All published articles of this journal are available on ScienceDirect.

COVID-19 and Orthodontics: An Approach for Monitoring Patients at Home
Authors Info & Affiliations
Abstract
Aim:
The aim of this study was to test an experimental approach involving the remote monitoring of orthodontic patients through the use of their smartphones.
Background:
Due to the COVID-19 emergency, dental offices were asked to stop elective treatments; suddenly orthodontic patients found themselves isolated at home, without the possibility of monitoring by their orthodontists. The use of telemonitoring via smartphones can be a quick way to recover the orthodontist-patient relationship, monitor and continue the treatment.
Objective:
The purpose of this study was to propose an innovative, simple and reliable approach for the remote management of orthodontic patients.
Methods:
137 patients were contacted verbally by phone and via WhatsApp®; they were asked to send a set of photographs taken with their smartphone. They were asked to complete a questionnaire to evaluate the effectiveness of the approach. Descriptive statistics (frequency with percent) of questionnaire results and the presence of procedural errors while taking pictures were calculated. Correlations between different questionnaire answers were analyzed with the Chi-Square test. Variables with p < 0:05 were declared as significant.
Results:
The majority of patients considered that this approach was positive and they did not feel abandoned. Difficulties emerged from a technical point of view, that is, in terms of photoshoot, and part of the patients expressed perplexity regarding the fact that telemonitoring can replace completely an outpatient visit.
Conclusion:
The use of telemonitoring managed to recreate a relationship with the orthodontist, especially in emergency periods.
1. INTRODUCTION
An epidemic of Severe Acute Respiratory Syndrome-Corona Virus-2 (SARS-CoV-2) (COVID-19), a new strand of the coronavirus family, reported in Wuhan (China) in December 2019, was declared a pandemic by the World Health Organization as of 11 March 2020 (https://www.who.int /emergencies/diseases/novel-coronavirus-2019) [1-3]. The global pandemic of SARS-CoV-2 (COVID-19) has affected the delivery of health care worldwide [4-18].
Current guidelines require prolonged self-isolation at home to reduce the chances of virus infection [19-24].
ADA (American Dental Association) recommends dentists to postpone elective procedures and treat only emergencies for the period. Focusing on emergency dental care permits looking after COVID-19 patients and alleviating the affliction that dental emergencies would place on hospital emergency units [25].
The reduction in the dental offices’ activities, the cancellation of the appointments and the reluctance of the patients to book new consultation during this difficult period, can lead to a slowing down of the orthodontic treatments or to the onset of complications [26-42].
Each orthodontic treatment is characterized by a duration over time that normally varies from 1 to 3 years [43]. Orthodontic approaches are of different types, based on the patient's problem and on the age in which treatment is started. Orthodontic visits are usually repeated with a frequency of 3 weeks to a month and a half [44].
Remote therapy monitoring approaches have been proposed through the use of the smartphone.
Teledentistry is defined by the Association of American Medical Colleges as “the use of telecommunication technology to send data, graphics, audio, and video images between participants who are physically separated (i.e. at a distance from one another) for the purpose of clinical care” [45].
Orthodontists are nowadays enthusiastic to incorporate new discoveries and new technologies into their practices. Today because of the COVID-19 restrictions, there could be a large number of patients seeking to undergo orthodontic treatment with no chairside appointments while permitting the orthodontist to monitor their treatment progress.
Remote monitoring technology would be especially applicable to all procedures in which treatment advancement could be followed with virtual checkups to complement in-office visits. The evaluation can relate to the initial leveling and alignment, correction with maxillary expanders or orthopedic devices, monitoring oral hygiene status, and checking cooperation with elastic wear.
Telecommunication technology has been found to be especially useful in orthodontics because minor emergencies such as discomfort due to a wire or ligature displacement could usually be resolved at home without chairside appointments [6]. Another study that estimated the efficacy of a teledentistry system for the orthodontic analysis reported that “screening and accepting orthodontic referrals based on clinical photographs were equivalent to in-office visits in the clinical decision-making process” [46]. Therefore, digital telecommunication systems have been found to increase the management of health care [47-49]and nowadays, decrease the risk of contagion.
In this emergency period, there is often no time to re-organize the management of orthodontic patients electronically, but the simplified use of the smartphone could help guarantee therapeutic continuity and allow the recovery of a doctor/patient relationship essential for patient collaboration and the success of the therapy.
