All published articles of this journal are available on ScienceDirect.

A Clinical Appearance of Traumatic Fibroma with a Distinct and Rare Histological Diagnosis –insights of Pseudo Perineurioma – Case Report
Authors Info & Affiliations
Abstract
Background
Oral pseudo perineurioma is a reactive lesion of the peripheral nerve sheath rarely described in the literature, occurring more frequently in the tongue and lower lips.
Objective
The objective of this case report is to describe pseudoperineurioma with a literary basis, to encourage learning and assist in decision-making in certain situations.
Case Report
We present here a rare case of oral pseudoperineurioma in tongue that occurred in a 19-year-old man and a brief review of the literature. A 19-year-old man presented with a nodular lesion on the dorsum of the tongue without painful symptoms. Excisional biopsy was performed. The pathological examination revealed a proliferation of structures like onion bulbs. Immunohistochemical analysis was positive for GLUT-1.
Conclusion
The histological diagnosis was oral pseudoperineurioma. Oral pseudoperineurioma is a rare clinical lesion and can be confused with other reactive and neoplastic conditions of the oral cavity.
1. INTRODUCTION
Perineural cells were first studied and described in 1873 as cells lining the nerve, literally “delicate perineural skin” [1]. Previous studies had reported that perineural cells are derived from fibroblasts stimulated by Desert Hedgehog, an intercellular signaling molecule secreted by Schwann cells, which leads perineural fibroblasts to form a cell sheath, the perineural barrier [2, 3]. The typical morphological and immunohistochemical characteristics of the perineural cells in the lesions contribute to the diagnosis of traumatic neuromas, peripheral nerve sheath tumors, and benign mixed nerve sheath tumors [4].
Perineuriomium is a benign neoplasm of the peripheral nerve sheath with perineural origin. However, peri- neurium can be presented mainly in intraneural and extraneural perineuriomas [5]. The morphological characteristics of the perineurioma are distinct, that is, it is composed of concentric layers of perineural cells [6]. The concentric layers of cells resemble the onion bulb appearance in Schwann cell lesions. However, Schwann cells arise from the endoneurial layers, and the perineurioma arises from the perineural layer [5, 7].
Although the histological and immunohistochemical characteristics of perineurioma are well established in the literature, in recent decades, scholars have discussed the existence of an intraneural pseudo perineuriomatous proliferation or pseudo perineurioma. This lesion has morphological characteristics like intraneural perineurioma and is often misdiagnosed. Pseudo perineurioma presents clinicopathological features of reactive lesions of the oral peripheral nerve sheath. This result may be due to traumatic and non-open mechanical injury, i.e., chronic and ischemic nerve compression or focal loss of the perineural lining without nerve transection [3].
Previous studies had reported case of intraneural perineurioma in the oral mucosa [6, 8, 9]. However, histological features such as spacing and distinct collagenous hyperplasia between individual pseudo-onion bulbs, lack or interruption of perineural involvement of the hyperplastic nerve fascicle [6, 8, 9] the morphological features of intraneural pseudo perineuriomatous proli- feration are similar.
Thus, the histological differentiation between pseudo perineuriomium and other perineural lesions in the oral mucosa can be difficult to diagnose for the oral pathologist. Thus, the present study aims to report a case of oral pseudo neurioma in the tongue and review the literature regarding clinical presentation and histo- pathology.
2. CASE REPORT
A 19-year-old man attended a particular office (CK Estomatologia) at Guarulhos, São Paulo, Brazil, presenting a slow, progressive, asymptomatic growth lesion. This lesion had been present for 2 years and clinically appeared as a pedicled nodule, located on the right lateral dorsum of the tongue, 2.5 cm in diameter and pink surface, close to the color of the surrounding mucosa (Fig. 1). The initial diagnosis was inflammatory fibrous hyperplasia, and a tissue fragment was referred to histological analysis. This excisional biopsy was also the treatment; We followed up the patient in the first month without any recurrence (Fig. 1) and after around 2 years of following up no recurrence was observed.

