All published articles of this journal are available on ScienceDirect.

Parental Acceptance of Behavior Management Techniques for Pediatric Dental Visits in Qassim, Saudi Arabia: A Cross-sectional Study
Authors Info & Affiliations
Abstract
Background:
Behaviour management techniques have been commonly used to promote a child’s positive behaviour during oral health treatment. Parents play an important role in their child’s dental care and its delivery.
Objective:
This study aimed to determine the most accepted behaviour management techniques used in paediatric dental clinics and assess the parents’ acceptance level for each technique using a visual analogue scale.
Methods:
This cross-sectional study based in Qassim, Saudi Arabia, used videotaped scenes of seven behaviour management techniques recorded in Arabic. After watching the videos, parents filled out a questionnaire on acceptance of each technique and rated their acceptance of it by using a visual analogue scale.
Results:
The study consisted of 130 parents, of which 86 (66.2%) were males and 44 (33.8%) were females. 96.9% of parents approved positive reinforcement, which was followed by tell-show-do (TSD) with 93.1% acceptance. General anesthesia (47.7%) was the least accepted behavioral management technique.
Conclusion:
It is crucial for parents to systematically understand the procedures to be used in a pediatric dental setting. Dentist-parent communication is necessary to address any concerns, thereby creating a safe environment to deliver quality oral care.
1. INTRODUCTION
One of the most challenging concerns in pediatric dentistry is dealing with uncooperative and anxious children during treatment. Successful treatment of children’s dental needs involves the management of their behaviour throughout dental procedures. Comprehensive application of behaviour manage-ment techniques (BMTs) is an integral part of paediatric dentalcare. These procedures aim to set up communication between the parent, patient, and the dentist to mitigate the fear and anxiety, and ease the delivery of quality dental care by promoting the child’s positive attitude towards oral health care [1]. The process by which the dental health team successfully and efficiently manages the child patients, while also developing a favorable dental attitude, is referred to as behavior management [2].
Several pharmacological and non-pharmacological behavioral management strategies have been applied in dental care contexts to provide dental services in a safe and effective manner [3, 4]. Tell-show-do, protective stabilization, voice control, parental separation, and positive reinforcement are common non-pharmacological approaches used, whereas nitrous oxide inhalation and general anaesthesia are common pharmacological techniques used [5]. A study conducted by Abushal and Adenubi [6] reported TSD, positive reinforcement, and voice control to be commonly used, while intravenous sedation, non-verbal communication, and physical restraint were rarely used BMTs reported in Saudi Arabia. Another cross-sectional study reported communicative techniques, such as TSD and positive reinforcement, to be the most routinely used by paediatric dentists [7].
The parent and the child should be included in the decision-making process when it pertains to BMT; dentists cannot decide on their own [8]. Parents play a crucial role in their child’s life, and acceptance of parents of these behaviour management techniques is critical to ensure that healthcare decisions are made in the best interest of the child, comply with legal and ethical considerations, foster collaboration and trust, and take into account individual factors for safe and effective care. It can help in making the dental experience less stressful and traumatic for the child, setting them on a trail toward good oral health and positive dental experiences during treatment in the future [9].
Childs’ dental care is greatly dependent on the parents’ knowledge and acceptance level of BMTs. It is because if parents are familiar with BMTs, they can understand and decide on better treatment for their child [10].
Parents' acceptance of behaviour management techniques can be influenced by a variety of factors, including cultural beliefs, personal beliefs and values, parenting style, prior experiences, education and knowledge, and the temperament and needs of their child [9, 11]. Previous research has identified TSD as the most widely accepted BMT [12, 13], whereas nitrous oxide and physical restrictions [13] have been found to be among the least accepted by parents [14]. Parents' acceptance is a crucial factor when selecting behavioural management approaches that are appropriate to their parenting philosophy and their child's personality traits. Therefore, the purpose of this study was to determine the most accepted BMTs used during pediatric dental and to assess the acceptance level of parents of each technique.
2. MATERIALS AND METHODS
2.1. Study Design, Setting and Ethical Consideration
This cross-sectional study was conducted at the Department of Orthodontics and Pediatric Dentistry, Qassim University, Saudi Arabia, among parents accompanying their children for dental treatment from October 2021 to May 2022. The study was carried out in accordance with the Declaration of Helsinki. The ethical approval for the conduct of this study was obtained from the Institutional Review Board of Qassim Research Centre (DRC), College of Dentistry, Qassim University (EA/ M-2020-3018). Furthermore, all individuals provided an informed consent. Parents were given an Arabic consent form as well as a participant information leaflet that explained the study's purpose, design, and procedures.
