All published articles of this journal are available on ScienceDirect.

Incidental Findings in Temporomandibular Joint Region Detected by Cone-beam Computed Tomography: A Retrospective Study
Abstract
Purpose:
The purpose of this study was to investigate the prevalence of Incidental Findings (IFs) in the temporomandibular joint (TMJ) region detected in Cone-Beam Computed Tomography (CBCT) scans of maxilla and mandible.
Materials and Methods:
In this study, 384 CBCT scans were reviewed for IFs of the TMJ region. Demographic data including age and sex were recorded. The scans were evaluated in multiplanar views: corrected sagittal, corrected coronal and axial sections. IFs in TMJ region were categorized into eight groups: osteoarthritis, flattening and erosion of condyle and articular eminence, osteophytes, subchondral pseudocyst, condyle hyperplasia, condyle hypoplasia, bifid condyle, and soft tissue calcification. Statistical analyses were performed using the SPSS statistic v.22.
Results:
From the CBCT scans, a total of 81 (21.1%) IFs were identified. 184 of the subjects (47.9%) were male and 200 (52.1%) were females. Their age ranged from 10 to 75 years old with a mean of 36.8 and a standard deviation of 13.9 years. The most frequent IFs were flattening and erosion of condyle and articular eminence (40.74%), followed by soft tissue calcification (30.86%). Osteoarthritis was not observed in any of the subjects. There was no significant difference between females and males in IFs of TMJ joint and its related structures. Flattening and erosion of condyle and articular eminence, soft tissue calcification, osteophytes and, subchondral pseudo cyst showed significant differences between individuals of different age ranges.
Conclusion:
While examining CBCT images, it is critical to check for evidence of IFs in the TMJ region. The findings of this study emphasize the value of a thorough examination of all areas visualized on CBCT scans even those beyond the region of interest.
1. INTRODUCTION
Incidental Findings (IFs) are defined in the literature as any findings on a radiographic image which are not related to the areas of research interest or the purpose for which the image was taken. A better understanding of IFs and improved knowledge of head and neck anatomy will allow clinicians to avoid misinterpretations of these images. The guidelines of the American and European Academies of Dentomaxillofacial Radiology also recommend the evaluation of all structures in a clinical examination. Therefore, a good knowledge of the dentomaxillary complex and the adjacent structures are required as part of a systematic examination.
IFs are asymptomatic and also common in TMJ images. Most IFs such as anatomical variations are asymptomatic and require no intervention; however, correct identification of these findings simplifies diagnostic assessments and warrant appropriate treatment plans.
Conventional imaging modalities are generally used in dental practice routine. They provide valuable information about the dentomaxillofacial region, but they suffer from limitations such as superimpositions, magnifications, distortions, and low-image quality [1]. During the past decades, the use of Cone-beam Computed Tomography (CBCT) imaging in dentistry has been on the rise. It offers advantages over conventional or medical computed tomography in that it can produce an excellent high spatial resolution, and the radiation dose is markedly lower [2]. CBCT imaging has been applied in implantology, orthodontics, maxillofacial surgery and in the assessment of dentoalveolar pathology by providing three-dimension images [3].
The images obtained on a CBCT scanner with a small field of view (FOV) are used for examining limited areas of the maxillofacial region, but a larger FOV image covers the paranasal sinuses, temporomandibular joint, airways and intracranial and cranial base structures [4]. The TMJ is one of the most important joints in the body, and it is in harmony with the oral cavity and teeth. Radiographical examination of TMJ structures is very important for evaluating the abnormalities and bony changes that affect the TMJ [5]. There are several imaging modalities to visualize the TMJ: panoramic radiography, plain radiography, conventional and computed tomography (CT), cone-beam computed tomography (CBCT), arthrography and magnetic resonance imaging (MRI). Conventional radiography of TMJ such as transcranial, transpharyngeal, panoramic radiograph, conventional tomographic sections of TMJ may be adequate in some clinical situations. But there are bony alterations like erosions, osteophytes are difficult to detect in conventional radiographs due to the superimposition of the anatomic structures [6].
