All published articles of this journal are available on ScienceDirect.

COVID-19 Associated Stress Among Dental Students
Abstract
Background:
The COVID-19 pandemic has exposed the global population to a high risk of infection that constitutes a major stress factor, especially for vulnerable groups such as dental students.
Objective:
To assess levels of COVID-19 related stress and anxiety, changes in hygienic and social habits, as well as subjective worries regarding the dental profession among dental students.
Methods:
A self-structured questionnaire was sent to students at the College of Dentistry, Umm Al-Qura University. It included demographic data, questions about the level of change in personal hygiene and social habits, students’ perception about the sufficiency of information received during the outbreak and its source, subjective worries regarding the dental profession, and the Generalized Anxiety Disorder 7-item (GAD-7) scale. Two hundred fifty-eight responses were received.
Results:
Moderate and severe anxiety were reported in 17% and 4% of students, respectively, with non-significant associations between anxiety and gender or level of study. A high percentage of students (46.5% to 62.4%) reported great change in most hygienic and social habits with a highly significant association between change in buying more sanitizers and anxiety levels. Forty-six percent agreed that their job performance was not at its best, and 31% reported a possible intention to change profession, with the latter reported more by male students (63.8%).
Conclusion:
A considerable percentage of dental students in our college are anxious and changed their hygienic and social habits due to COVID-19. This anxiety reflects worries about the dental profession in one-third of participants that necessitate counselling services and psychological support.
1. INTRODUCTION
Human coronaviruses are a family of viruses that can cause human diseases ranging from the common cold to Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS-CoV). Both SARS and MERS-CoV caused global epidemics with high mortality and morbidity rates in 2003 and 2012, respectively [1]. In December 2019, an outbreak of a novel virus from the beta-coronavirus family was identified in Wuhan, China, causing coronavirus disease 2019 (COVID-19) [2, 3]. On March 11, 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a global pandemic [4].
COVID-19 has the potential to cause a severe acute respiratory tract infection in infected humans. It is commonly transmitted from person-to-person via respiratory droplets, hands, saliva, and surface contact [5, 6]. The average incubation period for COVID-19 ranges between 4 and 14 days after exposure. The infected person usually presents with an acute upper respiratory tract infection and symptoms, including fever, dry cough, and tiredness. The severity of symptoms ranges from very mild to severe. Elderly people and those who have existing chronic medical conditions are the most vulnerable groups. Since COVID-19 is highly contagious, the rate of case detection rapidly became very high. Many organizational bodies launched web-based systems (dashboard) where the number of infected people could be tracked in almost real-time. On July 20, 2020, 19:55 hours (GMT), the number of confirmed cases worldwide was 14,567,109 and reported deaths were 607,187, with 8,804,227 recovered patients [7]. In Saudi Arabia, the number of confirmed cases was 253,349 and reported deaths were 2,523 cases with 203,259 recovered patients [8].
The first case of a dentist testing positive for COVID-19 was reported on January 23rd, 2020, in the Dental Hospital of Wuhan University, China. This was shortly followed by the identification of the transmission of disease to a further eight oral healthcare professionals [9]. Since then, more health care workers have tested positive for COVID-19 worldwide [10]. This has made the healthcare community more distressed as they are subjected to the highest risk of infection.
The rapid spread of COVID-19, that is difficult to control, compelled most governments worldwide to take serious measures in an attempt to slow down and control the epidemic. Curfews, home isolation measures, social distancing, closure of schools and universities, and shifts in the existing educational system to E-learning/distance learning systems were all implemented. Although these measures play a great role in controlling the spread of the epidemic, they are expected to put significant psychological stress on the students and may negatively affect their learning outcomes and overall psychological health. In particular, the nature of dental clinical training, the characteristics of dental settings, and the high risk of cross-infection between dental students undergoing their clinical training and patients could all contribute to provoking stress and anxiety among dental students and increase their worries about the future of their profession.
Previous published works have studied the psychological impact of infectious disease outbreaks, such as MERS and SARS, on students. One such study reported that almost one-quarter of medical students in Saudi Arabia recorded mild to moderate anxiety levels during MERS and SARS outbreaks [11]. Another study in Hong Kong reported that anxiety levels were found to be significantly higher among medical students than non-medical students [12]. Since the COVID-19 outbreak, very few studies have been conducted to estimate the effect of this pandemic on the psychological health of students [13, 14], but none has been carried out on dental students in Saudi Arabia.
