; they are simply screws made of stainless steel. Therefore, we believe that the invention of TBEs came after observing the expanding effect of dental implants when inserted with high insertion torques.
During a comprehensive review of the literature, we found many applications for TBEs, including alveolar ridge expansion, alveolar ridge splitting, inferior alveolar nerve lateralization, dental implant site preparation at low-density bone, preparation of implant site in special regions, and transalveolar sinus lift (Fig. 4).
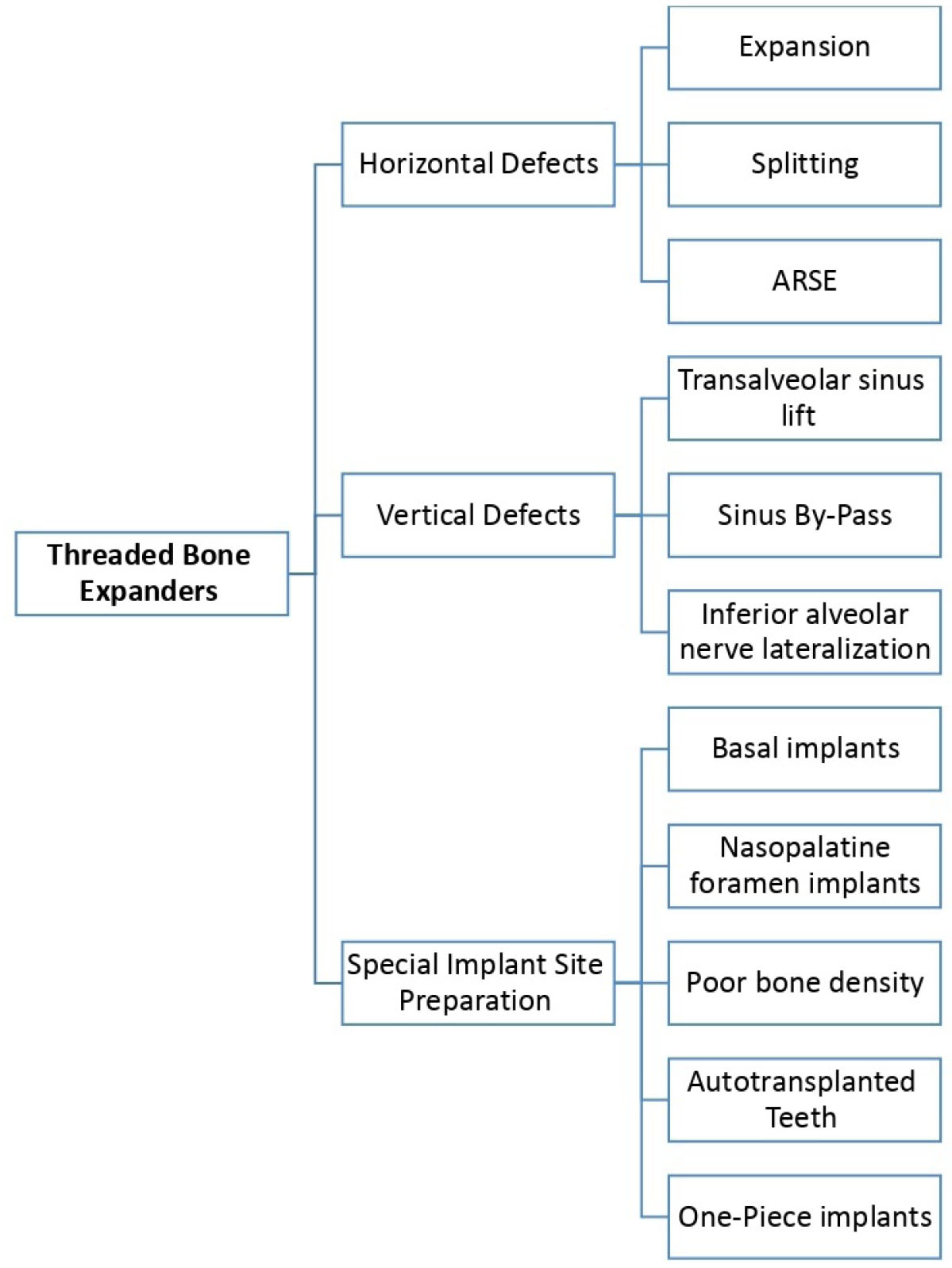
A flow chart for uses of threaded bone expanders.