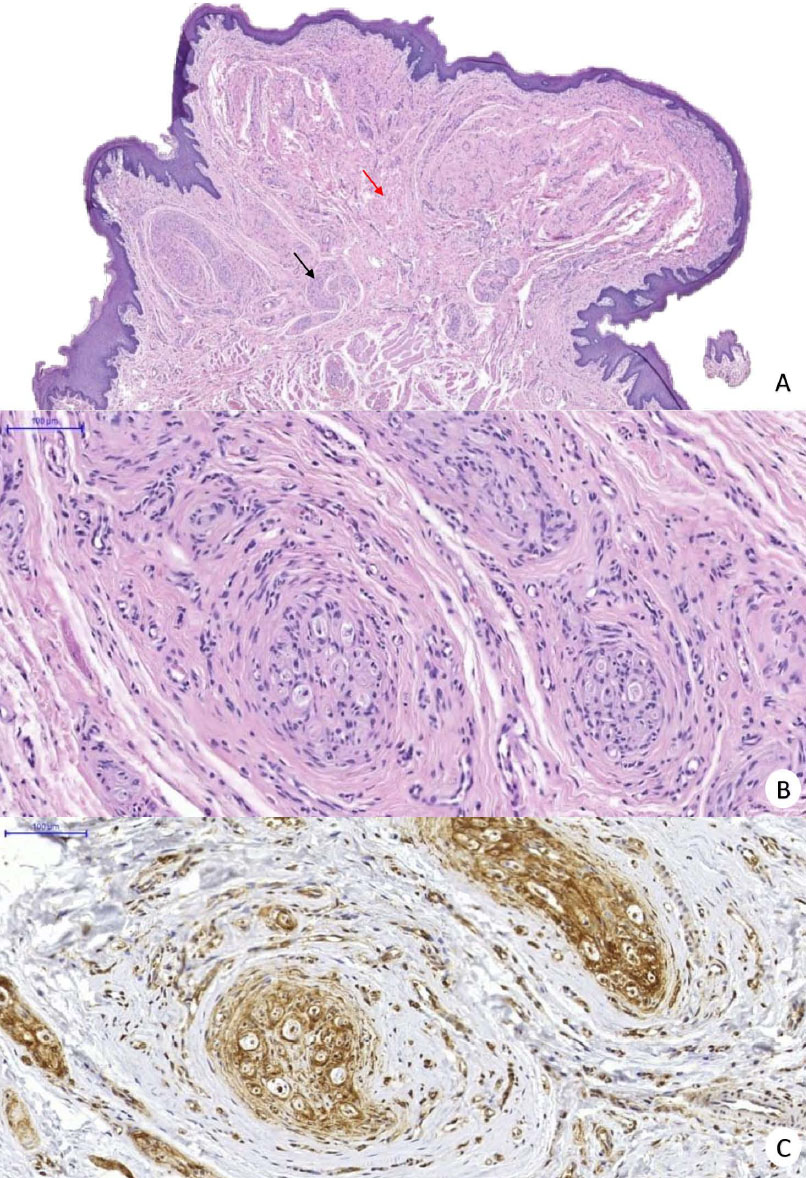
Histologically fragments of mucosa containing proliferative lesions on the lamina propria were revealed. This wascomposed of highly collagenated connective tissue, of which numerous nerve bundles were observed, sometimes cut transversely, sometimes longitudinally, and by nerve structures containing so-called onion pseudo-bulbs. These were characterized by flattened cells that werearranged concentrically around an axon. The lesion is covered by parakeratinized atrophic stratified squamous epithelium with a rectified basal layer. In the subepithelial connective tissue, there wasa discrete chronic inflammatory infiltrate, bundles of skeletal striated muscle fibers with an aspect of normality at the base of the lesion (Fig. 2).
Immunohistochemical staining was performed using antibodies against S100 (clone S100, dilution 1:10.000, Dako), GLUT-1 (polyclonal, dilution 1:100, BioSystems SPRING), and Epithelial membrane antigen (EMA) (clone E29, dilution 1:50, Dako).
S100 was positive on Schwann cells. EMA showed the absence of perineurioma around the nerve, and GLUT-1 showed onion pseudobulbs, which showed that the perineural envelope of the affected nerve was incomplete (Fig. 2).