2.2. Participants and Eligibility Criteria
The parents of all 3 to 12-year-old children who visited the clinical setting over the study period participated in the study. Parents who had come for dental treatment in the ward for the first time were only included in the study. Parents with children who had previous negative dental experiences were excluded from the study. Parents with any disability that might interfere with their understanding of the presented videos, parents who reported to the clinic for an emergency dental treatment, and parents of medically compromised children were also excluded from the study.
2.3. Data collection and Measurement
A convenience non-probability sampling method was used to recruit the samples. A total of 130 parents accompanying their children to the dental clinic for treatment were selected. Videotaped scenes of seven behavior management techniques to be used during the actual pediatric dental treatment were viewed by the selected parents. The seven techniques shown were (1) tell-show-do (TSD), (2) nitrous oxide sedation (N2O), (3) protective stabilization, (4) voice control, (5) parental separation, (6) positivereinforcement, and (7) general anesthesia (GA). Most of the videotaped scene was made with Saudi child and adult actors to make it explicit and compatible with Saudi culture. The video clips were recorded in the Arabic language, with each technique being about 20-60 seconds long. Nitrous oxide sedation and general anaesthesia videos were downloaded from YouTube and superimposed with Arabic voiceover. After watching the videos, a questionnaire consisting of questions on acceptance of each technique with options yes and no was given to the parents to fill. Each question was written in both English and Arabic language to connect to every segment. Also, parents were asked to rate their acceptance of each technique by using a visual analogue scale (VAS) that was 10 mm long (horizontal line). The VAS is a simple, quick, and versatile tool that is widely used in research and clinical practice to assess subjective experiences and gather quantitative data on subjective perceptions [15]. The left and right anchor endpoints of the scale corresponded to the “completely unacceptable” and “completely acceptable” behaviour management techniques. To minimize the bias, researchers avoided framing questions that would lead participants to respond in a particular way. To avoid misinterpretation, questions were concise, clear, and written in simple language.
2.4. Study Size
The sample size was calculated using G power software. Based on the power of previously published articles, the lowest prevalence was taken to calculate the sample size. The observed prevalence of the protective stabilization technique (40%) and expected prevalence (60%) were considered for calculation. Keeping in mind the expected power of our study (0.80) and confidence interval of 95%, the sample size was calculated to be 119 participants with an effect size of 0.4082. However, the total sample was 130 parents to avoid any drop-out or bias.
2.5. Statistical Analysis
Microsoft Office Excel was used to prepare the master chart for the data obtained from the questionnaires. The data were further analysed by using Statistical Package for Social Sciences (IBM, SPSS Statistics, version 25, Chicago, Illinois, United States). The categorical data were summarised by using frequencies and percentages. The chi-square test of association was used to establish the relationship between gender and acceptance of behaviour management techniques. The chi-square test, followed by the Marascuilo procedure, was used to determine the significant difference between the proportion of acceptance of various behaviour management techniques. Visual analogue scale scores were subjected to the test of normality by using Kolmogorov-Smirnov test. VAS scores did not follow the normal distribution, and non-parametric statistical tests were used. VAS scores were described by using the minimum, maximum, median, and interquartile ranges (IQR). The VAS scores between the seven techniques were compared by using the Friedmann test, followed by post-hoc multiple comparison tests using Wilcoxon signed rank test with Bonferroni correction. Also, the Mann-Whitney U test was used to compare VAS scores for each technique between males and females. P<0.05 was considered statistically significant.
3. RESULTS
The study consisted of 130 parents who agreed to participate in the study. Among these, 86 (66.2%) were males and 44 (33.8%) were females. Table 1 displays the acceptance of parents of seven different behaviour management techniques to be used during the actual pediatric dental treatment procedure. The BMTs in Table 1 are arranged according to the rank of acceptance by parents.