4.2.1. Alveolar Ridge Expansion and Splitting
During the past decades, threaded bone expanders have been used in the management of narrow alveolar ridges and horizontal bone defects in all regions of the upper and lower jaws (Fig. 5) [12-20]. Management of narrow alveolar ridges using expansion and splitting techniques requires several conditions, including [1, 4, 7, 18]:
1. Sufficient bone height.
2. Broad basal bone.
3. Low bone density.
4. Thin cortical bone plates.
5. Alveolar ridge width between 3-6 mm.

Bone splitting using bone expanders [22].
In this field, three techniques that are broadly similar in purpose but technically different can be distinguished [7]:
- Bone Expansion.
- Bone splitting.
- Alveolar ridge split and expansion (ARSE).
Bone splitting procedures usually include making a midcrestal horizontal osteotomy with two vertical osteotomies, while ARSE procedures include only midcrestal horizontal osteotomy [7]. Bone Expansion is a surgical technique to expand the alveolar ridge without any horizontal or vertical osteotomies [7].
Bone expansion is a highly predictable, relatively complication-free technique using TBEs without any horizontal or vertical osteotomies. The use of threaded bone expanders results in lateral bone augmentation and condensation of soft bone to increase bone volume and density necessary for successful implant placement [2].
The alveolar ridge split and expansion (ARSE) technique is used in the management of horizontally deficient (narrow) alveolar ridge with optimum bone height [7]. ARSE was combined between the use of TBEs and crestal osteotomy only [7]. This technique depends on the osteo-condensation method instead of osteo-mobilization to expand the alveolar ridge [7]. The minimally invasive technique of one-stage ARSE performed with motorized ridge expanders (MRE) and insertion of implant in the same operative procedure decreases the morbidity, treatment time, number of surgical procedures, and the risk of complications, thereby increasing the patient acceptance [7].
For retention overdentures, conical threaded bone expanders were used to split the alveolar ridge in the anterior region in the mandible after making a deep horizontal cut using the piezoelectric device [Exp 1]. Conical threaded bone expanders were also used to expand the anterior region of the maxilla. The use of threaded bone expanders can be combined with guided bone regeneration techniques in some cases, such as buccal bone cracks and buccal malfracture [16].
Threaded bone expanders can also be used for guided splitting and expansion procedures. This technique either allows for flapless split [21] of the buccal bone using midcrestal mesiodistal osteotomy and chisel, then continuous with threaded bone expansion, or with full thickness flap [22]. Threaded bone expanders were used for the expansion of the alveolar ridge in the anterior region of the maxilla with a surgical guide in a flapless approach [22].
4.2.2. Inferior Alveolar Nerve Lateralization
Threaded bone Expanders were used for inferior alveolar nerve lateralization by ridge splitting of the body of the mandible followed by lateral displacement of the cortical plate that contains the neurovascular bundle [10, 23]. This technique allows for installing wider, longer, and greater numbers of implants over the entire bony height of the mandible and achieving greater implant primary stability with a tricortical anchorage (buccal, lingual, and inferior) [10]. Regarding possible complications, IAN lateralization using threaded bone expanders is less traumatic than the conventional IAN lateralization technique (no direct instrument contact with IAN); therefore, the risk of permanent neurological dysfunction is minimal (0.7%) [10, 23].
4.2.3. Implant Site Preparation
Many studies have confirmed the capacity of threaded bone expanders to prepare osteotomy sites in both jaws, which cannot be prepared conventionally [12, 13]. The properties of these expanders forced the practitioners to employ them in some cases, including:
1- Basal implant bed preparation in the posterior region of the mandible [24].
2- Implant bed preparation in the nasopalatine foramen in the anterior region of the maxilla [25].
3- In the field of tooth autotransplantation, in which motorized threaded bone expanders were used to prepare the alveolus (bed of auto transplanted tooth) [26].
4- Immediate implant placement at septa of maxillary molars, using Manual threaded bone Expanders [27].
5-Preparation of immediate loading one-piece implant sites using Manual threaded bone Expanders [28].
6- Titled implant bed preparation in close proximity to the anterior sinus wall. This technique is also called Sinus by-pass [5, 6]. The titled implant bed was prepared parallel to the anterior wall of the sinus in cases where the angle was small (<30) [5]. If the angle is large, the axis is adjusted (deforming the anterior wall of the sinus) by applying a controlled force on the head of the contra-angle handpiece [5, 6] (Fig. 6).
7- Threaded bone expanders were also proposed to increase bone density in cases of bone type D4 as an alternative to the ridge expansion osteotomy technique. TBEs eliminate the percussive trauma caused by the hammering of osteotomes, considerably reducing the discomfort for the patient and simplifying the instrumental access in the posterior region of the jaws [3, 4, 11].
Sinus by-pass technique using bone expanders [6].
Transalveolar sinus lift using bone expanders [31].
