All published articles of this journal are available on ScienceDirect.

Cone Beam Computed Tomography Analysis of Post Space in Bifurcated Premolars Using ParaPost and Peeso Reamer Drills
Authors Info & Affiliations
Abstract
Introduction
Core buildups are usually maintained by the usage of posts. Even so, in curved and narrow canals, such as bifurcated premolars, excessive dentin removal during post-space preparation can result in a vertical root fracture or perforation. In order to preserve root canal dentin during post-space preparation of bifurcated premolars, this study examined and analyzed the effects of two widely used drills: Peeso Reamer (Dentsply Maillefer, Ballaigues, Switzerland) and ParaPost (Coltene/Whaledent, Inc., Altstätten, Switzerland). We also examined the risks associated with using Cone-beam Computed Tomography (CBCT).
Methods
Three operators with varying levels of experience treated a total of 72 removed bifurcated premolars, dividing them into equal groups. The rotary ProFile system (Dentsply Sirona, Charlotte, NC) was utilized for root canal treatments, and gutta-percha size #30/0.4 was used for obturation. Peeso Reamer #2 and ParaPost #1 were then used to prepare the palatal canals. CBCT was used to assess the total mean intracanal spaces of 3 mm, 5 mm, and 7 mm that were measured both preoperatively and postoperatively. To compare the mean dentin thickness within the canal area across all groups, we used analysis of variance testing. We detected complications, like deviations or perforations, using mesiodistal periapical radiographs.
Results
When utilizing the Peeso Reamer, the mean dentin thickness (0.749 mm) was slightly more than when using the ParaPost (0.736 mm) with p=0.16. There was no significant difference in the mean dentin thickness of the canal area between the Peeso Reamer and the ParaPost drills. The Pesso Reamer drill had fewer complications since it matched the canal configuration, while the Parapost drill removed somewhat more dentin in the canal area. Only seven teeth with minimum deviation from the center of the canal during preparation were produced by the Peeso Reamer drill (20% of teeth having deviation), whereas twenty-one teeth had deviations (72.2% of teeth) and eight had furcal perforations generated by the ParaPost.
Conclusion
Within the limitations of our study, the Pesso Reamer drill caused little more dentin removal than the ParaPost drill. However, the Peeso Reamer had fewer risks and was safer to use in bifurcated premolars. The ParaPost drill is not recommended in bifurcated premolars due to the high risks of deviation and perforation because they have narrow canals. The selection of an appropriate drill for post-space use in bifurcated premolars is essential for successful patient outcomes.
1. INTRODUCTION
Posts are commonly utilized in dentistry as a means of retaining core build-up. Maintaining the original canal form with less intrusive procedures leads to better endodontic outcomes [1]. For various post sizes to be accessible, root canals must be enlarged by eliminating intra-radicular dentin obstruction [2]. On the other hand, extensive dentin removal from cervical preflaring may result in concavity perforation in the furcation zone, particularly in curved and narrow canals [3].
Premolars are the teeth most frequently linked to clinical issues and vertical root fractures due to their canals' anatomical structure and thin roots [4]. According to research conducted in vitro and clinical studies, the amount of intracanal residual dentin that persists after endodontic treatment directly correlates with the longevity of teeth repaired with posts [5] [6]. Blount et al. reported that premolars accounted for 60.4% of vertical fractures, incisors for 22.6% of vertical fractures, and molars for 13.2% of vertical fractures [7]. Mesiobuccal roots of maxillary teeth and mesial roots of mandibular molars and mandibular incisors are more prone to fracture than other teeth when they have flat or thin roots with small mesiodistal and oval diameters in the bucco-lingual direction [8]. According to Testori et al., premolars are the teeth with the highest frequency of vertical root fractures after endodontic therapy [9].
It is not necessary to remove more dentin during the post-preparation of the root canal as this can decrease fracture resistance, especially in premolars. Different rotary instruments have been developed in response to the demand for new tools that enable proper cervical preparation.
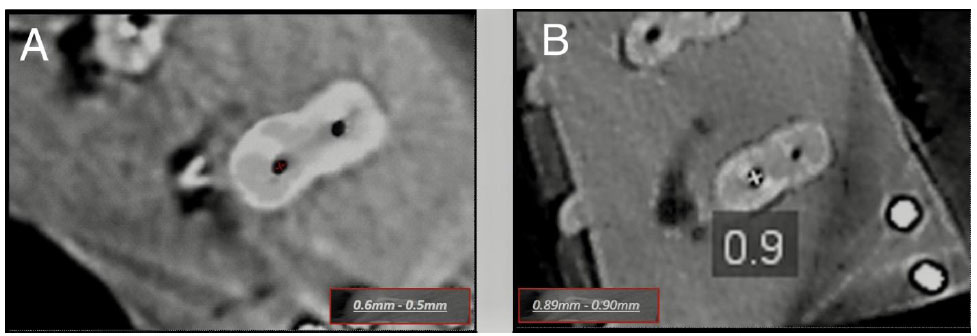
In this work, the ParaPost (brown) (Coltene/ Whaledent, Inc., Altstätten, Switzerland) size #1 and the Peeso Reamer (Dentsply Maillefer, Ballaigues, Switzerland) drill size #2 were used to measure the intracanal dentin removal in the roots of premolars after preparation. The instruments' designers believe that the application of nanotechnology strengthens the stainless steel and minimizes friction when the environment is dry. The diameters of the ParaPost drill size #1 (brown) and the stainless-steel size #2 Peeso Reamer are 0.90 mm, according to the manufacturer's specifications.
