All published articles of this journal are available on ScienceDirect.

Perceptions of Fluoride and Fluorosis among Saudi Community
Authors Info & Affiliations
Abstract
Introduction
Fluoride has been used in dentistry for a few decades to prevent dental caries, as it is a double-edged sword in nature. When a human being is exposed to more than normal fluoride levels, fluoride toxicity or fluorosis occurs. The study aimed to analyze Saudi community knowledge and views about the relevance of oral fluoride and its repercussions on health.
Material and Methods
A cross-sectional survey was distributed to 1020 Saudi people of both genders. The electronic survey was sent through social media. The questionnaire was written in Arabic and comprised 10 close-ended questions. Data was entered, cleaned, and analyzed with the SPSS 23.0 version, and necessary statistical tests like proportions and the chi-square test were performed.
Results
A total of 1020 participants participated in the study, with an age group ranging from 15 to 66 years. Most respondents were female (72.5%/), and 27.5% were male. The study survey showed that 42.8% of participants visited a dentist within the last six months. More than half of the participants (53.7%) brushed their teeth twice a day, 41.4% noted the appearance of a white spot on their teeth, and 65.9% reported a discoloration on their teeth. More than half of the people (56.7%) were aware that fluoride is significant in protecting and enhancing teeth. On the other hand, 78% of participants did not know that excessive exposure to fluoride during childhood could cause fluorosis.
Conclusion
According to this study, a substantial number of people are aware of the importance of oral care and fluoride. They were also mindful of teeth discoloration and how it affects their life. However, most participants and their parents were still unaware of the causes of fluorosis and its treatment.
1. INTRODUCTION
Decades ago, fluoride use started in dentistry, and worldwide, it has been considered for the prevention of dental caries. It has a long history of use in some countries through water fluoridation as a community health intervention [1]. In the early eighties of the last century, fluoride had begun to be prescribed topically for oral hygiene in various ways, including toothpaste, mouth- washes, gels, and varnishes. The mechanism of preventing caries is by creating a remineralized coat resistant to acid assault and by inhibiting microbial enzymes that produce the acid. This process promotes remineralization and stops or reduces demineralization in dental enamel or dentin [2]. Rigorous evidence over several decades has shown that there is a safe and successful method to control the prevalence of caries. The efficacy of this mechanism is through frequent daily contact between fluoridated water and teeth or when reallocated orally in saliva.
Conversely, when a human being is exposed to more than normal fluoride levels, fluoride toxicity or fluorosis occurs. This risk is usually in childhood before the eruption of permanent teeth or sometimes even before birth through the mother’s fluoride exposure. Fluorosis is the disturbance of teeth tissue that appears in the form of white markings on teeth in mild cases and pitting and intrinsic staining by yellow and brown discoloration in severe ones [3].
Research has shown that caries' prevalence has declined, but dental fluorosis's development has increased. This occurred due to water fluoridated programs exceeding the optimal level in the beginning. Moreover, studies have reported increased dental fluorosis caused by excessive contact with topical fluoride toothpaste and systematic fluoride.
This investigation describes the prevalence and severity of dental fluorosis among children born between 1986 and 1987 and 1999 and 2004 in the United States [4]. Dental fluorosis is a dental community health issue in Saudi Arabia. Based on the systematic review, the prevalence and severity of dental fluorosis fluctuate from region to region and differ from rural to urban. This review recommended more studies in every area in Saudi Arabia, so implementation, prevention, and awareness of fluoride and fluorosis rely on the findings of each city [5].
Hence, the present study was planned to evaluate the perceptions among the Saudi Arabian community about the importance of dental fluoride, its consequences, treatment options, and implementation of health promotional measures.
2. MATERIALS AND METHODS
2.1. Study Design and Target Population
A cross-sectional survey of people in the Kingdom of Saudi Arabia was conducted. The present study was executed at Qassim University's College of Dentistry from January 2021 to May 2021, with permission from the College of Dentistry Research Center. The institutional ethics committee granted authorization to perform the study, and after clearance, a self-administered survey was used to collect data via an online social media platform. Various internet tools, such as WhatsApp, Twitter, and Snapchat, were used to publicize the need for research and solicit responses to the questionnaire.