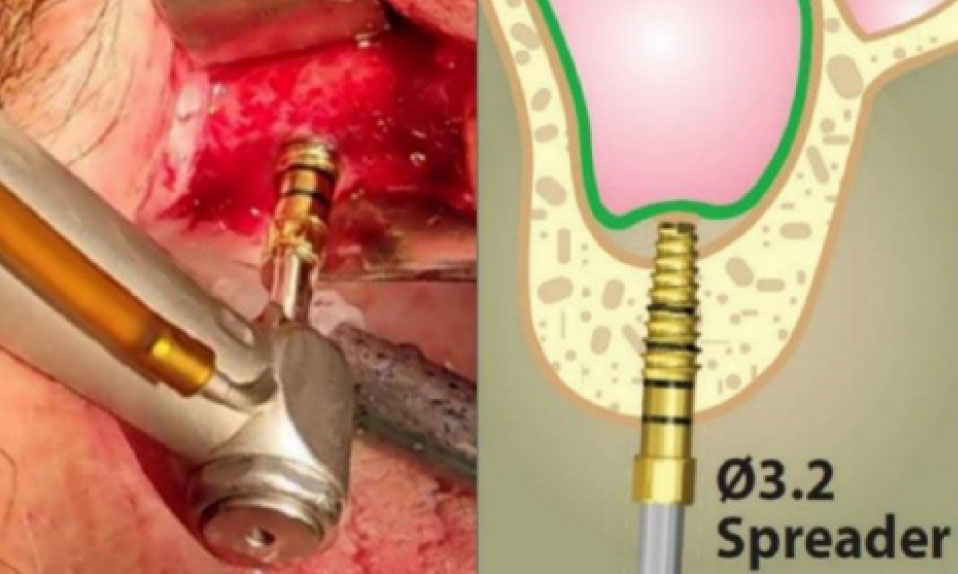
4.2.4. Transalveolar Sinus Lift
Threaded bone expanders were used to elevate the maxillary sinus floor with or without bone graft materials, manually or motorized (Fig. 7) [3, 29-31]. Threaded bone expanders demonstrated the capacity to effectively and safely move the cortical plate of the sinus floor, similar to the summer's technique and without using the hammer [3, 29, 30]. Transalveolar sinus lift using threaded bone expanders combines the advantages of osteotome-based techniques (no direct instrument contact with the sinus membrane) and the advantages of non-osteotomy-based techniques (eliminating hammering). The concept of this technique is based on the use of sequential expanders into the implant bed and pushing the sinus floor up in a vertical direction [30, 31].
4.3. Advantages and Disadvantages
4.3.1. Advantage of Threaded Bone Expanders
The advantages of threaded bone expanders are as follows:
1- They offer a simple and minimally invasive alternative to many instruments, which are used in the same indication, such as osteotomes, chisel, and mallet [4, 30].
2- TBEs transmit relatively low amounts of force compared to other instruments [4, 6].
3- TBEs utilize gradual and control force. TBEs are considered to be more effective in preventing buccal cortical bone fractures [4, 6, 30].
4- They require less time from first surgery to final restoration since they allow immediate placement of implants in narrow ridges at the time of expansion [4].
5- TBEs can be used in all regions of the jaws and can be used with different commercially available implant systems [12-20].
6- TBEs tap the implant site, which facilitates implant insertion [1, 4, 5, 10].
4.3.2. Disadvantage of Threaded Bone Expanders
The disadvantages of threaded bone expanders are as follows:
1-Using of TBEs in expansion and splitting procedures may be associated with some complications, such as bone cracks and buccal malfracture [16]. These complications occur when the threshold of bone elasticity is exceeded. Therefore, the case must be carefully selected in terms of width, thickness of cortical plates, and density of trabecular bone.
2- The preparation of implant beds using TBEs increases insertion torque. However, high insertion torque can generate micro cracks that could result in the progression of marginal bone loss [33].
3- High primary stability may be false. Many studies have confirmed that initial stability is high only during the first weeks of dental implant placements, while initial stability due to bone molding decreases during subsequent weeks. These studies have proven that the secondary stability values when using TBEs are lower than their counterparts when using other techniques, such as osseodensification [34].
CONCLUSION
Threaded bone expanders are essential tools in the field of implant dentistry, particularly in cases where the available bone lacks ideal density and quantity. These versatile tools are successfully used in procedures, such as bone expansion, bone splitting, transalveolar sinus lift, implant bed preparation, and bone density enhancement.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| TBE | = Threaded bone expander |
| TBEs | = Threaded bone expanders |
| ARSE | = Alveolar ridge split and expansion |
| IAN | = Inferior alveolar nerve |
| MRE | = Motorized ridge expander |
| MREs | = Motorized ridge expanders |