Using large diameters may increase the chance of a striping hole in the root canal by causing substantial dentin loss, specifically at the furcal aspect of the root canal [10]. The purpose of this study was to examine the impact of the two drills on the canal dentin during post-space preparation of bifurcated premolars using Cone-beam Computed Tomography (CBCT), because dentin inside the canals is critical for fracture resistance.
2. MATERIALS AND METHODS
This study received ethics approval with number KACST, KSA: H-01-R069. A sample of seventy-two human premolars with two separated roots that were previously kept in 10% buffered formalin solution for no more than six weeks after being taken out of the tooth bank was chosen. At first, the roots were examined under a microscope to rule out teeth that had cracks. Each tooth was placed on a tray (Fig. 1) containing a silicon rubber base (Zetaplus Putty C-Silicone Dental Impression Material, Zhermack GmbH, Marl, Germany).

One millimeter above the cementoenamel junction, the crowns of the teeth were sectioned. Weine's 1982 approach was used to calculate the curvature angle of the roots using a digital radiograph with mesial angulation [11]. Teeth that deviated from the canal's center by more than five degrees were excluded. Using an identical rotary file system (ProFile), root canal treatment was performed on all teeth. A patency K-file size #15 (Dentsply Sirona, Charlotte, NC) was passively inserted into the canal until it was visible from the apical foramen. A working length of 0.5 mm was chosen. The palatal canal was obturated with a single cone, utilizing the same master cone (gutta-percha size #30/0.4) to ensure consistency. We selected the palatal canal because numerous studies have shown that the lingual root should be used and the buccal root should be avoided in multirooted premolars when a post is required [12]. The teeth were assigned randomly and categorized into three groups, A, B, and C. Each group was given a stainless steel Peeso Reamer drill size #2 and a ParaPost drill size #1 (brown color) for post-space preparation. An advanced restorative specialist male 36-year-old practitioner working in a public hospital with eleven years of experience prepared group A teeth. A 29-year-old male recent graduate working in a public hospital prepared group B teeth. A 40-year-old male prepared group C teeth with nine years of experience as a general dental practitioner in a private hospital.
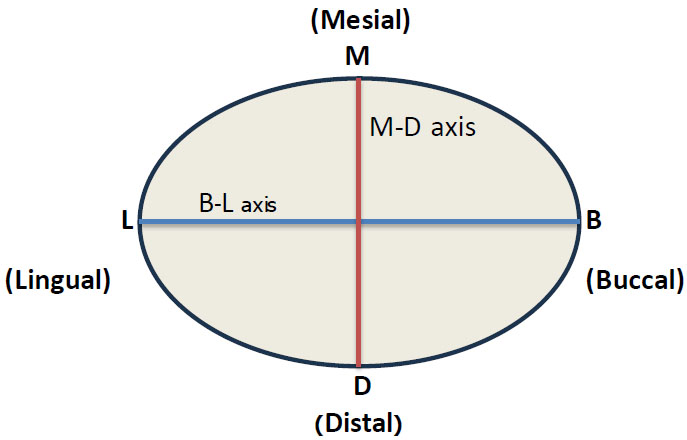
CBCT was used to examine the extent of dentin removal within the canal area (Kodak 9000C 3D, Atlanta, GA, USA). To guarantee excellent image quality, three scans were performed at different kilovoltage peaks (kVps) at a constant milliampere (mA). Three scans were performed at various mAs at the kVp with the optimal value after the best kVp was chosen. The optimal readings of 60 kVp and 15 mA were attained. There was a 44.2-second exposure period. Both before and after post-space preparation, we carried out analyses. The intracanal space was measured using CBCTs in axial sections at 3 mm, 5 mm, and 7 mm apically. A single image was captured at every level of the cross-section, which was then magnified to 100%. The photos were modified using three-dimensional dental imaging software (CS 3D Imaging Software, Carestream Dental, Atlanta, GA). The start point for all measurements was 3 mm above the bifurcated area. Subsequently, the calibration tool within the imaging software was used to calculate the mean values of the distances bucco-lingually (B-L axis) and mesio-distally (M-D axis) resulting from the measurements at 3, 5, and 7 mm. The B-L axis was represented by the line connecting the M-D axis line perpendicular to each other within the canal lumen. (Figs. 2 and 3). To calculate the canal area, the following equation was used:
 |
Mesiodistal periapical radiographs were collected following post-space preparation in order to detect any potential problems.