The chi-square test of association performed (Table 3) between the seven BMTs and gender revealed TSD to have a significant association with gender (
The most approved BMTs by parents was positive reinforcement, with 96.9% approval, followed by TSD with 93.1% acceptance. While the least approved technique by parents was general anesthesia (47.7%). Voice control and protective stabilization had similar acceptance of 57.7% and 56.2%, respectively (Table 1). The comparison of proportions of responses by parents on acceptance showed a significant difference between the proportions with
| S. No. | Techniques | Responses | Total N (%) |
|---|---|---|---|
| 1. | Positive Reinforcement | Yes | 126 (96.9) |
| No | 4 (3.1) | ||
| 2. | Tell show do | Yes | 121 (93.1) |
| No | 9 (6.9) | ||
| 3. | Nitrous oxide | Yes | 98 (75.4) |
| No | 32 (24.6) | ||
| 4. | Voice Control | Yes | 75 (57.7) |
| No | 55 (42.3) | ||
| 5. | Protective Stabilization | Yes | 73 (56.2) |
| No | 57 (43.8) | ||
| 6. | Parental Separation | Yes | 70 (53.8) |
| No | 60 (46.20 | ||
| 7. | General Anaesthesia | Yes | 62 (47.7 |
| No | 68 (52.3) |
| S. No. | Multiple Pairwise Comparisons | Difference in Proportions | Critical Value | |
|---|---|---|---|---|
| 1 | Positive Reinforcement | Tell show do | 0.04 | 0.10 (NS) |
| Nitrous oxide | 0.22 | 0.14* | ||
| Voice control | 0.39 | 0.16* | ||
| Protective stabilization | 0.41 | 0.16* | ||
| Parental separation | 0.43 | 0.16* | ||
| General Anaesthesia | 0.49 | 0.16* | ||
| 2 | General Anaesthesia | Nitrous oxide | 0.18 | 0.16* |
| Voice control | 0.35 | 0.17* | ||
| Protective stabilization | 0.37 | 0.17* | ||
| Parental separation | 0.39 | 0.17* | ||
| General Anaesthesia | 0.45 | 0.17* | ||
| 3 | Nitrous oxide | Voice control | 0.18 | 0.20 (NS) |
| Protective stabilization | 0.19 | 0.20 (NS) | ||
| Parental separation | 0.22 | 0.21* | ||
| Voice control | 0.28 | 0.21* | ||
| 4 | Voice control | Protective stabilization | 0.02 | 0.22 (NS) |
| Parental separation | 0.04 | 0.22 (NS) | ||
| General Anaesthesia | 0.10 | 0.22 (NS) | ||
| 5 | Protective stabilization | Parental separation | 0.02 | 0.22 (NS) |
| General Anaesthesia | 0.08 | 0.22 (NS) | ||
| 6 | Parental separation | General Anaesthesia | 0.06 | 0.22 (NS) |
| S. No. | Techniques | VAS Score | ||
|---|---|---|---|---|
| Minimum | Maximum | Median (IQR) | ||
| 1 | Positive Reinforcement | 4 | 10 | 10(9-10) |
| 2 | Tell show do | 3 | 10 | 10(8-10) |
| 3 | Nitrous oxide | 0 | 10 | 8(6-10) |
| 4 | Protective Stabilization | 0 | 10 | 6(3-8)NS |
| 5 | Voice Control | 0 | 10 | 7(5-9) NS |
| 6 | Parental Separation | 0 | 10 | 6(4-8) NS |
| 7 | General Anaesthesia | 0 | 10 | 6(2.75-9) NS |
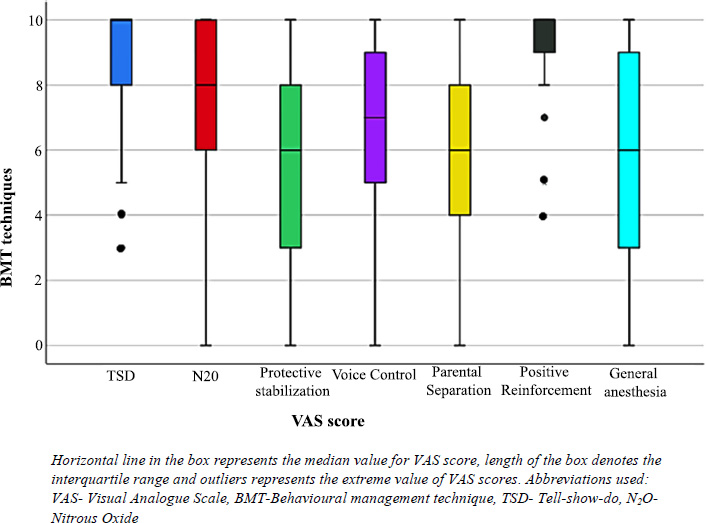
Using the Kolmogorov-Smirnov test of normality, the VAS scores were not found to be normally distributed; therefore, non-parametric tests were employed. Friedmann test was used to compare the median (IQR) VAS scores, which revealed a significant difference with chi-square (266.94, df=6, p=0.000<0.001). Hence, Wilcoxon's signed rank test with Bonferroni correction was conducted. As there were 21 pairwise comparisons, the new significance value was set at α=0.05/21=0.0024. Table 4 shows that TSD and positive reinforcement had the highest acceptance scores of 10 (8-10) and 10 (9-10), respectively. Although the median VAS score for both the techniques was the same, using the Wilcoxon sign rank test showed a significant difference between the two techniques as the distribution of the VAS scores was different, as can be seen in the box whiskers plot shown in Fig. (1). Protective stabilization, parental separation, GA, and voice control had the least median VAS scores, and the differences between those were not statistically significant. For each BMT, the comparison of median VAS scores for acceptance between males and females also did not show any significance (Table 5).