The aim of this study was to propose an innovative, simple and reliable approach in the distance-management of orthodontic patients and to test it using an “ad hoc” questionnaire.
2. MATERIALS AND METHODS
2.1. Sample
In this prospective study, participants were enrolled from the orthodontic patients of AB and BO, in active treatment between February and April 2020.
All patients were recruited from private dental offices where A.B. and B.O. work as orthodontists. The choice of patients was dictated by the possibility for the orthodontist to create a telephone contact. For this reason, a priori calculation of the sample size was not performed.
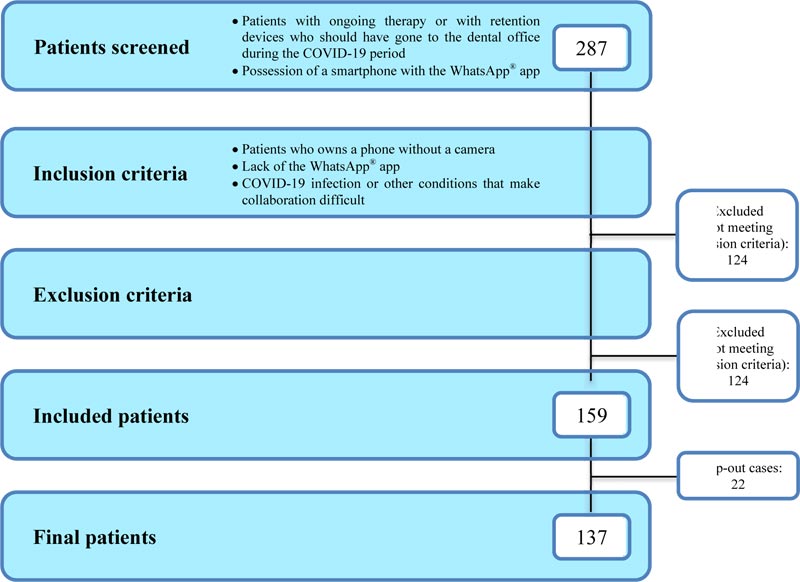
The inclusion criteria were patients in active treatment or in the retention phase, who should have gone to the dental office in the COVID-19 period; possession of a smartphone with the WhatsApp® app (WhatsApp Inc- Facebook Inc., Menlo Park, California, US).
The exclusion criteria were patients who own a phone without a camera; lack of the WhatsApp® app; COVID-19 infection or other conditions that make collaboration difficult.
After applying the inclusion and exclusion criteria, the number of initial patients was reduced from 287 to a final sample of 159 individuals (Fig. 1); a) 76 mobile orthodontic patients (35 males and 41 females; mean age: 7.82 years); b) 73 braces patients (31 males and 42 females; mean age: 15.75 years). All participants, or their parents when applicable, provided written informed consent for their participation in this study, after receiving information regarding the study protocol. The study was conducted in accordance with the Declaration of Helsinki. The study was not submitted to the ethical committee due to the unexpected situation of the COVID-19 emergency.
2.2. Variables Recorded
The telemonitoring process was carried out in the following way:
- A first telephone interview to recreate an adequate orthodontist /patient relationship. During the call, the dentists asked if the patients had orthodontic emergencies such as, for example, ulcerations, infections, pain due to loose orthodontic ligatures or brackets [50].
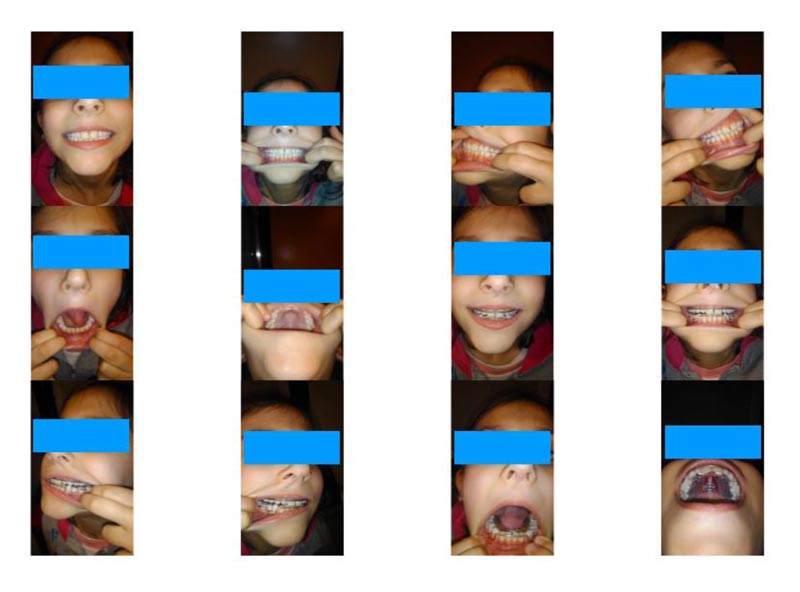
- Patients sent six photographs via WhatsApp® application after taking them autonomously. They had to take the photos with the flash always activated and using fingers to move the lips apart. The shots allowed to observe the patient's smile, the frontal projection of the mouth in occlusion, the right and left lateral projections in occlusion, the maxillary arch and the mandibular arch in occlusal view (Fig. 2).