2.1. Statistical Analysis
A paired sample t-test was used to examine the drills' effects. P-values <0.05 were considered statistically significant. ANOVA analysis was used to compare the mean of intra-canal area among all groups. We determined the normality of the data distribution using Kolmogorov-Smirnov and Shapiro-Wilk test. We checked the normality of the three groups before and after the drilling.
An Independent sample t-test was used to determine the significant difference between the two types of drills. We used a paired-sample t-test to determine the effects of the type of drill used (preoperatively and postoperatively) on intracanal dentin removal.
3. RESULTS
Three dental practitioners handled a total of 72 bifurcated premolars with different experiences in dental treatment. After checking the normality of the three groups, it was obvious that the normality condition was satisfied since the significance value was greater than 0.05, as shown in Table 1.
| Tests of Normality | |||||||
|---|---|---|---|---|---|---|---|
| - | Drill Type | Kolmogorov-Smirnova | Shapiro-Wilk | ||||
| Groups | Statistic | df | Sig. | Statistic | df | Sig. | |
| Preoperative A | Peeso | 0.132 | 12 | 0.200* | 0.961 | 12 | 0.802 |
| Para | 0.195 | 12 | 0.200* | 0.922 | 12 | 0.299 | |
| Postoperative A | Peeso | 0.156 | 12 | 0.200* | 0.967 | 12 | 0.874 |
| Para | 0.135 | 12 | 0.200* | 0.916 | 12 | 0.254 | |
| Preoperative B | Peeso | 0.137 | 12 | 0.200* | 0.985 | 12 | 0.996 |
| Para | 0.157 | 12 | 0.200* | 0.956 | 12 | 0.720 | |
| Postoperative B | Peeso | 0.187 | 12 | 0.200* | 0.946 | 12 | 0.576 |
| Para | 0.150 | 12 | 0.200* | 0.954 | 12 | 0.701 | |
| Preoperative C | Peeso | 0.200 | 12 | 0.200* | 0.961 | 12 | 0.793 |
| Para | 0.136 | 12 | 0.200* | 0.962 | 12 | 0.811 | |
| Postoperative C | Peeso | 0.132 | 12 | 0.200* | 0.977 | 12 | 0.969 |
| Para | 0.097 | 12 | 0.200* | 0.990 | 12 | 1.000 | |
| Drill Type | Period | Mean Canal Area (mm2) | SD (mm) | |
|---|---|---|---|---|
| Group A | Peeso | Before | 0.61 | 0.044 |
| After | 0.82 | 0.032 | ||
| Para | Before | 0.62 | 0.043 | |
| After | 0.78 | 0.049 | ||
| Group B | Peeso | Before | 0.58 | 0.043 |
| After | 0.81 | 0.042 | ||
| Para | Before | 0.62 | 0.046 | |
| After | 0.79 | 0.042 | ||
| Group C | Peeso | Before | 0.62 | 0.051 |
| After | 0.82 | 0.034 | ||
| Para | Before | 0.60 | 0.047 | |
| After | 0.79 | 0.035 | ||
| Drill Type | Period | Mean Canal Area (mm) | Mean Difference | P-value |
|---|---|---|---|---|
| Peeso Reamer | Before | 0.673 | 0.012 | 0.71 |
| ParaPost | 0.669 | |||
| Peeso Reamer | After | 0.749 | 0.009 | 0.16 |
| ParaPost | 0.736 |
We used the mean and standard deviation as descriptive measures for the intracanal area, as shown in Table 2 and Fig. (4).
P<0.05 was considered significant. The mean intracanal area among the study groups was compared using ANOVA analysis.
Table 3 shows no significant difference in the mean of the intracanal area between the Peeso Reamer #2 and the ParaPost #1 (p=0.16).
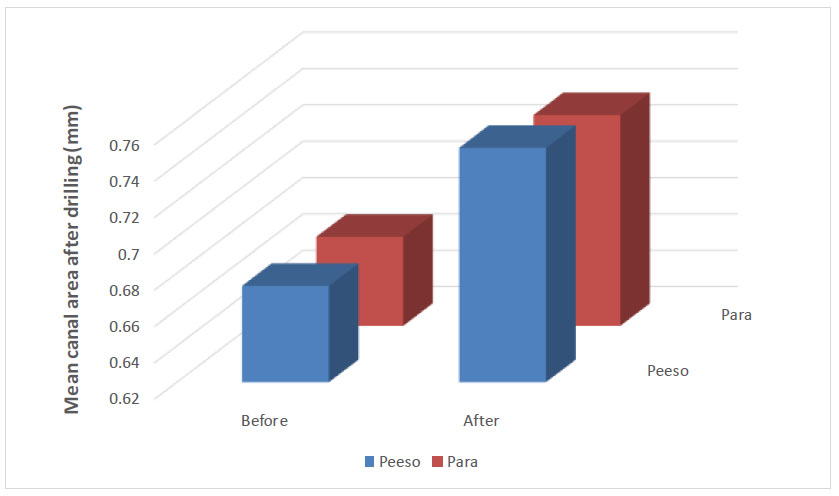
The mean intracanal area when using the Peeso Reamer #2 (0.749 mm) was a little higher than when using the ParaPost #1 (0.736mm). There was no significant difference in the intracanal area before using the Peeso Reamer and ParaPost drill (p=0.71), and using the Peeso Reamer drill resulted in a little more dentin removal in the canal lumen compared to using the ParaPost drill (Fig. 5).
