All published articles of this journal are available on ScienceDirect.

Effect of Duration of Use of a Toothbrush on its Filament’s Tapering and Plaque Removal Efficacy
Authors Info & Affiliations
Abstract
Background and Objectives:
Dental professionals often recommend changing toothbrushes every three months due to their wear and decreased plaque removal efficacy. This study aimed to assess the correlation of duration of use of a toothbrush and its wear and then the relationship of wear of toothbrush and Plaque Index (PI) of users and tapering of toothbrush filaments after three months of use was evaluated as well.
Materials and Methods:
In this study, 60 female students were enrolled according to the eligibility criteria and received a new set of toothbrush and toothpaste. They were requested to brush their teeth using the Bass technique twice a day for 2 minutes and the Ramfjord PI was measured at baseline and after 3 months. The wear of 47 toothbrushes after three months of use was evaluated using the Rawls index. Of collected 47 toothbrushes, 30 were randomly chosen and inspected under an electron microscope to determine the degree of tapering of bristles. Data were analyzed using SPSS version 20 via Spearman’s correlation coefficient, paired t-test and Pearson’s correlation coefficient (alpha=0.05).
Results:
After 3 months, the mean PI score significantly decreased (paired t-test, P=0.034). The PI at 3 months after use had no significant correlation with the toothbrush wear score (Spearman’s correlation coefficient, P=0.61) but the toothbrush wear score had a significant correlation with tapering of bristles (Spearman’s correlation coefficient, P=0.04). No significant association existed between PI at 3 months after use and tapering of bristles (Pearson’s correlation coefficient, P=0.69).
Conclusion:
The duration of use and wear of toothbrush alone do not affect the quality of plaque removal. Practicing Oral hygiene can affect the quality of plaque removal.
1. INTRODUCTION
Supragingival plaque removal is among the most important strategies to promote oral and dental health and decrease the prevalence of caries (especially in combination with the use of fluoridated toothpastes) and periodontal disease [1, 2]. Several methods are available for mechanical and chemical plaque removal. But, mechanical plaque removal by toothbrushing is the most commonly practiced technique of oral hygiene [3, 4]; therefore, it is important to assess the efficacy of this method [5].
In general, it is recommended to replace toothbrushes before the appearance of the first signs of wear of filaments, which often occurs 2-3 months after using the toothbrush. However, not all patients follow this recommendation and evidence shows that the mean age of a toothbrush is 2.5 to 6 months at the time of replacement [6].
Dental professionals and dental product manufacturers also recommend changing the toothbrushes every 3 months [4, 7]. A question arises whether there is a scientific basis for this recommendation or it is just a matter of profitability by increasing the sale [7]. The recommended time for toothbrush replacement may vary among different individuals depending on the amount of force applied during toothbrushing, technique and duration of toothbrushing and socioeconomic factors [8]. Also, toothbrush replacement in short time periods can be costly in underdeveloped countries; in these countries, greater attention must be paid to affordable preventive programs [9]. Despite the extensive use of toothbrushes, limited published data are available supporting the replacement of toothbrushes after several months [10, 11]. Some studies have recommended changing the toothbrush after 2, 5 or 6 months [11].
The American Dental Association emphasizes on replacement of toothbrushes every 3-4 months for maximum plaque removal. Studies conducted in Australia and the United States show that most dentists recommend their patients to change their toothbrush every 2-3 months [4, 7, 12]. Most studies have evaluated the wear of toothbrushes after 3 months of use [7,11,13-16].
Several authors stated that no difference exists in plaque removal between new and old toothbrushes [3,7,9,13,14,17-20]. In contrast, other authors showed a significant difference in plaque removal efficacy of old and new toothbrushes [11,15,16,21,22]. Kreifldt et al . [6] in 1980 studied the tapering of toothbrush filaments and showed that new toothbrushes were more effective than old toothbrushes in dental plaque removal. They evaluated the worn toothbrushes and noticed that following wear, the filaments become tapered and this tapering continues from the tip to the end of the filament. For instance, filaments are tapered from 0.28 mm at one end to 0.015 to 0.020 mm at their free end. They concluded that among different wear factors, tapering has a greater effect on decreasing the efficacy of toothbrushes for plaque removal. They explained that tapering decreases the diameter of filaments and thus, the toothbrush becomes softer and removes less amount of plaque [6].