| S. No. | Techniques | Gender | VASMedian (IQR) | P-value |
|---|---|---|---|---|
| 1 | Tell show do | Male | 10(9-10) | 0.145 NS |
| Female | 9.5(8-10) | |||
| 2 | Nitrous oxide | Male | 8(6-10) | 0.745 NS |
| Female | 8(5-10) | |||
| 3 | Protective Stabilization | Male | 5(3-8) | 0.293 NS |
| Female | 7(4.25-8) | |||
| 4 | Voice Control | Male | 7(5-9) | 0.876 NS |
| Female | 7(5-8.75) | |||
| 5 | Parental Separation | Male | 6.5(3.75-8) | 0.576 NS |
| Female | 6.4(7.75) | |||
| 6 | Positive Reinforcement | Male | 10(9-10) | 0.924 NS |
| Female | 10(9-10) | |||
| 7 | General Anaesthesia | Male | 5(2.75-8) | 0.319 NS |
| Female | 6.5(2.25-9) |
4. DISCUSSION
Children demonstrate different behaviours in a clinical setting and wide-ranging in a dental treatment environment. The majority of children can be comforTable and cooperative throughout dental procedures. However, a handful exhibit disruptive behaviours, which makes it challenging for dental healthcare professionals to provide effective and appropriate treatment [16]. The purpose of this study was to assess the parental acceptance of various behavior management approaches in pediatric dentistry. The study found that most parents had higher acceptance of the non-pharmacological and communicative techniques (positive reinforcement, tell-show-do) as compared to general anaesthesia, and viewing videotapes of management techniques that explained the procedures helped them understand the process easily.
The children's behaviours are a reflection of their inability to cope with anxiety revolving around exposure to new environments, fear of dental healthcare professionals, and treatment procedures. Therefore, behaviour management techniques should instill a positive dental attitude in patients and parents to enable the dental team to perform an effective and efficient treatment to encourage the wards' long-term interest in improving dental health and preventing diseases. These techniques should also help in developing appropriate behaviour among the patients. Successful management of the patient during a procedure can be a challenging but fulfilling experience.
For better dental care delivery, pediatric behavior management should include equal and constant communication between the child, parents, and dentist [17]. The decision to use behavioural techniques other than communicative management should be the consolidated decision of the parents, and to assist the parents in making the best decision for their child, the practitioner should clearly discuss different treatment options, potential benefits, and risks. It should be conducted in their preferred language, respecting their culture. With the increased importance of informed consent in recent years, it has become imperative to disclose the detailed procedure to the parent before its application.
Several behaviour management techniques may not be equally accepted by parents due to a lack of information or knowledge. It also depends on their child’s treatment needs and their urgency, which influences both the selection and parental acceptance of that technique. Parental participation in child's healthcare experiences has increased; therefore, healthcare practitioners can no longer assume approval of any form of management procedures [17]. Previous studies [13, 17] have emphasized providing detailed information to the parents about the management techniques, so that they can be more accepting of these techniques.
Visualisation plays a crucial role in acquiring and transferring knowledge through a clear understanding of the concept taught by the presence of visual effects. There are multiple ways of imparting knowledge through role-playing, educational videos, visual aids, podcasts, etc [18]. We used a single video to demonstrate different behavioural management techniques to parents to measure their acceptance, and in this study, parents were observed to be more flexible towards communicative management approaches that were considered visually more acceptable, such as tell-show-do, live modeling, and positive reinforcement.
In the current study, videos were used to demonstrate behavior management techniques to the parents. Real-life scenarios helped to enact the procedures for the parents, providing them with a detailed act of the involved steps. Most parents are unaware of the use of behavioural management techniques in paediatric dental offices. Behavioural techniques, such as N2O and general anaesthesia, are rarely used, and thus are paradoxical for all parents to be aware of. Positive reinforcement and tell-show-do techniques had the highest level of parental acceptance in this study. These results are similar to the previous studies [13, 19, 20].