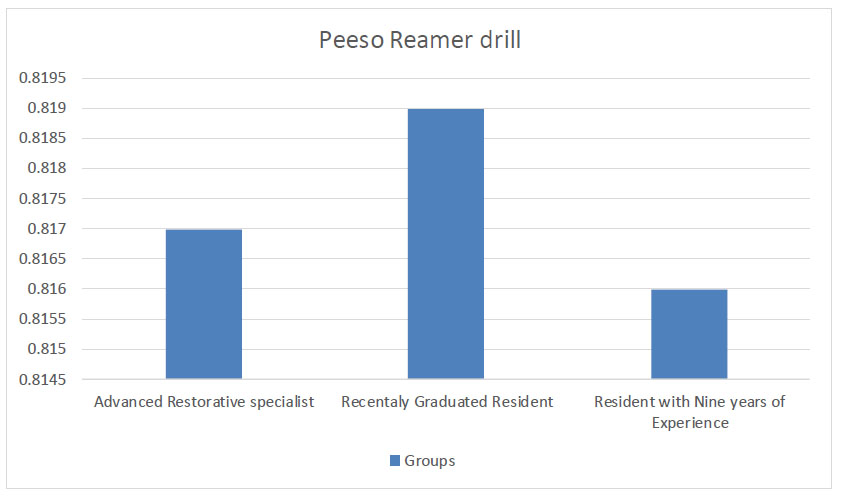
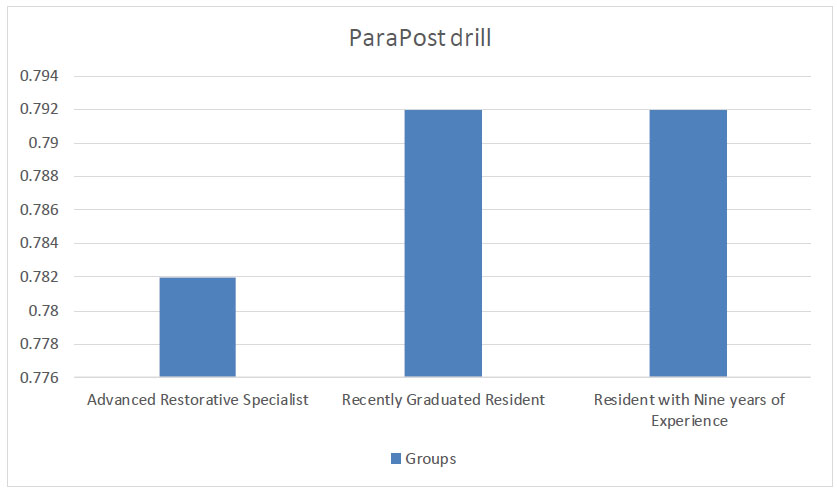
The advanced restorative specialist who prepared the teeth in group A achieved a significantly smaller mean intracanal area postoperatively than preoperatively with both types of drill (p<0.05; Table 4). The recently graduated resident who prepared the teeth in group B achieved a significantly larger mean intracanal area postoperatively than preoperatively with both types of drill (p<0.05; Table 5). The resident with nine years of experience who prepared the teeth in group C achieved a total significantly larger mean intracanal area postopera- tively with both the ParaPost and the Peeso drill with preoperative thicknesses (p<0.05; Table 6).