Considering the controversial results regarding the appropriate time of changing the toothbrush, the primary objective of this study was to assess the correlation of duration of use of a toothbrush and its wear and the second objective was to determine the relationship of the wear of toothbrush and plaque index (PI) of users and tapering of toothbrush filaments after three months of use.
The null hypothesis of this study is that the duration of use and wear of toothbrush do not affect the plaque removal efficacy.
2. MATERIALS AND METHODS
This was a double-blind descriptive clinical trial and included a prospective experimental design. This study was conducted on female non-medical students staying at Isfahan University dormitories. The sample size involved 60 individuals. With this sample size, the correlation coefficient more than 0.37 between the duration of use of toothbrush and the wear rate was significant with a probability of 0.80 (α = 0.05). But after 3 months, 13 students were excluded due to reasons not related to this study.
Two examiners presented to the student rooms in the dormitories one by one. The students were briefed about the study and were requested to fill out the questionnaire. Afterwards, they underwent a clinical oral examination by the first examiner. The age range of candidates was 18 to 37 years. They all reported toothbrushing twice a day, each time for approximately 2 minutes. Also, an intraoral clinical examination revealed that they all had the 6 Ramfjord teeth (16,21,24,36,41,44). They did not use dental floss or mouthwash and had no systemic disease. They did not have gingival recession, prosthetic crowns or class V caries in the respective teeth. They did not have a removable denture or orthodontic brackets either [16]. They signed informed consent forms prior to participation in the study. The Bass technique of toothbrushing was instructed to them again and they were provided with a new set of toothbrush (Morvarid PanbehRiz, Boushehr, Iran) and fluoridated toothpaste (Nasim, Goltash, Isfahan, Iran). They were requested to brush their teeth for 2 minutes with their new toothbrush and toothpaste according to the Bass technique. The PI was then measured by the first examiner using the Ramfjord PI [23] such that the students were requested to chew a disclosing tablet (Seveneska; Dentaurum, Sweden) and the interproximal, facial and lingual surfaces of the respective teeth were scored from 0 to 3 [22]. Eventually, the students were requested to brush their teeth twice a day each time for 2 minutes for 3 months using the new set of toothbrush and toothpaste according to the Bass technique. After 3 months, they were clinically examined again to make sure they do not possess any of the exclusion criteria; 13 students were excluded due to reasons not related to this study. The remaining students were requested to brush their teeth for 2 minutes using the Bass technique and then the first examiner measured the Ramfjord PI as explained earlier. The toothbrushes were then collected by the second examiner. The wear of toothbrushes used for 3 months was then evaluated according to the Rawls index (fraying and separation of filaments) [22]. According to this index:
Score 0: Cannot determine whether the toothbrush has been ever used or not.
Score I: Bristles of some of the tufts are separated.
Score II: Bristles of most of the tufts are separated and some tufts are covered with other bristles and some bristles were angled.