The aim of this study was to evaluate the level of stress and anxiety associated with COVID-19 among dental students at the College of Dentistry, Umm Al-Qura University and to explore the level of change in their personal hygiene and social habits in response to COVID-19 as well as their subjective worries regarding the dental profession.
2. MATERIALS AND METHODS
2.1. Study Design and Ethical Considerations
This study utilized a descriptive cross-sectional design and was conducted at the College of Dentistry, Umm Al-Qura University, Makkah, Saudi Arabia, between May 27 and June 10, 2020. Makkah was selected for the study as it is the only city that had total lockdown restrictions during the spread of COVID-19 in Saudi Arabia and has only one college of dentistry.
The study protocol was approved by the Institutional Review Board (IRB) of the college (No. 175-2). Questionnaire submission by the students was considered as consent from their side to participate in this study.
2.2. Study Population
Undergraduate dental education in Saudi Arabia provides basic training to students over a period of 5 years, starting from Grade 2 after passing preparatory year for medical colleges. After this basic training, students undergo a 1-year internship before being eligible to receive a Bachelor's Degree in Dental Science (BDS) and a license to practice. Convenience and snowball sampling (students were asked to forward the questionnaire to their colleagues) were used to ensure maximal participation. Two hundred fifty-eight (258) study subjects out of a total of 300 students in the college responded to the questionnaire. The study was performed during the summer holiday before registration of the next academic year Grade 2 students and, therefore, the study included junior students of the 3rd and 4th academic year as well as senior students of 5th and 6th academic years together with dental interns.
2.3. Study Questionnaire
A detailed, anonymous, structured questionnaire designed by authors as an online Google form of 27 items in six sections was posted to study participants along with its link via the WhatsApp platform. The first section included an introduction to the research that emphasized the confidentiality of the questionnaire. The second section included four questions related to demographic data (age, gender, study level, and university name). The third section of eight questions focused on the level of change in personal hygiene and social habits in response to COVID-19 on a 5-point Likert scale (did not know, did not change, changed a little, moderately changed, and greatly changed). The fourth section contained two questions about students’ perception of the sufficiency of information they received about COVID-19 during the outbreak on a 5-point Likert scale (excellent, good, fair, poor, and very poor) and source of that information (college and university announcement, ministry of health, World Health Organization, media [TV and news], and social media). The fifth section had six questions focused on subjective worries regarding the dental profession with a Yes or No option and its rate on a scale from 1 to 10. Lastly, the sixth section of the Generalized Anxiety Disorder 7-item (GAD-7) scale included seven questions about the level of anxiety they felt over the preceding two weeks due to the COVID-19 outbreak. Each question in the scale was graded on 4- point scale (not sure, for 2-3 days, more than half of the days and nearly every day) scored from 0 (not sure) to 4 (nearly every day). Total scores of 5, 10, and 15 were taken as the cut-off points for mild, moderate, and severe anxiety, respectively, where 0-4 was considered as none to minimal anxiety, 5-9 as mild anxiety, 10-14 as moderate anxiety, and 15-21 as severe anxiety [15].
2.4. Validity and Reliability of the Questionnaire
A pilot study to test the precision of survey questions was conducted with 10 participants. Based on their responses, three survey questions were modified, and the format was edited for clarity and comprehensibility. A second pilot study was conducted with another 10 participants to confirm the feasibility, validity, and reliability of the questionnaire. To avoid questionnaires’ bias, google form was designed to accept the submission of completely answered questionnaires only. Each participant was allowed a single submission only.
2.5. Statistical Analysis
Data was entered and analyzed using the Statistical Package for Social Sciences (SPSS 20, IBM, Armonk, NY, United States of America). Descriptive statistics were used to describe the data where frequency and percentage for categorical variables were determined. The subjective worries regarding the dental profession and total GAD-7 score were described by the mean and standard deviation. Pearson's Chi-square test was used to assess the association between anxiety level and gender, level of study, personal hygiene, and social habits, as well as the subjective worries regarding the dental profession. A Chi-square test was also used to study the association between the possible intention to choose another profession and gender and study level. A critical probability value (P-value) of <0.05 was used as the cut-off level for statistical significance.