In the orthodontic treatments with mobile devices, the photos were taken with and without the device; this allowed to observe how the device was worn and whether it determined changes in the mandibular posture or not (protrusion, retrusion, correction of mandibular deviation).
In the orthodontic treatments with extraoral devices, the photos allowed to control how they were worn and the elastics' direction.
In the orthodontic treatments with multi brace systems, photos had to be taken with and without intra- and inter-maxillary elastics.
After receiving the photos, the orthodontist could advise patients in order to improve or eliminate problems such as wrong framing, blur, absence of light, or incomplete vision.
Patients' opinions on telemonitoring were assessed through a questionnaire. We conducted a literature review to identify whether a previously validated questionnaire already existed which resulted in an unsuccessful attempt. We therefore decided to build a short specific questionnaire based on expert judgments, on the relative review of the literature and on interviews with patients or parents to evaluate individual problems. Due to the emergency context, a preliminary pilot test has not been performed. We only compared it with a previous questionnaire created for a study conducted at the University of Brescia; in this study, Dalessandri et al. analyzed the attitude of 30 orthodontists and 40 patients towards the use of dental monitoring in their daily practice [51-53]. We carried out this comparison in order to identify any possible source of confusion on any element and, subsequently, the questionnaire was accordingly revised. In the final version of our questionnaire, there were two answers, “yes” or “no”, for eight different questions and we sent it using the WhatsApp® application (Table 1).
| 1 | Were you aware of the possibility of remote treatment? |
| 2 | Do you judge telemonitoring positively? |
| 3 | Was the explanation of the telemonitoring system simple? |
| 4 | Was the shooting of the photographs easy? |
| 5 | In an emergency situation and inability to carry out outpatient checks, can telemonitoring replace an outpatient check or not? |
| 6 | Were the indications provided by the orthodontist exhaustive? |
| 7 | With this therapeutic approach, did you perceive that the orthodontist took care of you? |
| 8 | At the end of the emergency period, would you agree using telemonitoring for future checks? |
This research received no external funding. The data supporting the findings of the article is available in the repository at the private practices of A. B. and B. O, with reference number COVID-19.
2.3. Statistical Analysis
Descriptive statistics of questionnaire results and the presence of procedural errors while taking pictures were calculated. Statistical analysis of data was performed using the Statistical Package for the Social Sciences, version 24.0 for Windows (SPSS Inc., Chicago, Illinois, USA). Correlations between different answers were analyzed with the chi-square test (significance level: p-value <0.05).
3. RESULTS
After making the phone calls, we received all the photos within 3-4 days. The orthodontist's responses and comments were straightforward and, in some cases, new shots were required to improve the analysis of the oral cavity. Forty-nine patients had to take photographs again and the orthodontist had to request new shots to complete the visual analysis. The most common errors were lack of flash (31), blurred photo (19), incomplete shot (16), modification of the mandibular posture by the patient (40).
After receiving the photos, the questionnaire was sent to all patients via WhatsApp®.
Patients were asked to answer the questions by sending a message characterized by the sequence of 8 answers between YES or NO (example: YES-NO-YES-NO-YES-NO-YES-NO). 137 patients replied, 22 did not reply to the message.
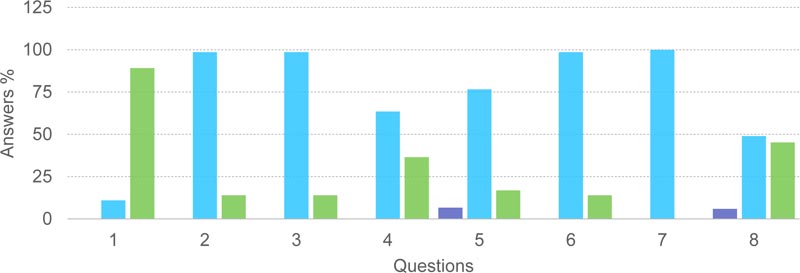
The knowledge of the possibility of treatment by telemonitoring (Question 1) was unknown to the majority of patients (89.1%), although 98.6% of patients judged this possibility positively (Question 2).