Score III: Most tufts are covered with other bristles and bristles have a sharp tip and are bent (Fig. 1).
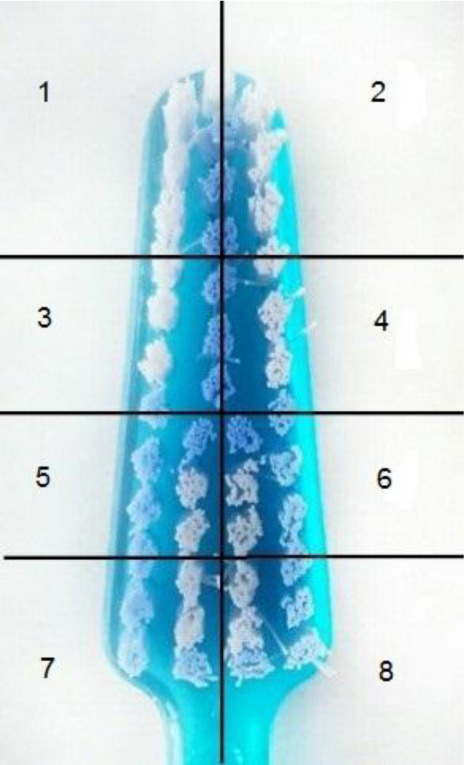
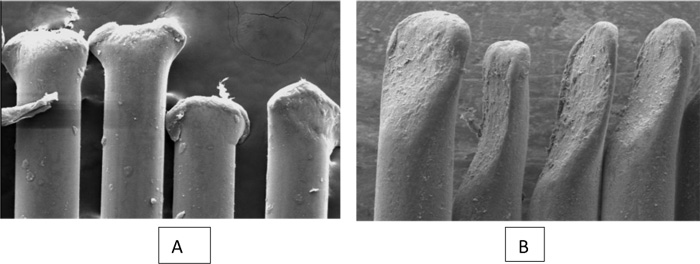
According to the Rawls index, scores 0 and I are acceptable for a toothbrush and indicate that the toothbrush is capable of maximum plaque removal. Scores 2 and 3 indicate that the toothbrush is not capable of maximum plaque removal. Two examiners independently inspected the toothbrushes and scored them. In case of the presence of a difference between the scores, they inspected the toothbrush together to reach one final score that both agreed on [8]. Of 47 toothbrushes evaluated, 30 were randomly selected by draw (as explained earlier) and the head of each toothbrush was divided into 8 equal areas and coded from 1 to 8 (Fig. 2). Two areas were selected among the 8 by draw and the tufts present in these two areas were coded by numbers (separately for each area). Eventually, one tuft was randomly chosen from each area by draw (2 tufts from 2 areas of the toothbrush head). Four bristles of the 2 selected tufts (a total of 8 bristles from each toothbrush head) were chosen and cut [24]. Bristles were cut from the end and mounted horizontally on an aluminum foil next to each other. Eight bristles of a new toothbrush were also cut and used as a standard reference. In the next phase, bristles were gold-coated for scanning electron microscopy (SEM) assessment. Of the selected 8 bristles, 3 to 4 photographs were taken at x100 magnification (Fig. 3). Using Image J software, the diameter of the tip (endpoint of the bristle head) and the basis of all 8 bristles of each toothbrush were measured in microns (µ). The difference between the diameter of basis and tip was calculated and the mean value for all 8 bristles of each toothbrush was separately calculated and compared with that of a new toothbrush. Data were analyzed using SPSS version 20 via Spearman’s correlation coefficient, paired t-test and Pearson’s correlation coefficient (alpha=0.05). Spearman’s correlation coefficient was used to evaluate the relationship between a quantitative variable (tapering) and a ranking variable (wear score). Pearson’s correlation coefficient was used to evaluate the relationship between two quantitative variables (tapering and PI).

3. RESULTS
A total of 60 female students with a mean age of 21.4±3.2 years (range 18 to 37 years) were evaluated. In our study according to Rawls index, score 0 was noted in 13 (27.7%), score 1 was noted in 24 (51.1%), score 2 was noted in 7 (14.9%) and score 3 was noted in 3 (6.4%) toothbrushes. The toothbrush wear score was less than 2 in the majority of toothbrushes (78.8%). The Wilcoxon test showed a significant difference between the toothbrush wear scores at baseline and after 3 months (P<0.001) and the wear of toothbrush significantly increased after 3 months of use.
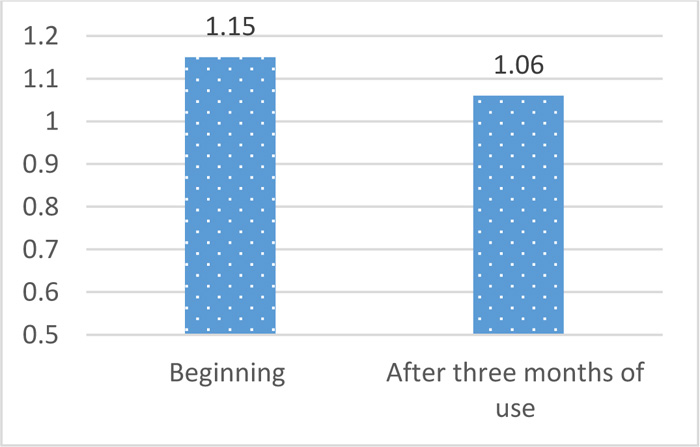
Paired t-test showed that the Mean plaque index significantly decreased after three months (P=0.034) (Table 1 and Fig. 4).
| Variable | Time | Mean (standard deviation) | P- value |
|---|---|---|---|
| Plaque index | Beginning | 1.15 (0.47) | 0.034 |
| After three months of use | 1.06 (0.39) |
One-sample t-test showed a significant difference between the mean diameter of bristles of a new toothbrush (-43.57) and the mean diameter of bristles of the 30 used toothbrushes (100.98±25.87) after 3 months, and significant tapering occurred during this time period (P<0.001).