3. RESULTS
3.1. Demographic Data
The responders were 258 students out of 300 total students from the College of Dentistry, Umm Al-Qura University, giving a response rate of 86%, with 104 (40.3%) males and 154 (59.7%) females, and an age range of 18-26 years. The participants included 53 (20.5%) third grade, 45 (17.4%) fourth grade, 49 (19%) fifth grade, and 47 (18.2%) sixth grade students, and 64 (24.8%) dental interns.
3.2. Source of Students’ Information about COVID-19 and their Perception of the Sufficiency of the Information Provided
The Saudi Ministry of Health was the main source of information to the greatest number of students (n = 136 [52.7%]), followed by social media (60 [23.3%]), then the WHO (43 [16.7%]), followed by the media, including TV news (16 [6.2%]), and finally college and university announcements (3 [1.2%]). Most of the students (120 [46.5%]) reported that the information they received was excellent and 111 students (43.0%) considered it as good, 25 students (9.7%) thought it was fair and only one student thought it was poor.
3.3. Level of Anxiety Felt in the Preceding 2 Weeks Due to COVID-19 Outbreak
The level of anxiety felt over the preceding 2 weeks due to COVID-19 varied between dental students. From Fig. (1), it can be observed that 40% of the students had no or minimal symptoms of anxiety, while 4% reported severe anxiety.

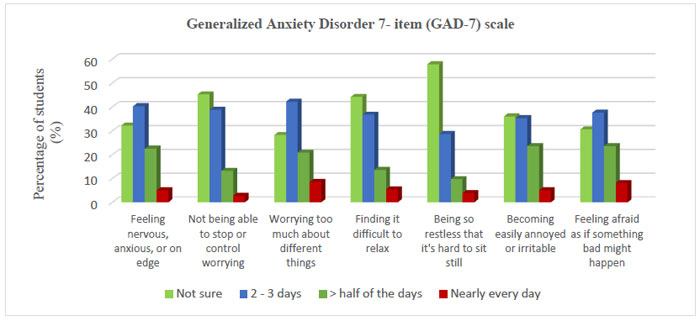
The mean values of responses to each item of the GAD-7 score are shown in Fig. (2). Here, the lowest percentages of students reported anxiety nearly every day. The mean total GAD-7 score was 6.20 ± 4.38.
There was no significant association detected between anxiety level and gender or level of study (Table 1).
3.4. Level of Change in Personal Hygiene and Social Habits in Response to COVID-19 and its Association with Anxiety Level
Table 2 shows that the highest percentages of students (46.5-62.4%) reported that they had greatly changed in all personal hygiene measures and social habits except for handwashing technique, buying more sanitizers, and avoidance of social gathering, where the greatest percentages of them (31.8-60.9%) were moderately changed. A highly significant association was observed between changes in the behavior of buying more sanitizers and anxiety level, where percentages of students with greatly changed habits increased with increased levels of anxiety while in compliance with standard precautions, the association with anxiety level was significant.