TSD, positive reinforcement, and voice control techniques are highly utilized by both general dental practitioners and pediatric dentists [6]. The high acceptance for tell–show–do and positive reinforcement is expected, as it is among the safest and least invasive. General anaesthesia is the least accepted management procedure among parents. The lower VAS score for GA corresponds with the results of previous studies [13, 20-22].
Desai et al. assessed the parents' attitude toward behaviour management by inspecting the impact of maternal anxiety on the child’s behaviour and the parent's presence during the treatment [18]. The study found that parents are more accepting of visually accepting techniques compared to aggressive management. It is similar to the findings of this study, where techniques, like voice control, protective stabilization, and parental separation, have shown parental acceptance of 57.7%, 56.2%, and 53.8%, respectively. These techniques, like protective stabilization, have been considered aggressive techniques from the parents’ point of view of their children. Therefore, parents tend to refrain from techniques that are unpleasant to their wards and would make them fearful [13]. As shown in previous research, parents prefer to stay alongside their child during the dental visit [13, 18]. Seangpadsa et al. indicated the least acceptance of the parental separation technique [23].
Nitrous oxide was acceptable by 75.4% of the parents in this study. There are diverging results concerning nitrous oxide sedation in previous researches [13, 18]. The frequency of nitrous oxide use at two referral centres in Saudi Arabia was 14.36%. After experiencing BMTs alongside their children, parents' attitudes toward nitrous oxide sedation improved substantially [24]. A study conducted in Germany and Jordan showed high acceptance of the nitrous oxide sedation technique [8].
Tell-show-do showed a significant association with gender distribution, wherein male parents had a higher acceptance. Both positive reinforcement and tell-show-do exhibited the highest VAS scores for both male and female parents. The study did not find any other significant difference in the level of acceptance between male and female parents.
The videotape used in this study was developed according to Saudi culture and local language requirements. It is vital to consider patients' social, economic, cultural, and linguistic factors while selecting a suitable behaviour guidance technique [9]. Furthermore, each culture has its own set of concepts, principles, and traditions, making it critical to learn how to establish rapport with patients from various backgrounds and to develop tools that assist them in managing the experiences they have [11]. By elaborating on and measuring parental preferences, this study assists the pediatric dentist in deciding on BMT. Furthermore, one of the study's benefits is that it contributes to the existing literature on parental acceptance of BMT during dental treatments. In addition, one of the strengths of this study is that it enriches the current literature on parental acceptance of BMT during dental procedures.
The study also has some limitations; the data collected only included the gender of the parents and did not include other characteristics, such as their economic status, which additionally serves as a determinant of the child's behavior. Furthermore, the study utilized convenience sampling, which may have resulted in sampling bias. The findings of the study cannot be generalized to the entire population of Saudi Arabia because only one region out of the country's eleven regions has been studied.
This study establishes the foundation for future research into the factors influencing the adoption of behavior management techniques in a dental context for the Saudi population. There is a need for research on developing highly communicative behaviour techniques that are patient-friendly, less traumatic, and invasive within the ethical norms acceptable to the parents while delivering safe all-around dental care.
CONCLUSION
Behaviour management is widely agreed to be a key factor in dental care for children. The current study documented that videotapes of behaviour management techniques and explaining the procedures to parents enabled them to understand them in a better way. Most parents showed higher acceptance of the non-pharmacological and communicative techniques (positive reinforcement, tell-show-do) as compared to general anesthesia. This high level of acceptance of these techniques suggests that parental acceptance is more substantial. Further studies are needed to compare the effectiveness of various BMTs among patients with special needs and of various socio-economic statuses (like autism spectrum disorder). Future studies could examine children's satisfaction and acceptance of dental care as well as the behavioural techniques used. It is important to continuously maintain optimal dentist-parent communication to address the patient’s/parents’ concerns sensitively and respectfully.
LIST OF ABBREVIATIONS
| AAPD | = American Academy of Pediatric Dentistry |
| BMP | = Behavior Management Technique |
| GA | = General Anaesthesia |
| IQR | = Interquartile Range |
| N2O | = Nitrous Oxide |
| SPSS | = Statistical Package for Social Sciences |
| TSD | = Tell-show-do |
| VAS | = Visual Analogue Scale |
| VC | = Voice Control |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This cross-sectional study was conducted at the Department of Orthodontic and Pediatric Dentistry, Qassim University, Saudi Arabi.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee, and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the [Zenodo Repository] at [https://zenodo.org/record/8378474].
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICT OF INTEREST
The authors state that they have no conflicting professional or personal interests that could have impacted the outcome or reporting of the research.
ACKNOWLEDGEMENTS
The authors would like to thank all participating parents for their great assistance in this study.