Communication, characterized by a first telephone approach and by sending a message via WhatsApp® subsequently, was judged by 98.6% of patients as simple and intuitive (Question 3).
The personal ability to take pictures correctly was instead a reason for separation into two distinct groups: 36.5% of the patients found it difficult to take the pictures correctly, 63.5% had no difficulties (Question 4).
When asked if telemonitoring could replace an outpatient check in an emergency, 6.6% did not answer, 76.6% answered in an affirmative way, while 16.8% answered negatively (Question 5).
The data supporting the findings of the article are available in the authors’ private repository, which will be available upon request.
The indications that the orthodontist gave after viewing the photos via WhatsApp® were considered exhaustive by 98.6% of the patients (Question 6), and 100% of the patients believed that the orthodontist took care of them (Question 7) (Fig. 3).
The possibility that this type of therapeutic approach can be repeated even outside this circumstance of emergency was agreed by 48.9%, while 45.2% did not consider it appropriate and 5.9% did not answer (Question 8).
| QUESTIONS | NO ANSWER | YES | NO | TOTAL | |
|---|---|---|---|---|---|
| 1 | Were you aware of the possibility of remote treatment? | 0 (0%) |
15 (10.9%) |
122 (89.1%) | 137 |
| 2 | Do you judge telemonitoring positively? | 0 (0%) |
135 (98.6%) |
2 (1.4%) | 137 (100%) |
| 3 | Was the explanation of the telemonitoring system simple? | 0 (0%) |
135 (98.6%) |
2 (1.4%) | 137 (100%) |
| 4 | Was the shooting of the photographs easy? | 0 (0%) |
87 (63.5%) |
50 (36.5%) | 137 (100%) |
| 5 | In an emergency situation and inability to carry out outpatient checks, can telemonitoring replace an outpatient check or not? | 9 (6.6%) |
105 (76.6%) |
23 (16.8%) | 137 (100%) |
| 6 | Were the indications provided by the orthodontist exhaustive? | 0 (0%) |
135 (98.6%) |
2 (1.4%) |
137 (100%) |
| 7 | With this therapeutic approach, did you perceive that the orthodontist took care of you? | 0 (0%) |
137 (100%) |
0 (0%) |
137 (100%) |
| 8 | At the end of the emergency period, would you agree using telemonitoring for future checks? | 8 (5.9%) |
67 (48.9%) |
62 (45.2%) |
137 (100%) |
Several correlations between different answers were tested with the chi-square test, looking for the presence of strong statistically significant correlations. All chi-square tests were statistically significant, except for the relationship between question 6 (Were the indications provided by the orthodontist exhaustive?) and question 2 (Do you judge telemonitoring positively?); in this case, all patients who rated telemonitoring positively also found the indications given by the orthodontist to be exhaustive (Fig. 4).
| Answers Association | Chi-Square | p-Value |
|---|---|---|
| Q1 vs. Q2 | 212.13 | <0.00001 |
| Q2-Q3 vs. Q4 | 54.69 | <0.00001 |
| Q2 vs. Q5 | 21.11 | <0.00001 |
| Q2 vs. Q6 | 0 | 1 |
| Q2 vs. Q8 | 78,97 | <0.00001 |
| Q5 vs. Q8 | 26.29 | <0.00001 |
4. DISCUSSION
The inability to leave home and the need to continue the orthodontic therapies of our patients prompted us to investigate the potential of teledentistry.
Italy was the first European nation severely affected by COVID-19 and the lockdown period abruptly interrupted normal life. The Decreto-legge 25 marzo 2020, n. 19 “Urgent measures to deal with the epidemiological emergency from COVID-19. (20G00035)” declares “ The limitation of the movement of people, limitations on the possibility of moving away from one's own residence, domicile or residence except for individual travel limited in time and space or motivated by work needs, from situations of necessity or urgency, from health reasons or from others specific reasons”; “The limitation or suspension of other business activities or professional, even when involving the exercise of public functions, as well as self-employment, with the possibility of excluding public service needs after the assumption of anti-contagion safety protocols and, where it is not possible to respect the predetermined and adequate interpersonal safety distance, increase or reduce the risk of contagion as a main containment measure, with the adoption of adequate individual protection tools” [12].