| Variables | Anxiety level | Chi-square | |||||
|
None/Minimal (n = 103) |
Mild (n = 101) |
Moderate (n = 45) |
Severe (n = 9) |
X2 | P-value | ||
| Gender | Male | 43 (41.7%) | 35 (34.7%) | 22 (48.9%) | 4 (44.4%) | 2.872 | 0.412 |
| Female | 60 (58.3%) | 66 (65.3%) | 23 (51.1%) | 5 (55.6%) | |||
| Level of study | 3rd | 25 (24.3%) | 23 (22.8%) | 5 (11.1%) | 0 (.0%) | 7.829 | 0.798 |
| 4th | 16 (15.5%) | 18 (17.8%) | 8 (17.8%) | 3 (33.3%) | |||
| 5th | 19 (18.4%) | 19 (18.8%) | 9 (20.0%) | 2 (22.2%) | |||
| 6th | 17 (16.5%) | 19 (18.8%) | 9 (20.0%) | 2 (22.2%) | |||
| Dental Interns | 26 (25.2%) | 22 (21.8%) | 14 (31.1%) | 2 (22.2%) | |||
| Personal hygiene and social habits | Response |
Total n. (%) |
Anxiety level | Chi-square | ||||
|
None/Minimal n. (%) |
Mild n. (%) |
Moderate n. (%) |
Severe n. (%) |
X2 | P-value | |||
| Handwashing technique | R1 | 3 (1.2) | 0 (0.0) | 3 (3.0) | 0 (0.0) | 0 (0.0) | 18.149 | 0.111 |
| R2 | 24 (9.3) | 12 (11.7) | 7 (6.9) | 4 (8.9) | 1 (11.1) | |||
| R3 | 34 (13.2) | 19 (18.4) | 9 (8.9) | 5 (11.1) | 1 (11.1) | |||
| R4 | 100 (38.8) | 42 (40.8) | 43 (42.6) | 14 (31.1) | 1 (11.1) | |||
| R5 | 97 (37.6) | 30 (29.1) | 39 (38.6) | 22 (48.9) | 6 (66.7) | |||
| Buying more sanitizers | R1 | 2 (0.8) | 0 (0.0) | 0 (0.0) | 2 (4.4) | 0 (0.0) | 32.043 | 0.001** |
| R2 | 24 (9.3) | 11 (10.7) | 11 (10.9) | 2 (4.4) | 0 (0.0) | |||
| R3 | 75 (29.1) | 39 (37.9) | 31 (30.7) | 3 (6.7) | 2 (22.2) | |||
| R4 | 82 (31.8) | 26 (25.2) | 29 (28.7) | 24 (53.3) | 3 (33.3) | |||
| R5 | 75 (29.1) | 27 (26.2) | 30 (29.7) | 14 (31.1) | 4 (44.4) | |||
| Wearing surgical masks and gloves outdoor | R1 | 5 (1.9) | 2 (1.9) | 3 (3.0) | 0 (0.0) | 0 (0.0) | 15.004 | 0.241 |
| R2 | 22 (8.5) | 11 (10.7) | 4 (4.0) | 6 (13.3) | 1 (11.1) | |||
| R3 | 42 (16.3) | 18 (17.5) | 20 (19.8) | 3 (6.7) | 1 (11.1) | |||
| R4 | 59 (22.9) | 23 (22.3) | 28 (27.7) | 7 (15.6) | 1 (11.1) | |||
| R5 | 130 (50.4) | 49 (47.6) | 46 (45.5) | 29 (64.4) | 6 (66.7) | |||
| Following social distancing (2m apart) | R1 | 3 (1.2) | 1 (1.0) | 2 (2.0) | 0 (0.0) | 0 (0.0) | 13.685 | 0.321 |
| R2 | 14 (5.4) | 6 (5.8) | 8 (7.9) | 0 (0.0) | 0 (0.0) | |||
| R3 | 47 (18.2) | 20 (19.4) | 17 (16.8) | 10 (22.2) | 0 (0.0) | |||
| R4 | 74 (28.7) | 36 (35.0) | 25 (24.8) | 11 (24.4) | 2 (22.2) | |||
| R5 | 120 (46.5) | 40 (38.8) | 49 (48.5) | 24 (53.3) | 7 (77.8) | |||
| Avoid social gathering | R1 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 14.540 | 0.104 |
| R2 | 6 (2.3) | 3 (2.9) | 3 (3.0) | 0 (0.0) | 0 (0.0) | |||
| R3 | 32 (12.4) | 7 (6.8) | 20 (19.8) | 5 (11.1) | 0 (0.0) | |||
| R4 | 63 (24.4) | 22 (21.4) | 23 (22.8) | 14 (31.1) | 4 (44.4) | |||
| R5 | 157 (60.9) | 71 (68.9) | 55 (54.5) | 26 (57.8) | 5 (55.6) | |||
| Avoid hand shaking | R1 | 1 (0.4) | 1 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 10.655 | 0.559 |
| R2 | 10 (3.9) | 3 (2.9) | 4 (4.0) | 3 (6.7) | 0 (0.0) | |||
| R3 | 33 (12.8) | 13 (12.6) | 18 (17.8) | 2 (4.4) | 0 (0.0) | |||
| R4 | 57 (22.1) | 26 (25.2) | 18 (17.8) | 11 (24.4) | 2 (22.2) | |||
| R5 | 157 (60.9) | 60 (58.3) | 61 (60.4) | 29 (64.4) | 7 (77.8) | |||
| Avoid using public utilities | R1 | 6 (2.3) | 3 (2.9) | 3 (3.0) | 0 (0.0) | 0 (0.0) | 6.294 | 0.901 |
| R2 | 6 (2.3) | 3 (2.9) | 2 (2.0) | 1 (2.2) | 0 (0.0) | |||
| R3 | 36 (14.0) | 14 (13.6) | 16 (15.8) | 6 (13.3) | 0 (0.0) | |||
| R4 | 49 (19.0) | 19 (18.4) | 21 (20.8) | 6 (13.3) | 3 (33.3) | |||
| R5 | 161 (62.4) | 64 (62.1) | 59 (58.4) | 32 (71.1) | 6 (66.7) | |||
| Compliance with standard precautions | R1 | 9 (3.5) | 5 (4.9) | 3 (3.0) | 1 (2.2) | 0 (0.0%) | 25.972 | 0.011* |
| R2 | 8 (3.1) | 4 (3.9) | 1 (1.0) | 1 (2.2) | 2 (22.2) | |||