The Spearman’s correlation coefficient showed that the PI at 3 months after using the toothbrush had no significant correlation with toothbrush wear (P=0.61). But toothbrush wear had a significant correlation with tapering (P=0.04). The Pearson’s correlation coefficient found no significant correlation between PI at 3 months after using the toothbrush and tapering (P=0.69). (Table 2).
4. DISCUSSION
Regular plaque removal from all dental surfaces is imperative for adequate oral hygiene, and manual toothbrushing is an efficient tool for plaque removal [11]. According to the general belief, toothbrushes should be regularly replaced since old toothbrushes are no longer capable of efficient dental plaque removal [7, 16]. This can be due to tapering of the tip of bristles and their consequently decreased diameter. As a result, the toothbrush becomes softer and can eliminate lower amounts of plaque [6]. According to some studies, the plaque removal efficacy of toothbrushes depends on factors such as the distribution of bristles, their separation and tapering. Clearly, bristles are separated during toothbrushing to cover and clean a larger surface and increase the efficacy of cleaning [11]. Differences in the area covered by toothbrush bristles can be due to factors such as the load applied during toothbrushing and the technique of toothbrushing [3, 13, 14, 19-21]. For instance, patients who brush their teeth with excessive force have greater toothbrush wear [3]. Other factors playing a role in this respect include individual differences in shape and size of the dental arch, size of teeth and shape and sharpness of cusps. Habits such as chewing the head of the toothbrush during toothbrushing is another important factor in this respect [14]. The purpose of this study was to assess the changes in toothbrush wear, dental plaque and tapering of bristles 3 months after using the toothbrushes and to evaluate the correlation among these three variables. The plaque removal efficacy of a new toothbrush was also compared with that of toothbrushes used for 3 months. The results showed a significant difference between the toothbrush wear scores at the beginning of the study and after 3 months of using the toothbrush, and the wear significantly increased at 3 months, which is obvious since by using the toothbrush, bristles are gradually frayed.
At 3 months, 78.8% of toothbrushes showed scores 0 and 1 and 21.2% had scores 2 and 3. This finding indicates that individuals who receive adequate oral hygiene instruction (Bass technique) apply standard force during toothbrushing; therefore, toothbrush wear and separation of bristles less commonly occur. Since toothbrush wear can significantly affect dental plaque accumulation, it seems imperative to assess the effect of toothbrush wear on plaque control quality. In this study, the mean PI significantly decreased at 3 months after toothbrushing (Table 1 and Fig. 4). The PI score is expected to increase following 3 months of wear of toothbrush but it may not be the case in all individuals, and a person with a high toothbrush wear score may show a low PI score. One reason may be the effect of oral hygiene instruction and correct toothbrushing on dental plaque. In our study, oral hygiene instruction had a superior effect compared to toothbrush wear on the reduction of microbial plaque. Also, it may take some time until the individuals get used to the new method of toothbrushing and may not be able to correctly brush their teeth at the beginning of the study. Resultantly, the plaque may not be completely removed and the PI score may be higher at the onset of the study. Another reason explaining the improvement in PI score may be the motivation of individuals for participation in the study (the Hawthorne effect) [3, 14, 20], which may positively affect the oral hygiene. Thus, in our study, the duration of the use of toothbrush alone did not affect the quality of plaque removal. Oral hygiene and microbial plaque control are among the most important factors with regard to oral and dental health. Oral hygiene instruction must be taken into account in all dental procedures and is imperative for the primary prevention of gingivitis [6].
| Variable | Toothbrush Wear Score | Plaque Index at 3 Months After Using the Toothbrush | ||
|---|---|---|---|---|
| R | P | R | P | |
| Toothbrush wear score | 1 | - | -0.076 | 0.61 |
| Plaque index at 3 months after using the toothbrush | -0.076 | 0.61 | 1 | - |
| Tapering | 0.250 | 0.04 | 0.075 | 0.69 |
The PI at 3 months after the use of toothbrush had no significant association with toothbrush wear. The current results showed that dental plaque removal did not correlate with the duration of the use of toothbrush, at least within 12 weeks. This finding was in line with the results of studies conducted by Daly (1996), Sforza (2000), Tan and Daly (2002), Van Palenstein Helderman (2006) and Pochapski (2011) stating that the efficacy of plaque removal does not correlate with age and wear of toothbrush [3, 13, 14, 17, 20].