3. RESULT & DISCUSSION
The term intraneural pseudo perineuriomatous proliferation was first described in 2013 by Koutlas & Scheithauer, who described it as an apparently reactive lesion of the oral peripheral nerve sheath. In the study, Koutlas & Scheithauer, observed that all lesions were nodular or polypoid that mainly affect the tongue, corroborating our case. Thus, clinically, oral pseudo perineurioma may resemble traumatic fibroma. In addition, the frequent involvement of oral pseudo perineurioma in areas susceptible to trauma, such as the tongue and lower lips, supports the hypothesis of a traumatic etiology [3].
The diagnosis must be based on the histological features of the oral pseudoperineurioma, such as a pattern that varies from round or ovoid to plexiform pseudo-onion bulb nests. There are cases that may present fibrous stromal hyperplasia interspersed with pseudo-onion bulbs. A serpiginous pattern can also be observed [3]. However, the oral pathologist needs attention to close the diagnosis of oral pseudo perineuriomium, as there are other neural lesions that present similar morphological characteristics.
In the present case, the diagnostic hypothesis was inflammatory fibrous hyperplasia. Certainly, there is no clinical characteristic that led us to think of a nerve-derived lesion. We do not think of oral pseudo perineurioma by the rarity of the case. It is important to emphasize that diagnostic confusion may occur in the evaluation of histopathological examination with traumatic neuromas.
Possibly, these similar morphological findings in some neural lesions can be explained by the loss of the perineurial barrier due to previous trauma, causing endoneurial fibroblasts to transform into perineural cells due to the stimulatory effect of Desert Hedgehog by Schwann cells that sheath axons [2], resulting in a newly formed protective barrier around individual Schwann cell-axon nerve units [10, 11]. The deposition of collagen between the cell layers that the pseudobulbs cells results from secretion by perineural cells, resulting in fascicular enlargement without obvious loss of axons [3].
On the other hand, a study carried out by Chou in 1992, which classified the types of hypertrophic neuropathies that present cells morphologically like onion bulbs, observed that there are two types, those with central Schwann cells (paratraumatic perineurioma and, in some cases, amputation neuroma) and those with no or few Schwann cells (hamartomas). Thus, it may be that there are two different etiologies for the proliferation of intraneural onion bulbs, one neoplastic and the other reactive [3].
In 2013, Koutlas & Scheithauer, pioneers in the study of oral pseudo perineuriomium, suggested some histological features to distinguish oral pseudo peri- neuriomium from true intraneural perineuriomium, \including: (a) it may present perineural discontinuity of the affected minor nerve, (b) the layers of perineural cells in the onion pseudobulbs rarely present more than one, (c) the intrafascicular collagenous component is present, and (c) generally comprises part of another lesion, i.e., fibrous hyperplasia/fibroma. While true intraneural perineurioma has more than one perineural cell layer in the onion bulb, the affected nerve sheath is normally intact, and the collagenous component is limited to prominent (sclerosis), and only the main lesion is seen.
CONCLUSION
In conclusion, oral pseudo perineuriomium is a rare lesion in the oral cavity, and there are few studies in the literature on it. Clinical features can be confused with other reactive or neoplastic lesions; however, it is very difficult to propose other hypotheses that do not cover non-neoplastic proliferative processes or benign tumors, and the final diagnosis can be confirmed with detailed analysis of morphological features and immunohisto- chemical analysis. Finally, we emphasize that the correct diagnosis is only possible with the morphological analysis of the lesion.
AUTHORS' CONTRIBUTION
Ana Clara Ribeiro Carnevalli, Sara Maria Santos Dias da Silva, and Larissa Sandy da Silva Leite contributed in writing the text, Vitória Tavares de Moura revised the text; Dárcio Kitakawa and Felipe da Silva Peralta did clinical care and constributed as responsible surgeons, Thayná Melo de Lima Morais contributed as a responsible oral pathologist and co-supervisor and Luis Felipe das Chagas e Silva de Carvalho assisted clinically and contributed as anadvisor).
ABBREVIATION
| EMA | = Epithelial Membrane Antigen |
CONSENT FOR PUBLICATION
The patient authorized the clinical case to be published for teaching purposes. Consent for publication was obtained for every individual person’s data included in the study.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.