So, we were forced to investigate what results teledentistry can achieve. There are not many studies available at the moment regarding this subject [54-59]. A monitoring technology (DM, Dental Monitoring) that combines mobile phone applications with artificial intelligence has become available for orthodontists to follow their patient’s treatment remotely. The orthodontic monitoring software allows tracking of tooth movement using the images of scanning videos taken by the patient using specific cheek retractors through a smartphone application (Android, iOS). The doctor’s interface with the monitoring software makes it possible to monitor treatment progress in real-time between office visits. The doctor may receive an alert if a problem is detected, such as a broken appliance, poor hygiene, or gingival recession. In this way, many appointments requiring simple evaluation may be eliminated, and it is possible that the use of this technology could decrease cost and chairside time while improving the delivery of orthodontic care [60].
Moylan et al. investigated the reliability and accuracy of a monitoring system in patients undergoing orthodontic treatment with a rapid maxillary expander. In their pilot study, the use and the accuracy of smartphone devices were able to give the possibility of an accurate monitoring of the therapy and even to make some measurements through the use of a dedicated software [61].
According to a survey by the Pew Research Center, nowadays the diffusion of smartphones is very vast. It shows that the percentage of those having a smartphone in the eighteen advanced economies surveyed is on average 76%, against 45% of those who live in an emerging country [62].
Today, more than 5 billion people have mobile devices, and over half of these connections are smartphones.
In Italy, according to CENSIS, in 2018, the number of mobile phones exceeded that of TVs; in each family, there were on average 4.6 mobile devices. In particular, in Italian houses, there were 43.6 million smartphones and 42.3 million televisions [63].
The possibility of a dialogue through this tool is now within everyone's reach and the younger generations, who are most involved in orthodontic treatments, have great affinity and ability to use it.
In developed nations, the age group that mostly uses smartphones is that which extends between 13 years and 25 years.
The spread of the WhatsApp® application allows a quick dialogue between smartphones. WhatsApp® (formally Whats App® Messenger) is an instant messaging computer application, created in 2009 and part of the Facebook Inc. group since 19 February 2014. The application allows you to send and receive large numbers of photographs. Users can exchange text messages, images, videos and audio files, as well as location information, documents and contact information between two people or in groups [64-73].
With the therapeutic approach used in this study, all patients positively responded to the orthodontist's invitation and behaved in a cooperative and interesting way; all of them were very happy with recreating the orthodontist-patient relationship.
The photos allowed to monitor the progression of the therapy from an orthodontic point of view, the eruption time of the deciduous and permanent dentition, the consequences of the activation of the devices, the progressions determined by the activity of arches or by the effectiveness of the elastic bands.
We also managed to check the possible detachments of brackets, the integrity of mobile devices and orthodontic masks. In all our patients wearing removable retainers, we also checked the post-orthodontic compliance, as the study by Zotti et al. showed previously [74].
Other information we recovered was the quality of oral hygiene, the state of health of the gingival support, the presence of fistulas or lesions of the oral mucosa.
Some studies highlighted the possibility of monitoring oral hygiene effectively, thanks to WhatsApp®; these studies involved children and adolescents, who were the populations most involved in this study, and the results confirmed the possibility of good remote oral hygiene monitoring [75-79].
All this can certainly allow us to define the priority of future appointments when the general conditions will allow the resumption of work.
Most of the patients who participated in this study were at the first experience of remote treatment, in particular, in the dental and orthodontic fields (Question 1). The diffusion of telemonitoring in Italy is still quite scarce; on the 23rd of December 2009, the European Economic and Social Committee issued an opinion on the communication COM (2008) 689. In the conclusions of the document, telemedicine is defined as a sort of “cultural revolution”, whose development must be seen in the context of a general evolution of health policies and systems [80]. About ten years have passed since this topic started spreading, and at the moment, the population neither has been sufficiently informed about nor has it included telemedicine and telemonitoring in daily lives.
Teledentistry is aimed to have in the future a strategic importance, also thanks to the possible interaction and integration with other digital improvements, such as Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM) systems and Cone Beam Computed Tomography (CBCT); these digital technologies combined together allow to create a “virtual patient”, to manufacture fully customized appliances, and to real-time monitor treatment effects. Additionally, the patients’ feedback for these systems is generally positive, so CAD CAM and CBCT technologies could be easily linked with telemedicine, thus reducing the number of in-office visits [81-87].