| R3 | 35 (13.6) | 17 (16.5) | 10 (9.9) | 7 (15.6) | 1 (11.1) | |||
| R4 | 77 (29.8) | 34 (33.0) | 36 (35.6) | 6 (13.3) | 1 (11.1) | |||
| R5 | 129 (50.0) | 43 (41.7) | 51 (50.5) | 30 (66.7) | 5 (55.6) | |||
(**) Highly significant P≤ 0.001, (*) Significant P< 0.05.
3.5. Subjective Worries Regarding the Dental Profession and its Association to Level of Anxiety
The mean rate of worries reported was 7.67 ± 1.91 on a scale from 1 to 10 (where 1 is not worried at all and 10 is extremely worried) regarding contracting COVID-19. Table 3 shows that a higher percentage of students (53.9%) disagreed with the idea that they would not be able to perform their job to the best of their ability post COVID-19, with a highly significant association with the level of anxiety (P = 0.001). Correspondingly, 69.0% of students do not wish to change their profession if given a chance, and this was significantly associated with the anxiety level (0.011). Moreover, there was a highly significant association between the level of anxiety and response of students to their need for extra precautions during dental training, even after the number of COVID-19 cases declined (P = 0.001).
3.6. Association Between the Possible Intention to Choose Another Profession and Gender and Level of Study
The results of this study showed a highly significant difference between both genders regarding their intention to change their dental profession (P = 0.001), with a higher percentage among male students (63.8%). On the other hand, there was a non-significant difference among students in different study levels for their possible intention to choose another profession (Table 4).
| Subjective Worries Questions |
Total n. (%) |
Anxiety level | Chi-square | |||||
|
None/ Minimal n. (%) |
Mild n. (%) |
Moderate n. (%) |
Severe n. (%) |
X2 | P-value | |||
| Will your profession be risky post COVID-19? | Yes | 211 (81.8) | 79 (76.7) | 87 (86.1) | 37 (82.2) | 8 (88.9) | 3.384 | 0.336 |
| No | 47 (18.2) | 24 (23.3) | 14 (13.9) | 8 (17.8) | 1(11.1) | |||
| Will your ability to perform your job to the best, be jeopardized post COVID-19? | Yes | 119 (46.1) | 28 (27.2) | 52 (51.5) | 33 (73.3) | 6 (66.7) | 30.971 | 0.001** |
| No | 139 (53.9) | 75 (72.8) | 49 (48.5) | 12 (26.7) | 3 (33.3) | |||
| Would you choose another profession if given a chance? | Yes | 80 (31.0) | 21 (20.4) | 35 (34.7) | 21 (46.7) | 3 (33.3) | 11.238 | 0.011* |
| No | 178 (69.0) | 82 (79.6) | 66 (65.3) | 24 (53.3) | 6 (66.7) | |||
| Do you prefer to postpone your training until COVID-19 cases decline/ vaccine is available? | Yes | 193 (74.8) | 69 (67.0) | 79 (78.2) | 37 (82.2) | 8 (88.9) | 6.223 | 0.101 |
| No | 65 (25.2) | 34 (33.0) | 22 (21.8) | 8 (17.8) | 1 (11.1) | |||
| Will there be a need for extra precautions in clinical training after COVID-19 cases decline? | Yes | 217 (84.1) | 76 (73.8) | 91(90.1) | 41 (91.1) | 9 (100.0) | 14.274 | 0.003* |
| No | 41 (15.9) | 27 (26.2) | 10 (9.9) | 4 (8.9) | 0 (.0) | |||
| Variables | Would you choose another profession if given a chance? | Chi-square | |||
| Yes (n = 80) | No (n = 178) | X2 | P-value | ||
| Gender | Male | 51 (63.8%) | 53 (29.8%) | 26.478 | 0.001** |
| Female | 29 (36.3%) | 125 (70.2%) | |||
| Level of study | 3rd | 16 (20.0%) | 37 (20.8%) | 4.727 | 0.316 |
| 4th | 12 (15.0%) | 33 (18.5%) | |||
| 5th | 21 (26.3%) | 28 (15.7%) | |||
| 6th | 15 (18.8%) | 32 (18.0%) | |||
| Dental Interns | 16 (20.0%) | 48 (27.0%) | |||
4. DISCUSSION