2.2. Sampling
The sample size was calculated using the Openepi sample size calculator based on the following parameters: Saudi Arabia's population was 35 million, the assumed anticipated prevalence was 50%, the confidence interval was 95%, the design effect was 1.0, and the estimated sample was 385. One thousand and twenty samples were collected to maintain the study's accuracy. The convenience sampling method was applied to collect the data in this research.
2.3. Data Collection Tool
Information on sociodemographic variables, including gender and age, was included in the questionnaire. The inclusion criteria for participants were adolescents (more than 15 years of age) and adult Saudi people of both genders. The exclusion criteria included non-Saudi and children less than 15 years old. The questionnaire was written in Arabic and comprised 10 close-ended questions about people's personal and habitual information: gender, age, oral hygiene, water source, dental clinic visit, and family history. The second part recorded people's background in the knowledge of fluoride and fluorosis disease. On a sample of 10 participants, the pilot testing of the questionnaire was performed for clarity and organization, and the KMO and Bartley test was used to assess the survey's item validity.
2.4. Statistical Analysis and Ethical Considerations
When the appropriate sample size was obtained, the data were statistically analyzed using the Statistical Package for the Social Sciences (SPSS Inc.; Windows version 23, Chicago, Illinois, United States). For the statistical comparison of categorical variables and the variations among the groups, the chi-square test was employed. Significant results were defined as those with a p-value less than 0.05. An ethical committee approval certificate was obtained from the College of Dentistry, Qassim University, on 20.04.2020, with approval number EA/M – 2020-3014.
3. RESULTS
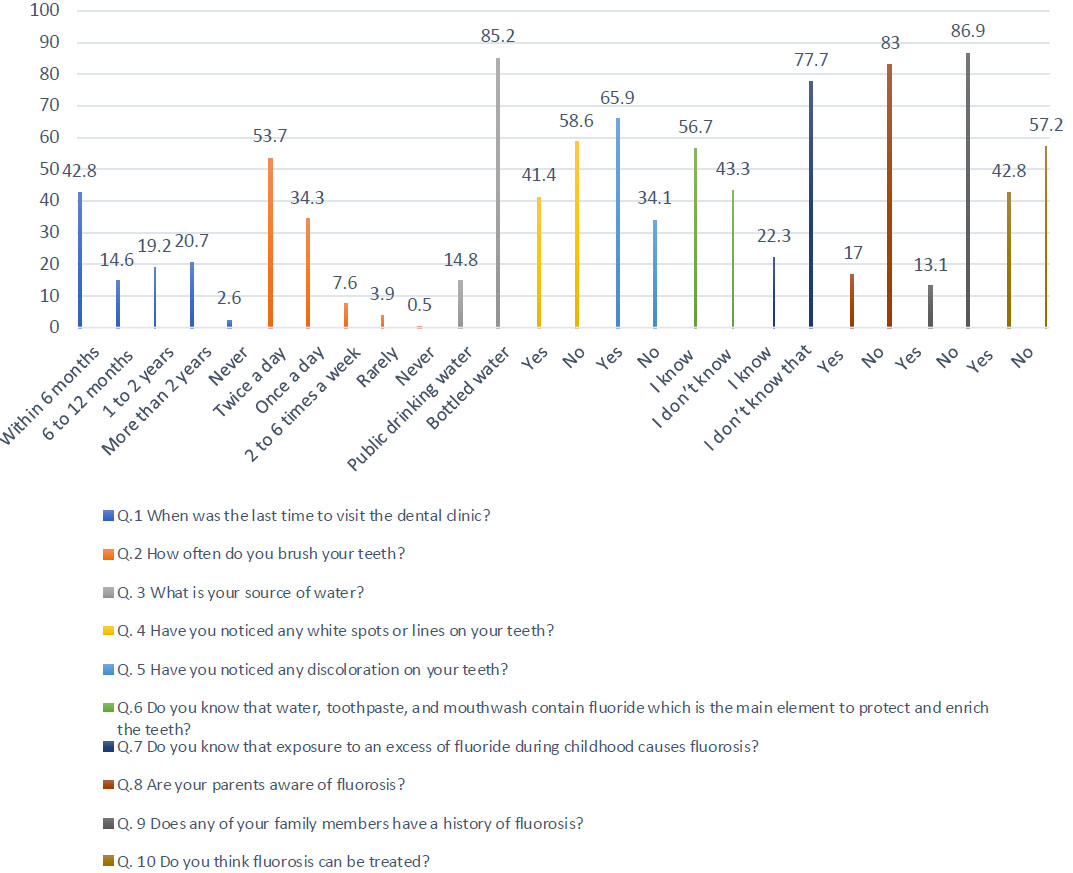
As illustrated in Table 1 and Fig. (1), a total of 1020 participants took part in the study, with an age group ranging from 15 to 66 years. Most respondents were female (72.5%/), and 27.5% were males. The study survey showed that 42.8% of participants visited a dentist within the last six months for either a dental exam or emergency visit, while the previous visit of the other participants was more than six months. Regarding their brushing habit, more than half of the participants (53.7%) brushed their teeth twice daily, while one-third (34.3%) brushed once daily. Most respondents (85.2%) drank bottled water, and 14.8% drank public drinking water. For the participants’ observation of any sign or color abnormalities in their teeth, 41.4% of them noted a white spot appearance on their teeth, and 65.9% reported a discoloration on their teeth.
| Question | Gender | Total | X2 | p-value | |
|---|---|---|---|---|---|
| Male | Female | - | - | - | |
| Q.1 When was the last time to visit the dental clinic? | |||||
| Within 6 months | 104 (10.2) | 333 (32.6) | 437 (42.8) | 111.47 | 0.00 |