However, patients appreciated telemonitoring, especially in relation to the opportunities that this therapeutic approach allows continuity of therapeutic assistance, recreation of the orthodontist-patient relationship, possibility of asking questions, eliminating doubts, possibility of receiving from the orthodontist therapeutic indications useful for continuing the therapeutic treatment (Question 2). Therefore, although not aware of this therapeutic system, it is interesting to note that the lack of knowledge is not associated with the lack of appreciation of the topic, but it is exactly the opposite (Question 1 vs. 2).
The ability to send explanatory photos, write messages and speak directly through the WhatsApp® application made orthodontist / patient communication simple, effective and unambiguous (Question 3).
Although telemonitoring was appreciated and the explanation was simple, the execution was not automatic (Questions 2/3 vs. 4). Some difficulties emerged instead in the management of the smartphone like a camera (Question 4); most of the parents or relatives of the patients have never taken photographs of the oral cavity and none of them has ever been instructed by the orthodontist or has undergone a learning training that would allow them to take documentation photographs in such a specialized area. This type of photographic set certainly puts those in difficulty who, in this period of isolation, found themselves alone at home. In fact, some patients had to take a greater number of photos using the reflection of the home mirror to complete the photographic investigation.
Considering telemonitoring an approach capable of replacing an outpatient visit, it revealed a not low percentage of patients who considered it impossible (16.8%); outpatient visits were considered certainly more accurate, allowing the orthodontist to investigate the oral cavity in a better way. In fact, patients perceived a higher therapeutic quality in direct visits. (Question 5) However, assuming that this was done in an emergency setting, so the compromise was acceptable for most patients (Question 2 vs 5).
In Question 8, however, when we assumed that telemonitoring could become part of the orthodontic routine outside an emergency period, the number of people who considered this approach not as appropriate as normal visits increased to 45.2% (Question 5 vs. 8); just over half of them preferred to integrate telemonitoring into the orthodontic routine, many still feared that the quality of therapy might deteriorate if the number of visits and the direct relationship with the orthodontist were reduced (Question 2 vs. 8).
In our opinion, remote monitoring should be introduced into clinical practice by alternating outpatient visits with remote controls in order to improve therapeutic quality by reducing appointments in the office, promoting home dental practice movements in cases where, for example, only checking the progress of the dental exchange or the quality of the patient's general hygiene is required.
Finally, the possibility of obtaining indications from the orthodontist (moving the insertion points of the elastics, activating the mobile devices, etc.) was highly appreciated by the patients (Question 6), who did not feel abandoned (Question 7). In fact, the potential to have a telephone contact or to send WhatsApp® messages allowed us to provide the patient with useful information to deal with any orthodontic problems as indicated by Caprioglio et al. in their recent article [88].
In our opinion, perhaps these were the factors that allowed patients to evaluate telemonitoring so positively (Question 6 vs. 2: chi-square statistics: 0 p-value = 1).
The critical aspects of this study are many: the orthodontist was not aware of the tools (the smartphone) that the patients had and the quality of the images was different depending on the smartphone used. The previous absence of training led to the onset of many errors and the request by the orthodontist for frequent reshooting. On the other hand, the collaboration of the patients was very high; the responses were fast and in a short time, we received the requested material and answers. This was certainly due to the speed of communication that WhatsApp® allowed us, but also to the high availability of time that we all had in that period. The questionnaire was sent only once after one virtual appointment, therefore patients’ compliance over time was not evaluated, rather than the frequency of these “virtual appointments”. The hypothesis of continuing with a teledentistry approach may encounter a series of problems, delays or communication difficulties which are certainly more frequent in everyday life.
CONCLUSION
In an emergency period, because of the high risk of disease transmission within the orthodontic practice, it was important that orthodontists sought new therapeutic approaches. The use of smartphones positively helped to recreate a useful orthodontist-patients relationship allowing the orthodontist to follow the progression of therapy and to stimulate patient cooperation.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was not submitted to the ethical committee due to the unexpected situation of COVID-19 emergency.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All patients signed the standard consent form, authorizing the use of their personal data for research purposes.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the University of Brescia repository “OPENBS IRIS” at http://hdl.handle.net/11379/539557, reference number 539557 (COVID-19 and Orthodontics database).
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