Stress is a general response or reaction of a person to a difficult physical or psychological situation. It could predispose anxiety, which has a negative impact on mental and physical health, with a sense of uncontrollability and unpredictability over potentially unpleasant life events [16, 17]. Undergraduate dental education is usually considered a stressful environment, and one of the reported stressors facing dental students is the fear of infection, which can lead to clinical anxiety [18, 19]. The hypothesis tested here was that dental students would have elevated stress and anxiety during the COVID-19 outbreak, which may have an impact on personal hygiene behaviors and social habits as well as subjective worries about the dental profession.
In this study, the mean total GAD-7 score reflects that the majority of students have mild anxiety, while a few percentages of them have moderate to severe anxiety. The same anxiety scale (GAD-7) was used to assess anxiety during the COVID-19 pandemic among dental students in the United Arab Emirates and reported a higher percentage of moderate to severe anxiety levels in almost half of their students [14]. However, much lower percentages of moderate (2.7%) to severe anxiety (0.9%) were found in medical students in China [13]. The percentages were nearly the same among dental practitioners in Italy, whether in the mean GAD-7 score (6.56) or in the recorded levels of moderate (15.2%) and severe (8.7%) anxiety [20]. On the other hand, using other scales for psychological distress, such as Kessler’s K6, on dentists and dental hygienists in Israel found that 11.5% of their study sample reported distress due to COVID-19 [21]. A self-designed questionnaire, which included a section focused on the fear of getting infected with COVID-19, was given to dentists from 30 countries with 50% of participants from Pakistan, Saudi Arabia, and the United Arab Emirates, and concluded that more than two-thirds of the general dental practitioners (78%) were anxious and scared [22].
According to study levels, the present work showed a non-significant difference in anxiety levels among students in different grades, with no students reported severe anxiety in the 3rd year. This could be attributed to their theoretical study and lack of experience in facing infected patients in clinical situations and being less acquainted with the clinic environment. A higher percentage of females reported anxiety in comparison to males, with a non-significant difference between both genders. This could be explained by the higher number of females participating in the study (154 vs. 104 males) as well as the assumption of Muhammad and Rajan (2020) that “females are more prone to get emotional and neurotic problems because of their metacognitive beliefs and thought control strategies” [23]. However, the response of any person to a potential stressor could be changeable according to their personality make-up [24].
With regards to changes in personal hygiene and social habits in response to COVID-19, students in the present study reported that they were changed with moderate to great levels and significant association between a change in behavior of buying more sanitizers as well as a change in standard precautions with anxiety level was reported. The study by Saddik et al. [14] on 719 medical and 323 dental students reported an increase in hand hygiene (46.7%) compliance to standard precautions (29.3%), an increase in the use of hand sanitizers (60.6%), a decrease in social visits (34.8%), a decrease in handshaking (27.5%), and a decrease in the use of public facilities (39%) [14]. This difference in the percentage of change could be attributed to the higher total number of students in their study and the involvement of medical students in addition to dental students.