| 6 to 12 months | 10 (1.0) | 139 (13.6) | 149 (14.6) | ||
| 1 to 2 years | 42 (4.1) | 154(15.1) | 196 (19.2) | ||
| More than 2 years | 109 (10.7) | 102 (10.0) | 211 (20.7) | ||
| Never | 15 (1.5) | 12 (1.2) | 27 (2.6) | ||
| Q.2 How often do you brush your teeth? | |||||
| Twice a day | 93 (9.1) | 455 (44.6) | 548 (53.7) | 84.76 | 0.00 |
| Once a day | 123 (12.1) | 227 (22.3) | 350 (34.3) | ||
| 2 to 6 times a week | 45 (4.4) | 33 (3.2) | 78 (7.6) | ||
| Rarely | 17 (1.7) | 22 (2.2) | 39 (3.9) | ||
| Never | 2 (0.2) | 3 (0.3) | 5 (0.5) | ||
| Q. 3 What is your source of water? | |||||
| Public drinking water | 81 (7.9) | 70 (6.9) | 151 (14.8) | 55.210 | 0.00 |
| Bottled water | 199 (19.5) | 670 (65.7) | 869 (85.2) | ||
| Q. 4 Have you noticed any white spots or lines on your teeth? | |||||
| Yes | 41 (4.0) | 381 (37.4) | 422 (41.4) | 125.08 | 0.00 |
| No | 239 (23.4) | 359 (35.2) | 598 (58.6) | ||
| Q. 5 Have you noticed any discoloration on your teeth? | |||||
| Yes | 98 (9.6) | 574 (56.3) | 672 (65.9) | 158.88 | 0.00 |
| No | 182 (17.8) | 166 (16.3) | 348 (34.1) | ||
| Q.6 Do you know that water, toothpaste, and mouthwash contain fluoride which is the main element to protect and enrich the teeth? | |||||
| I know | 90 (8.8) | 488 (47.8) | 578 (56.7) | 94.923 | 0.00 |
| I don’t know | 190 (18.6) | 252 (24.7) | 442 (43.3) | ||
| Q.7 Do you know that exposure to an excess of fluoride during childhood causes fluorosis? | |||||
| I know | 70 (6.9) | 157 (15.4) | 227 (22.3) | 1.653 | 0.206 |
| I don’t know that | 210 (20.6) | 583 (57.2) | 793 (77.7) | ||
| Q.8 Are your parents aware of fluorosis? | |||||
| Yes | 38 (3.7) | 135 (13.2) | 173 (17.0) | 3.267 | 0.092 |
| No | 242 (23.7) | 605 (59.3) | 847 (83.0) | ||
| Q. 9 Does any of your family members have a history of fluorosis? | |||||
| Yes | 32 (3.1) | 102 (10.0) | 134 (13.1) | 1.012 | 0.351 |
| No | 248 (24.3) | 638 (62.5) | 886 (86.9) | ||
| Q. 10 Do you think fluorosis can be treated? | |||||
| Yes | 80 (7.8) | 357 (35.0) | 437 (42.8) | 33.075 | 0.00 |
| No | 200 (19.6) | 383 (37.5) | 583 (57.2) | ||
| Total | 280 (27.5) | 740 (72.5) | 1020 (100.0) | ||
More than half of the people (56.7%) were aware that fluoride is the main element of water, toothpaste, and mouthwash and has significance in protecting and enhancing the teeth. On the other hand, 22.3% of participants and their parents (17.0) knew that excessive exposure to fluoride during childhood could cause fluorosis. In this study, 13.1% mentioned having family members with a fluorosis history. When exploring the awareness about fluorosis treatment, 42.8% thought that fluorosis could be treated, while 57.2% did not. 42.8% of the respondents who believed fluorosis could be treated were not aware of the treatment options available.
4. DISCUSSION