| Drill Type | Period | Mean Canal Area (mm2) | Mean Canal Area Difference | SD (mm) | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Peeso (before-after) | Before | 0.6125 | -0.20500 | 0.0550 | (-0.2310, -0.1700) | p≤.05 |
| After | 0.8175 | |||||
| ParaPost (before-after) | Before | 0.6250 | -0.15750 | 0.0614 | (-0.1965, -0.1185) | p≤.05 |
| After | 0.7825 |
| Drill Type | Period | Mean Canal Area (mm2) | Mean Canal Area Difference | SD (mm) | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Peeso (before-after) | Before | 0.5850 | -0.23417 | 0.0558 | (-0.2696, -0 .1987) | p≤.05 |
| After | 0.8192 | |||||
| Para (before-after) | Before | 0.6192 | -0.17250 | 0.0465 | (-0.2021, -0.1429) | p≤.05 |
| After | 0.7917 |
| Drill Type | Period | Mean Canal Area (mm2) | Mean Canal Area Difference | SD (mm) | 95% CI | P-value |
|---|---|---|---|---|---|---|
| Peeso | Before | 0.6167 | -0.1992 | 0.0569 | (-0.2354, -0.1629) | p≤.05 |
| After | 0.8158 | |||||
| Para | Before | 0.6042 | -0.1875 | 0.0379 | (-0.2116, -0.1634) | p≤.05 |
| After | 0.7917 |
| Drill Type | Period | Mean Canal Area (mm2) | Mean Difference | 95% CI | P-value |
|---|---|---|---|---|---|
| Peeso Reamer | Before | 0.67 | -0.85 | (-0.147, -0.005) |

|
| After | 0.75 | ||||
| ParaPost | Before | 0.67 | -0.72 | (-0.124, -0.010) |

|
| After | 0.74 |
| Group | Peeso Reamer | ParaPost | ||||
|---|---|---|---|---|---|---|
| Mean canal area (mm2) | F-test | P-value | Mean Canal Area (mm2) | F-test | P-value | |
| A) Advanced restorative specialist | 0.817 | 9.967 |

|
0. 782 | 8.963 |

|
| B) Recently graduated resident | 0.819 | - | - | 0.792 | - | - |
| C) Resident with nine years of experience | 0.816 | - | - | 0.792 | - | - |
It can be concluded from Tables 4-6 that the difference in the standard deviation is small, which indicates the standard deviation to be statistically very similar before and after the drilling.
We found a significant increase in the mean canal area after the operation than before when using the Peeso Reamer (p≤0.036) and ParaPost drill (p≤0.022) (Table 7).
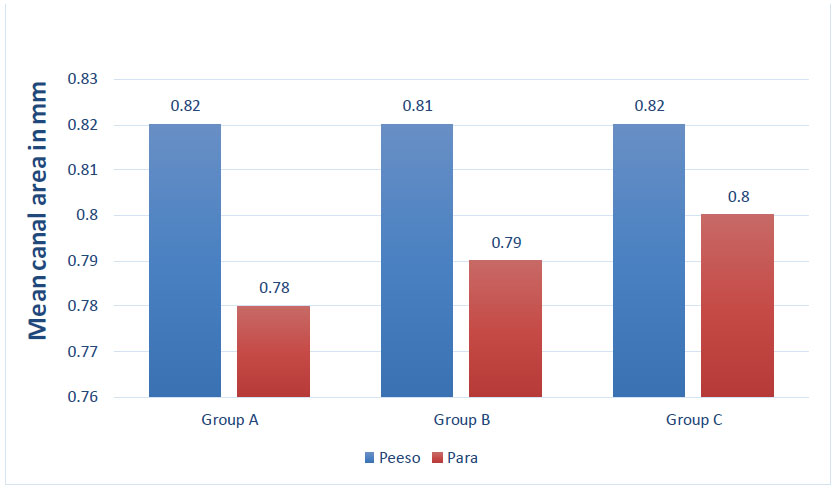
The changes in the mean canal area between groups A, B, and C were significant for the Preeso Reamer #2 (p=0.003) and ParaPost #1 drill (p=0.006) (Table 8, Figs. (6 and 7).
The correlation between drill type and complication has been obtained as a positive and moderate correlation, showing the drill type to affect the deviation, as illustrated in Table 9.
| Model | R | R-square | Adjusted R square | Std. Error of the Estimate |
|---|---|---|---|---|
| 1 |

|
0.427 | 0.419 | 1.469 |
| - | Complication | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| None | Minute Deviation from the Canal Center | Slight Deviation from the Canal Center | Moderate Deviation from the Canal Center | Total Deviation from the Canal Center | Furcal Perforation | - | ||
| Drill type | Peeso | 29 | 2 | 5 | 0 | 0 | 0 | 36 |

|
5.6% | 13.9% | 0.0% | 0.0% | 0.0% | 100.0% | ||
| Para | 10 | 0 | 2 | 6 | 10 | 8 | 36 | |

|
0.0% | 5.6% | 16.7% | 27.8% | 22.2% | 100.0% | ||
| Total | 39 | 2 | 7 | 6 | 10 | 8 | 72 | |
| 54.2% | 2.8% | 9.7% | 8.3% | 13.9% | 11.1% | 100.0% | ||
The deviation from the center of the canal was classified into four categories, namely minute deviation, slight deviation, moderate deviation, and total deviation. We considered it minute if one-fourth of the post space shifted laterally from the center of the canal pathway. If two-fourths shifted, it was taken as a slight deviation. If three-quarters of the post space has shifted, it was observed to be a moderate deviation. Lastly, total deviation meant that the whole post space was away from the canal center pathway. It was considered important to test the association between the drill type and the complications for all groups using crosstabs, as shown in Table 10.
