All published articles of this journal are available on ScienceDirect.

Surgical and Orthodontic Management of Multiple Supernumerary Teeth Associated with Impacted Permanent Teeth: A Case Report
Abstract
Background:
Clinical problems are frequently detected when there are various irregularities in the number, structure, quantity, size, and eruption of the teeth. Supernumerary teeth can be found in almost any part of the dental arch, and because they are typically asymptomatic, they are frequently found by radiographic screening.
Case report:
The existence of the supernumerary teeth is the most frequent reason for impacted permanent teeth. This article describes the surgical and orthodontic treatment of a 20-year-old female with many supernumerary teeth and an impacted permanent tooth. All supernumerary teeth in the maxillary arch were extracted as part of the patient's treatment, and then the maxillary teeth were aligned using fixed appliances. The mandibular arch is left untreated, as the surgical removal of mandibular supernumerary teeth could damage the inferior alveolar nerve and result in numbness in the lower lip.
Conclusion:
In this case, we removed the extra teeth and used orthodontic traction to bring the remaining teeth into the proper position. After the procedure, the cosmetic outcome was greatly improved, and the patient's confidence increased.
1. INTRODUCTION
Permanent teeth will emerge to their functional occlusion throughout normal dental development and replace their predecessor's teeth. When variations in tooth eruption or abnormalities in tooth morphology are observed during the development of occlusion, pediatric dentists have to deal with challenging situations. It is possible for a variety of factors to hinder the proper positioning of the teeth, their harmonious interaction with adjacent and antagonistic elements, and the organic growth of the occlusion as a whole. Supernumerary teeth have been reported to cause a delay in the eruption of maxillary and mandibular teeth [ 1].
In the oral cavity, supernumerary teeth can develop anywhere. In the general population, maxillary midline supernumeraries (mesiodentes), which are most frequently observed, account for about 1 in 110 children's supernumerary teeth [ 2]. It is possible that there are several extra teeth, and they could all be impacted for many years, complicating the clinical settings. Supernumerary premolars are unique among supernumeraries in that they develop and retain later than expected, making treatment unpredictable and challenging [ 3].
The most frequently recognized theory for the cause of supernumerary is the localized hyperactivity of the dental lamina. However, the exact cause is unknown and may be complex, incorporating both hereditary and environmental factors [ 4-9]. The etiology and mechanisms that can result in extra teeth in the premolars or the maxillary midline are pretty similar. Three explanations were put up by Gardiner [ 10], including aberrant dental lamina proliferation, an additional follicle, and an extension of the dental lamina after the development of both the deciduous and permanent follicles (post-permanent type). It is theoretically feasible to place post-permanent supernumerary teeth since the development of the extra premolar root is delayed by 7-10 years.
Many racial and ethnic groupings have variable rates of supernumerary teeth. The prevalence ranges from 1% to 3% in the Caucasian population [ 11]. 90-98% of these occur in the premaxillary area. Supernumerary teeth occur more frequently among Asians, at a rate of greater than 3% [ 12]. Kids of Latino heritage were shown to have an occurrence of 5.6%, compared to black children's 0.42% [ 13]. In permanent teeth, the prevalence ranges between 0.15 and 1%, with a 2:1 preference for men [ 14, 15].
A tooth is predisposed to delayed eruption for reasons other than just the simple existence of an extra tooth. Other determining elements that may affect the outcome of the incisor eruption include their shape, number, and location. There are four types of additional teeth: conical or peg-shaped, invaginated or tuberculate, supplementary or incisiform, and odontome-shaped. Several incidences of delayed eruption of the maxillary incisors have been linked to the tuberculate or invaginated supernumerary type [ 16-18]. The clinician must identify the cause and create an effective treatment strategy when the incisors do not emerge at the anticipated period. The delayed eruption of the permanent teeth, impaction of the permanent incisors, prolonged retention of the deciduous teeth, ectopic eruption, root dilatation, etc., are the most common issues brought on by the presence of extra teeth in the maxillary or mandibular area.
Case management is difficult when there are numerous impacted and multiple supernumeraries, which further lengthens the course of therapy. In such circumstances, determining an appropriate treatment schedule, anchoring, planning, and implementing orthodontic biomechanics is challenging. In this case report, we provide a case of many supernumeraries with impacted permanent teeth managed surgically and orthodontically. Before beginning orthodontic treatment, the patient was advised to get routine X-rays, which is when the diagnosis was made. In these situations, an interdisciplinary approach is encouraged.