Fluoride concentration in water has decreased the prevalence of dental caries. Although a precise dose of fluoride must not exceed every liter of water, the prevalence of dental fluorosis will have a negative impact. Topical fluoride, such as toothpaste, can be another cause of fluorosis when children tend to swallow it. Thus, water fluoridation has a valuable effect on public health and protects and enhances teeth as long as fluoride is within the range of 0.7mg -1mg per liter of water, as the World Health Organization recommended in 1994 [6]. A systematic review including more than 3000 studies on the dental or general health effects of water fluoridation in York concluded that there was no clear evidence of any adverse effect other than dental fluorosis [7].
This study identified two main drinking water sources: bottled and public drinking water. Interestingly, this study showed a significant shift (85.2%) from public drinking to bottled water. In a survey conducted in 2003, it was reported that the primary source of drinking water in Saudi Arabia at that time was groundwater [8]. This major shift could justify the decrease in fluorosis prevalence in the study. In the conclusion of the review, since bottled water was the first drinking source in Saudi Arabia, Madinah province was shown to have the most negligible rates of individuals affected by fluorosis [5].
Knowledge of the fluoride content of drinking water, either public or bottled, is essential at all community levels since another study in Saudi Arabia reported that the content of various bottled water differs in the fluoride concentration but is within a safe range [9]. It is essential for the public community to know the difference and to be aware of the consequences of the increase in the concentration of fluoride [9]. Therefore, a recent and accurate assessment of the population's current fluoride intake habits will be necessary to organize preventive dental programs and prescribe fluoride supplements.
In this study, 13.1% of participants reported that some of the family members had fluorosis; this was consistent with another study by Albanian et al., where they reported the prevalence of fluorosis to be 14% in Riyadh, Saudi Arabia. However, another study conducted in another region (Qassim region) in 2000 showed an increase in the prevalence of fluorosis to 24-67% [5]. The difference can be explained by the different fluoride concentrations in public water in various cities of the Kingdom. In contrast, other studies have shown that the prevalence of fluorosis in rural areas tends to be higher than in urban regions of AL Qassim province [10].
A comprehensive survey in Saudi Arabia discovered that 12 percent of those older than 15 saw a dentist regularly in the previous year, with 50 percent doing so for a particular area of concern. A different finding was reported in this study since 42.8% of participants underwent dental exams within the last 6 months. Still, it could not be measured whether this visit was due to regular checkups or specific complaints. Regular dentist visits can enhance patients’ awareness of fluoride and other important oral hygiene instructions [11]. Saudi Arabians rarely follow good oral hygiene, and they seldom use medical services to prevent mouth diseases. This is not true in this study since around 88% of participants brushed their teeth once or twice a day.