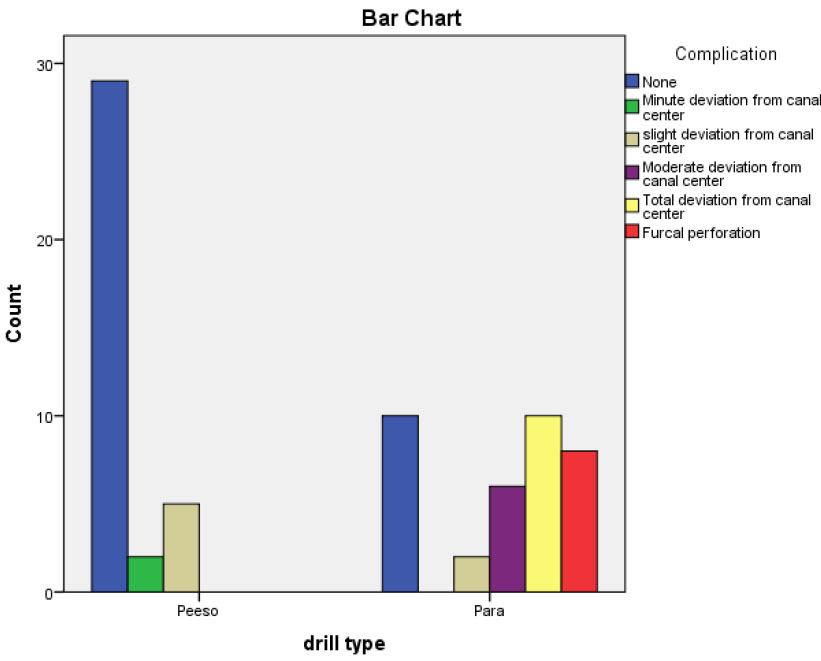
From Table 10, it can be concluded that the Peeso Reamer #2 proved to be better than the ParaPost #1 in drilling since using Peeso Reamer prevented 80% deviation, but using the ParaPost prevented only 27.8% deviation. The types of drilling versus the type of deviation are illustrated in Fig. (8).
The chi-square value of 0.000 less than 0.05 shows that the relationship between the drill type and deviation was statistically significant (Table 11).
Twenty-one teeth showed various degrees of deviation from the center of the canal, and the ParaPost drill caused eight furcal perforations. The Peeso Reamer drill resulted in only seven teeth with minimal deviation from the center of the canal during the preparation (Tables 12-14, and Fig. 9).
Using the Pesso Reamer drill resulted in a little more dentin removal in the canal area during the post-space preparation than using the ParaPost drill. However, the Peeso Reamer had fewer complications because it followed the canal configuration. The ParaPost was associated with a higher risk of causing deviation or perforation than the Peeso Reamer drill (Fig. 9).
| - | Value | Df | Asymp. sig. (2-sided) |
|---|---|---|---|
| Pearson Chi-square | 36.542 | 5 |

|
| Likelihood ratio | 47.034 | 5 | 0.000 |
| Linear-by-linear association | 30.313 | 1 | 0.000 |
| N of valid cases | 72 | - | - |
| Tooth Number and Drill Type | Mean Canal Area (mm2) | Complications (Perforations or Deviation) | |
|---|---|---|---|
| Preoperative | Postoperative | ||
| Peeso Reamer 1 | 0.63 | 0.81 | None |
| Peeso Reamer 2 | 0.61 | 0.84 | None |
| Peeso Reamer 3 | 0.65 | 0.80 | None |
| Peeso Reamer 4 | 0.59 | 0.78 | None |
| Peeso Reamer 5 | 0.64 | 0.85 | None |
| Peeso Reamer 6 | 0.59 | 0.77 | None |
| Peeso Reamer 7 | 0.66 | 0.83 | Minute deviation from the canal center |
| Peeso Reamer 8 | 0.54 | 0.81 | None |
| Peeso Reamer 9 | 0.58 | 0.87 | None |
| Peeso Reamer 10 | 0.55 | 0.82 | None |
| Peeso Reamer 11 | 0.63 | 0.85 | Slight deviation from the canal center |
| Peeso Reamer 12 | 0.68 | 0.78 | None |
| ParaPost 1 | 0.59 | 0.79 | None |
| ParaPost 2 | 0.67 | 0.82 | Total deviation from the canal center |
| ParaPost 3 | 0.60 | 0.84 | Total deviation from the canal center |
| ParaPost 4 | 0.59 | 0.77 | Slight deviation from the canal center |
| ParaPost 5 | 0.57 | 0.78 | Total deviation from the canal center |
| ParaPost 6 | 0.61 | 0.72 | None |
| ParaPost 7 | 0.68 | 0.85 | Moderate deviation from the canal center |
| ParaPost 8 | 0.64 | 0.82 | None |
| ParaPost 9 | 0.68 | 0.72 | Moderate deviation from the canal center |
| ParaPost 10 | 0.66 | 0.71 | Total deviation from the canal center |
| ParaPost 11 | 0.56 | 0.75 | None |
| ParaPost 12 | 0.65 | 0.82 | Total deviation from the canal center |
| Tooth Number and Drill Type | Mean Canal Area (mm2) | Complications (Perforations or Deviation) | |
|---|---|---|---|
| Preoperative | Postoperative | ||
| Peeso Reamer 1 | 0.60 | 0.85 | None |
| Peeso Reamer 2 | 0.58 | 0.75 | None |
| Peeso Reamer 3 | 0.57 | 0.85 | Slight deviation from the canal center |
| Peeso Reamer 4 | 0.60 | 0.82 | None |
| Peeso Reamer 5 | 0.51 | 0.83 | None |
| Peeso Reamer 6 | 0.54 | 0.85 | None |
| Peeso Reamer 7 | 0.63 | 0.79 | None |