2. CASE REPORT
A 20-year-old girl visited the orthodontic clinic in a private practice. The main concern was the crowding in the maxillary arch and asking for teeth alignment. She was in good physical health, and the medical history was irrelevant. Upon examination, the patient had a mild skeletal class II malocclusion with crowding in the upper and lower arch, deep bite, and asymmetrical smile (Fig. 1).
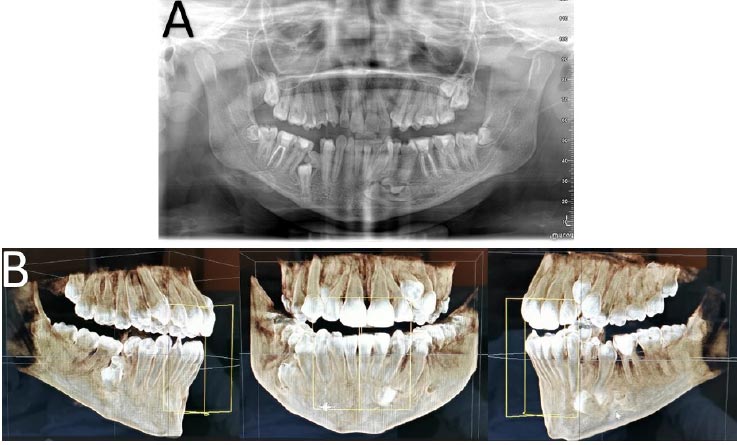
The panoramic radiograph showed an asymmetric condyle with multiple supernumerary teeth in the anterior and posterior area of the maxilla and mandible (Fig. 2a). A cone beam computed tomography (CBCT) was taken. It showed multiple supplemental impacted supernumerary teeth located mainly in the premolars and canine's area (Fig. 2b).


The following treatment options were considered: (i) Extraction of all supernumerary teeth under general anesthesia (G.A) followed by Orthodontic treatment with the fixed appliance to align the teeth' by closing spaces and correcting the deep bite. (ii) Extraction of all supernumerary teeth in the maxillary arch under G.A, followed by orthodontic treatment with fixed appliances to align the maxillary teeth with the mandibular arch left untreated because extraction of mandibular supernumerary teeth may disrupt the inferior alveolar nerve and produce numbness in the lower lip as a consequence following the surgical extraction. (iii) No extraction or orthodontic treatment. After discussing the available alternative treatment options with the patient, she chose the 2nd option treatment of the maxillary arch without treatment of the mandibular arch, to avoid the complication of the surgery.
Treatment was started by extraction of all maxillary supernumerary teeth under G.A. except the premolar supernumerary teeth located in the maxillary right side as it is located close to the sinus, and the orthodontic treatment concentrated only from 16 to 26. After that, the fixed orthodontic appliances were bonded to maxillary teeth from 16 to 26. Intraoral photograph after 15 months of orthodontic treatment (Fig. 3). After 19 months of orthodontic treatment, the fixed appliances were de-bonded, and the patient was given a clear vacuum retainer (Essix) as a removable retainer with fixed lingual retainer bonded from 3-3 in the maxillary arch (Ortho Flex Tech, Reliance Orthodontic, IL, USA) as shown in Figs. 4 and 5).


3. DISCUSSION
The normal position and eruption of neighboring teeth can be impacted by supernumerary teeth, necessitating frequent clinical intervention [ 15]. They can be erupted or unerupted and can be found in practically any area of the dental arch; they are frequently discovered during regular radiography evaluation. When an individual has multiple extra teeth, it is uncommon if there are no other linked illnesses or syndromes. This disorder results from interference with tooth development at its beginning stage. Although the precise cause of this disorder is unknown, several theories have been put forth, including dichotomy of the tooth bud [ 19], hyperactivity of the dental lamina [ 20], and a phylogenetic remnant of extinct ancestral tissue [ 1]. Both the primary and permanent dentitions may contain them, and they have the potential to crowd, hinder, postpone, or erupt ectopically nearby permanent teeth.