Most students reported that the information they received about COVID-19 during the outbreak ranged from good to excellent. The Saudi Ministry of Health (MOH) was the main source of information for the greatest percentage of them, followed by social media. The least number of students got their information from college and university announcements. In comparison, Saddik et al. [14] reported social media as the main source of information for 46.7% of their medical/dental study group, with the second source the Ministry of Health (39.8%), while 31.3% got their information from university announcements [14]. Reporting the MOH as the main source of information in the present study could be explained by the daily messages sent to all cell phones with information about modes of infection, warnings, and preventive measures against COVID-19.
Owing to the high likelihood of dental healthcare providers acquiring infections during dental practice, the dental profession has been considered a hazardous job [18]. This hazard is expected to increase among undergraduate students because of early exposure to patients in dental clinics while training in practical sessions with the possibility of exposure to many respiratory viruses [14]. This expectation tends to be more during the COVID-19 pandemic, as confirmed by the high percentages of students who agreed that the dental profession would be more risky post COVID-19.
A large percentage of participants in the present study agreed that their job performance will not be to the best of their ability and that they have the possible intention to choose another profession; these are both alarming responses. These results are consistent with the conclusions of a study in Italy that found anxiety from COVID-19 might prevent a new generation of dental practitioners from entering the practice [20]. In that study, 74.4% of the respondents mentioned that COVID-19 had a highly negative impact on their professional activity and that most of them (89.6%) were quite concerned about their professional future, mostly due to the uncertainty about the end of the emergency situation.
Most students in the present work, whatever their level of anxiety, thought that they would prefer to postpone their training until COVID-19 cases decline or a vaccine is available, while there was a highly significant association between level of anxiety and response of students to their need to extra precautions on dental training even after the number of COVID-19 cases declines. These results are in accordance with a previous study by Ahmed et al. where 66% of their study participants agreed to close their dental practice until the number of COVID-19 cases starts to decline [22]. Similarly, Consolo et al. reported that one-third of their study participants were concerned by the need for further devices and adequate new clinical guidelines to overcome the spread of COVID-19 in the near future [20].
Although there was a non-significant difference between students in different study levels and their possible intention to choose another profession, the highest percentages were mentioned for the fifth-grade students and interns. The possible explanation of higher percentages among students in the fifth grade is that they have already passed one year of clinical training and patient contact and they were on the way to transitioning to a greater clinical contact in advanced dental driplines, while interns are on the way to be licensed for actual clinical practice without supervision.
The higher percentage of possible intention to change profession among male students (63.8%) in the present study highly recommends providing counselling services and psychological support with continuous monitoring of stress level to this recognized group. Moreover, as mentioned by Bhanushali et al. [24], Ghai [26], and Varalakshmi et al. [27], the college should urge faculty members to engage the students academically through online courses for the benefit of their career. Additionally, they recommended helping students to attend webinars about COVID-19 and its risk of infection in dental practice, aiming to understand the importance of its preventive guidelines’ implementation.
CONCLUSION
In conclusion, COVID-19 created some degree of anxiety among dental students at Umm Al-Qura University, ranging from mild to severe. This anxiety was higher in females with a non-significant difference between students in different grades. A high percentage of participating students reported changes in their personal hygiene and social habits with subjective worries regarding the dental profession, where one-third of them agreed that they would change their profession if they had the chance. Therefore, efforts should be made to minimize student anxiety in colleges through counselling and creating a supportive learning environment. In addition, dental schools should adequately prepare to face outbreaks of COVID-19 and other emerging infectious diseases with the latest updated information about its modes of infection and preventive measures.
The present study has some limitations, such as being confined to a single dental college, and consequently, the results may not be applicable to other parts of Saudi Arabia. Other COVID-19-related stressors, such as economic stressors, effects on daily-life, and academic delays, were not addressed. Thus, further study on a larger cohort of dental students is recommended, together with investigations of other factors that could lead to stress and anxiety during the COVID-19 pandemic.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study received ethical approval from the Institutional Review Board (IRB) at the College of Dentistry, Umm Al-Qura University, Saudi Arabia (IRB No. 175-2).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All participants in the study agreed on study publication by answering the study questionnaire.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [I,K,A], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank Professor Omayma Afifi for her help with statistical analysis.