| Peeso Reamer 8 | 0.55 | 0.76 | Slight deviation from the canal center |
| Peeso Reamer 9 | 0.55 | 0.78 | None |
| Peeso Reamer 10 | 0.61 | 0.88 | None |
| Peeso Reamer 11 | 0.66 | 0.81 | Minute deviation from the canal center |
| Peeso Reamer 12 | 0.62 | 0.86 | None |
| ParaPost 1 | 0.55 | 0.72 | Furcal perforation |
| ParaPost 2 | 0.63 | 0.73 | Total deviation from the canal center |
| ParaPost 3 | 0.70 | 0.82 | Furcal perforation |
| ParaPost 4 | 0.62 | 0.81 | Moderate deviation from the canal center |
| ParaPost 5 | 0.60 | 0.85 | None |
| ParaPost 6 | 0.59 | 0.78 | Furcal perforation |
| ParaPost 7 | 0.63 | 0.81 | Total deviation from the canal center |
| ParaPost 8 | 0.56 | 0.79 | Moderate deviation from the canal center |
| ParaPost 9 | 0.65 | 0.76 | Furcal perforation |
| ParaPost 10 | 0.62 | 0.79 | Total deviation from the canal center |
| ParaPost 11 | 0.59 | 0.80 | Furcal perforation |
| ParaPost 12 | 0.69 | 0.84 | Total deviation from the canal center |
| Tooth Number and Drill Type | Mean Canal Area (mm2) | Complications (Perforations or Deviation) | |
|---|---|---|---|
| Preoperative | Postoperative | ||
| Peeso Reamer 1 | 0.59 | 0.83 | None |
| Peeso Reamer 2 | 0.63 | 0.82 | Slight deviation from the canal center |
| Peeso Reamer 3 | 0.56 | 0.79 | None |
| Peeso Reamer 4 | 0.67 | 0.81 | None |
| Peeso Reamer 5 | 0.64 | 0.88 | None |
| Peeso Reamer 6 | 0.59 | 0.76 | None |
| Peeso Reamer 7 | 0.66 | 0.84 | None |
| Peeso Reamer 8 | 0.58 | 0.85 | None |
| Peeso Reamer 9 | 0.53 | 0.83 | None |
| Peeso Reamer 10 | 0.66 | 0.79 | None |
| Peeso Reamer 11 | 0.59 | 0.77 | Slight deviation from the canal center |
| Peeso Reamer 12 | 0.70 | 0.82 | None |
| ParaPost 1 | 0.61 | 0.80 | Furcal perforation |
| ParaPost 2 | 0.59 | 0.73 | Total deviation from the canal center |
| ParaPost 3 | 0.69 | 0.82 | Total deviation from the canal center |
| ParaPost 4 | 0.63 | 0.85 | Slight deviation from the canal center |
| ParaPost 5 | 0.64 | 0.81 | Moderate deviation from the canal center |
| ParaPost 6 | 0.56 | 0.76 | None |
| ParaPost 7 | 0.62 | 0.80 | Moderate deviation from the canal center |
| ParaPost 8 | 0.57 | 0.79 | Furcal perforation |
| ParaPost 9 | 0.61 | 0.83 | None |
| ParaPost 10 | 0.54 | 0.78 | Total deviation from the canal center |
| ParaPost 11 | 0.64 | 0.77 | Furcal perforation |
| ParaPost 12 | 0.55 | 0.76 | Total deviation from the canal center |
4. DISCUSSION
The primary aim of this study was to develop a better understanding of how the selection of an appropriate drill for post-space use in bifurcated premolars is essential for successful patient outcomes. By preserving the intracanal dentin, we can maintain the integrity of the tooth structure and reduce the potential for further damage. Consequently, a crucial component of teeth's fracture resistance is dentin thickness. Premolars have a narrow canal and variable post-space configurations, making strip perforation during post-space preparation extremely risky [13]. The tooth wall's thickness directly correlates with a tooth's ability to tolerate lateral forces [14]. Trope et al. found that creating an access opening without a post space was more effective in strengthening endodontically treated teeth than creating a post space [15].