The most effective care of this issue is made possible by the early discovery of supernumerary teeth, frequently resulting in less invasive surgery, orthodontic treatment, and associated consequences. After the supernumerary tooth is extracted, the permanent incisors with immature roots emerge spontaneously [ 21]. However, in some circumstances, merely extracting the supernumerary tooth does not cause the spontaneous eruption of the permanent teeth [ 21, 22]. As a result, choosing an effective treatment strategy will also be aided by understanding the developing stage of an unerupted or impacted tooth. If the apex of the tooth has been closed, the impacted tooth's natural ability to erupt is lost, and the tooth will require active orthodontic assistance [ 21].
Supernumerary tooth management can be done using a variety of methods. However, most patients will need surgical and/or orthodontic modification. In some circumstances, conservative care is the preferred option. After the extra tooth is extracted, the patient undergoes the first stage of orthodontic treatment. Once the initial phase has produced enough arch space, active orthodontic treatment to extrude the unerupted incisor can start [ 11].
If there is not enough arch space, active orthodontic treatment might be used to create additional space before an eruption occurs. If a tooth does not begin to erupt after a year of removing the supernumerary tooth and there is enough arch space, surgical exposure followed by orthodontic movement of the impacted incisor is advised [ 23-25]. Orthodontic devices should be applied to teeth before beginning the surgical exposure to act as the proper anchoring and promote eruption. Arch alignment should have advanced to a stable archwire that will maintain the integrity of the tooth arch before beginning with orthodontic mechanical traction. The initial applications of elastic and ligature wire were in orthodontic traction. It can be connected to the bonded bracket from the archwire. This should allow the tooth to come out with minimal force. Unerupted or impacted teeth may take anywhere between 6 and 36 months to emerge, depending on where they are initially located within the jaw. Light forces must be used to force the tooth to erupt along the proper route; heavy forces may result in tooth resorption, ankylosis, or devitalization [ 24].
In this case, the premolar regions held most of the supernumerary teeth. Our results were consistent with earlier publications. Spontaneous supernumerary teeth typically develop in the premaxilla [ 5, 6]. However, in multiple supernumerary teeth, the premolar region (especially the mandibular premolar area) may predominate in the hyperdontia occurrence, followed by the molar and anterior areas, correspondingly. In the mandible, numerous supernumerary teeth may occur in roughly 60.9% of cases, with the premolar region accounting for about 44.8% [ 3, 6]. The position and orientation of the affected tooth, the degree of root completion, and the availability of space for the impacted tooth in the arch are a few considerations to take into account for the best alignment of an impacted tooth. Many authors may use different approaches. Typically, such teeth are extracted cautiously or, if practical, part of them are moved into the arch [ 7, 26]. Some people believe the extra tooth may be left in place if it has developed in a normal alignment and has not disrupted the occlusion. Instead of extracting it, the extra tooth would be followed up until it started to endanger the other structures. Space should be created as soon as possible to avoid crowding and occlusal disturbances if unavailable [ 7, 27]. An early extraction prior to future orthodontic treatments may be advised for impacted supernumerary teeth [ 8]. To avoid iatrogenic harm to neighboring teeth or anatomical structures, some dental practitioners suggest delaying treatment until the conventional permanent teeth fully erupt, or the supernumerary dental roots have finished erupting [ 7, 8, 28]. In the current situation, the orthodontic treatment in the maxilla was started before all the extra teeth were removed. However, in the mandible, supernumerary teeth were not extracted because of clinical considerations, i.e., they are close to vital structures, and the patient refused the extraction to avoid the complication of the surgical extraction. The treatment options were to accept the teeth without any intervention (no treatment), to extract the supernumerary teeth and align the teeth into occlusion in the maxillary arch only by orthodontics, like in this case or extract all the supernumerary teeth in both arches and align the teeth by orthodontics teeth movement.
CONCLUSION
Supernumerary teeth can be present in any region of the oral cavity. They can erupt or remain impacted and lead to complications. In order to satisfy the patient's and parents' expectations as well as other clinical problems, a clinician should develop a good treatment plan after discussing it with them in advance. In this case, we removed the supernumerary teeth in the maxillary arch only and used orthodontic traction to bring the remaining teeth into the proper position. The treatment was completed with a significantly enhanced aesthetic result and improved self-confidence.
ACKNOWLEDGEMENTS
Declared none.