Daly et al., in 1996, evaluated the effect of toothbrush wear on plaque control and found that significant toothbrush wear did not decrease the efficacy of plaque removal. They stated that the improvement in plaque score can be due to the motivation of individuals towards participation in the study. Thus, toothbrush wear does not necessarily refer to inadequate plaque control [20]. Rosema et al., in 2013, evaluated plaque removal by new and old toothbrushes (used for 3 months) and found no significant difference between them. They stated that the wear of bristles is a more important factor than the duration of use of toothbrush in plaque removal [7].
In contrast, Nam in 2005 showed that a new toothbrush is superior to a worn toothbrush in plaque removal by 15.1% in the entire mouth, 20.6% in proximal areas and 16.3% in marginal areas [16]. Pradeep S Tangade et al., in 2013, evaluated the correlation of plaque removal and separation of bristles and found a higher PI score in the group that used an old toothbrush. They concluded that PI score increases by an increase in flaring of bristles [11].
Differences among the studies regarding the correct time of replacing a toothbrush can be attributed to variables such as type of toothbrush, type of toothpaste, methods used for calculation of PI, difference in the number of examined teeth and areas, method of assessment of wear, duration of study and the study population.
Kreifldt et al. showed that new toothbrushes were significantly more effective than old toothbrushes in removal of dental plaque. They evaluated the worn toothbrushes and noticed that following wear, filaments became tapered and the tapering continued from the tip to the end of the filament. For instance, filaments were tapered from 0.28 mm diameter at the end to 0.015-0.020 mm at the free end. They concluded that among the wear factors, tapering had a greater effect on decreasing the efficacy of toothbrushing. They interpreted that due to tapering, the diameter of filaments decreases, the toothbrush becomes softer and consequently removes less amount of plaque. Eventually, they concluded that toothbrushes should be regularly replaced [6]. The current study evaluated the tapering of bristles. A significant difference was noted in the mean diameter of bristles of a new toothbrush and the mean diameter of bristles of the 30 toothbrushes used for 3 months. In other words, the mean diameter of bristles of toothbrushes used for 3 months was significantly smaller and more tapered compared to the bristles of a new toothbrush. The tapering of bristles had a direct correlation with the toothbrush wear scores and by an increase in toothbrush wear scores, the tapering increased as well (Table 2). However, the PI at 3 months after using the toothbrush had no significant correlation with tapering (Table 2). As mentioned earlier, the greatest confounder in decreasing the efficacy of toothbrushing and consequently increasing the PI was a reduction in bristle diameter and tapering; whereas, in our study, PI decreased and the reason was believed to be the dominant effect of oral hygiene instruction compared to tapering and decreased diameter of bristles in the reduction of PI.
CONCLUSION
Toothbrush wear is not necessarily correlated with the age of toothbrush and can be due to other factors such as the amount of load applied, method and duration of toothbrushing and socioeconomic factors. Duration of use and wear of toothbrush do not affect the quality of plaque removal alone. Proper oral hygiene instruction and correct method of toothbrushing are more important parameters in this respect. Thus, oral hygiene instruction is an important factor for oral health promotion, which should be addressed by dental clinicians at all times. Also, as the result of instruction of oral hygiene and correct method of toothbrushing, individuals brush their teeth with optimal force and decrease the toothbrush wear score as such. Although the tapering of bristles had a high frequency in our study, it had no correlation with PI. This finding may highlight the role of oral hygiene instruction in plaque removal.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study has been approved by the Ethics Committee of Isfahan University , Iran with approval no IR.MUI.REC.1395.3.921
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from each participant prior to the study.
STANDARD OF REPORTING
CONSORT guidelines and methodology were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that supports the findings of this study is available at http://s12.picofile.com/file/8400298492/data2.sav.html.
FUNDING
None.
ACKNOWLEDGEMENTS
The authors would like to thank Mr. Rahimzadeh for his assistance in electron microscopic analysis.