As a result of these factors, certain researchers have given a high priority to maintaining dentin, while others have shown that post-preparations need at least 1 mm of residual thickness [16]. A tooth may become weaker and develop root fractures as a result of an excessive or improper dentin removal procedure if the original canal is not followed [17]. Five drills were compared by Fisher et al. utilizing artificial roots rather than teeth that were taken from humans. They discovered that the ParaPost and Parkell's C-I drills (a system for amalgam and composite cores) exhibited the highest degree of deviation from the canal center, while the Peeso Reamer and Kurer drills demonstrated the least [18]. This is similar to our findings, as more deviations in our study occurred in canals prepared using the ParaPost drill. With the exception of Peeso Reamer and Kurer drills, Fisher et al. similarly observed a noticeably higher variation in preparation dimensions in the faciolingual surface compared to the mesiodistal directions [18].
Pilo and colleagues reported that using parallel-sided drills, like ParaPost, during post-space preparations endangers root integrity due to the risks involved during preparation [12], and our research has confirmed their findings.
Our method involved post-space preparation for all groups under standardized conditions to get more reliable results and then using CBCT imaging to measure the dentine thickness canal area without destroying the teeth by sectioning. This approach guaranteed no loss of intracanal dentin during the cutting of teeth, providing more accurate results, unlike the Muffle technique, which has certain drawbacks, including its invasive nature and its requirement of physically reassembling sections. In addition, it involves destructive sectioning of specimens, which is another limitation to consider [16, 19].
Hartmann et al. demonstrated the reliability of this method without the need for destructive sectioning of the specimens in their research [20]. Meanwhile, Ozgur Uyanik and his team found CT scans to enable simple measurement of canal changes and that they can reduce the risk of radiographic or photographic transfer errors [21].
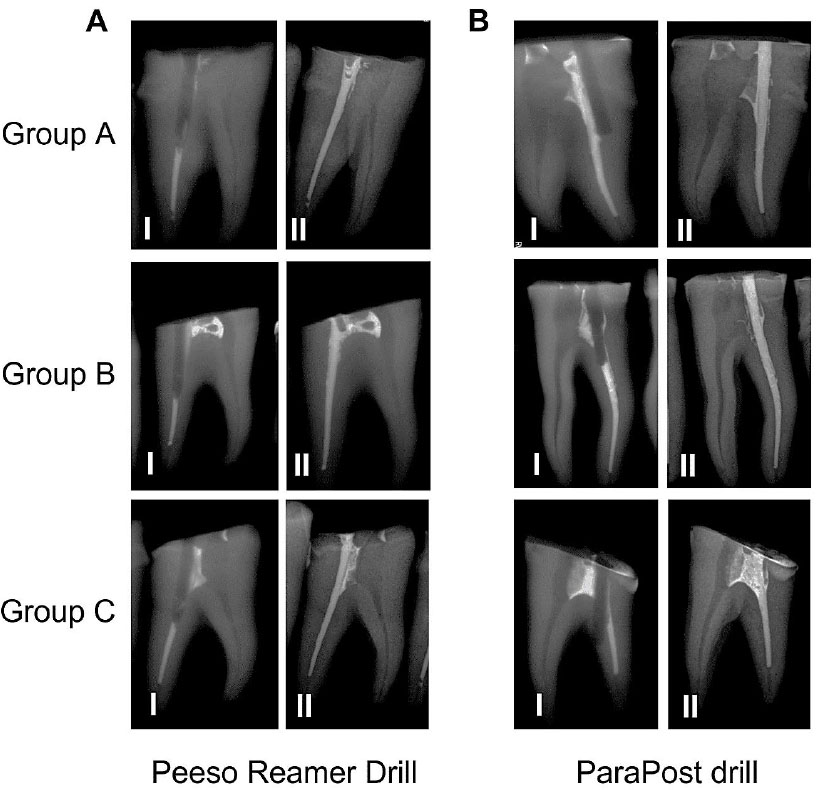
The risk of root perforation increases when the drill is moved farther from the middle of a canal that has been properly endodontically treated. The radiograph presented in Fig. (9) illustrates how much more easily deviations can be noticed using the mesiodistal view than with the buccolingual view. It is crucial to understand the diameter and deviation linked to a specific drill type. Post-space preparation appears to depend on the root configuration, the operator, and the design of the cutting side of an instrument. Our experiment has demonstrated the operator’s experience to be a significant factor, as evidenced by the results of group A, which had fewer complications compared to the other groups.
There are some limitations associated with our study as there is a lack of prior research studies on the same comparison of post-drills. Therefore, to provide stronger evidence for our findings, we need further studies that are similar in nature.
CONCLUSION
Within the limitations of our study, the Pesso Reamer drill caused a little more dentin removal than the ParaPost drill. However, the Peeso Reamer had fewer risks and was safer to use than the ParaPost drill in bifurcated premolars. Given their narrow canals and significant deviation and perforation risk, bifurcated premolars are not advised to be drilled using a ParaPost drill.
LIST OF ABBREVIATIONS
| CBCT | = Cone-beam Computed Tomography |
| kVps | = kilovoltage peaks |
| mA | = milliampere |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study received ethical approval with the number KACST, KSA: H-01-R069.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.