However, there is a limitation to this since the majority of the study’s participants were female. Usually, females have better oral hygiene than males, which could bias the findings of this part of the study. Another study showed similar findings regarding oral hygiene practices, whereas 72% reported brushing at least once daily [11]. According to a study in India, around 85% of the population is aware of the use of fluoride [12]. Another study found that Scandinavian nations had higher oral fluoride awareness than other developing nations [6]. In this study, fifty percent of the sample population knew fluoride's use and significance.
The general public needs to understand fluoride and its different sources for better dental hygiene. Therefore, public awareness is crucial to advance dental care and know the various sources of fluoride. Children's dental health is correlated with their parents' oral health knowledge. Targeting parental oral health knowledge and habits may be crucial in preventing oral health issues like dental fluorosis since parents have a significant role in influencing children's development in the early years. In this study, 77.7% of participants and their parents (83%) did not know that excessive exposure to fluoride during childhood might cause dental fluorosis.
According to studies conducted in Pakistan, most parents were less aware of dental fluorosis. Additionally, the findings indicated that parental knowledge of dental fluorosis was substantially correlated with children's fluorosis status [13]. However, in the study aiming at community awareness of fluoride in Northern Tanzania, most (77%) of the participants reported that their children had discoloration on their teeth, and 84.93% of the respondents were using fluoride toothpaste. Children were not helped or observed while using fluoride toothpaste, which could lead to swallowing the toothpaste and increasing the amount of fluoride, leading to fluorosis [14]. As an illustration, most children and their parents in the study conducted in Pakistan had little knowledge about fluorosis. Around 84.8 percent of parents lacked trust in their kids' fluorosis status, and 87.3% had never heard of it [13].
The KSA Ministry of Health should create and implement programs to raise oral health awareness. All primary health clinics should incorporate these programs into their ongoing outreach efforts. Additionally, programs to raise public awareness of the value of oral health are required to lessen the financial and human costs of oral disease in the future.
Nowadays, people have become more aware of teeth discoloration, and it has become a point of concern. For instance, in this study, 65.9% of participants noticed some discoloration, and 58.6% reported that they had white spots. One study that evaluated children's esthetics found that fluorosis was easily seen in its milder forms; other research studies have mentioned that fluorosis can be a concern in severe stages [15]. This worry may significantly impact the quality of those affected by this condition.
Sigurjons et al., in the United Kingdom, discovered that parents of children with significant fluorosis in their teeth felt guilty and expressed disapproval about the color of the teeth of their offspring. Another study on children's esthetics in Mexico revealed their dissatisfaction with the shade of their teeth. Given this awareness of the problem and comprehension of its effects, behavioral guidelines that will be helpful for determining future dental and psychological care related to fluorosis must be established [16]. In this study, more than half of the participants were not aware that there was a treatment for fluorosis. Fluorosis can be treated in all its forms, mild or severe.
One systematic review showed that fluorosis treatment could range from minimally invasive therapies like resin infiltration, bleaching, and micro abrasion to more invasive treatments like crowns and veneers. This can be planned by making a proper diagnosis to determine the stages of fluorosis based on the fluorosis index [17-20]. The major strength of this study was a large sample of 1020 during the COVID-19 period, despite lockdowns, quarantine, and isolation of patients and other people. The study's limitation was that the discoloration of the teeth was taken as fluorosis; it could be due to intrinsic or extrinsic causes, whereas in-depth analysis is difficult in the population.
CONCLUSION
Based on the study findings, awareness of the significance of fluoride and good oral hygiene was observed in many people. Also, the study population was aware of teeth discoloration and how it affects their life. Only four out of ten (42.8%) people knew that fluorosis could be treated. However, most participants and their parents were still unaware of the causes of fluorosis and its treatment.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
ABBREVIATION
| SPSS | = Statistical Package for the Social Sciences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
An ethical committee approval certificate was obtained from the College of Dentistry, Qassim University, on 20.04.2020, with approval number EA/M – 2020-3014.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.