Osseous changes are best visualized in tomography and CBCT. Studies have reported high accuracy when using CBCT to evaluate the TMJ region. The superiority of CBCT for analyzing the TMJ region because of the absence of superimposition of anatomical structures [7].The presence of TMJ abnormalities play a critical role in treatment planning and are important to evaluate prior to commencing treatment.
Imaging of the TMJ is not always required for a diagnosis. Research has shown that the radiological findings of the TMJ do not always support the clinical findings. TMJ imaging should only be performed when it is known that it could contribute to a proper diagnosis and treatment with a better prognosis [8].
Accurate evaluation of CBCT scans may also reveal IFs that are unrelated to the current disease but are of clinical significance. It would also facilitate a comprehensive evaluation of underlying diseases by practitioners leading to life-saving interventions through early diagnosis. The purpose of this study was, therefore, to investigate the prevalence of IFs in the Temporomandibular Joint (TMJ) region detected in Cone-Beam Computed Tomography (CBCT) scans of maxilla and mandible.
2. MATERIALS AND METHODS
This study was performed using CBCT scans obtained between June 2017 and April 2019. The CBCT machine utilized was aGallileos unit (Sirona Dental System GmbH, Germany) with a 15*15 cm field of view, 85 kV, 28mAs, and 0.3 mm voxel size, VO1 resolution, effective dose for a full scan 67.52 ± 0.30. For Gallileos CBCT scans, volumes were viewed using the manufacturer's proprietary SidexisX-G software (Sirona Dental X-ray Systems Next Generation).
The study consisted of 384 patient CBCT scans that had been taken for other diagnostic purposes and were referred for CBCT evaluation to the Department of Oral and Maxillofacial Radiology, School of Dentistry, Isfahan, Iran. Ethics approval for the retrospective review was obtained from the Ethical Committee of Isfahan University of Medical Sciences, Faculty of Dentistry. The consent of the Imaging Center of Isfahan Dental School was sought for the use and sharing of scans information for educational and research purposes. Other licenses were obtained from competent authorities where required. All the collected data were only accessible to the researchers involved in this study. The information on the patients’ gender and age were also collected in this study.
Images with a full field of view (maxilla and mandible areas) that contained the TMJ region were only included in this study and those CBCT scans with only maxilla or only mandible images or with suboptimal quality were excluded.
The bone kernel was used in the CBCT reconstruction. To optimize the image presentation and facilitate the diagnosis, for each scan, the contrast/window and brightness/level parameters were adjust in to select the best possible images reproducing the bony structures of TMJ. The observers were permitted to scroll through axial, corrected sagittal and corrected coronal sections searching for the presence or absence of IFs in the TMJ region.
Images were viewed in a dimly lit room. Two radiologists with more than 10 years of clinical experience performed an analysis of the scans. First, radiologists examined 30 scans followed by a new assessment two weeks later. Finally, a second radiologist re-evaluated all the CBCT examinations. Where no conclusion could be drawn from an image, the opinion of other experienced radiologists was sought. All diagnoses were based on CBCT findings. Comparisons and associations with conventional radiography and histopathological examinations were not performed here.
A list containing the most cited IFs in the CBCT examination [6] was generated as guidance for the classification of images. Findings were categorized into eight groups: Osteoarthritis, Flattening and erosion of condyle and articular eminence, Osteophytes, Subchondral Pseudo cyst, Condylar hyperplasia, Condylar hypoplasia, Bifid condyle and Soft tissue calcification.
The sample size was selected by the statistical consultant. Statistical analyses were performed using the SPSS statistic v.22 package (IBM crop, formerly SPSS Inc, Chicago, USA) and Microsoft Excel 2013, based on 95% confidence and a margin error of 0.5%. The Chi-square test was used for comparisons. An intra-calibration and inter-calibration were performed through the Kappa test.
3. RESULTS
A total of 384 CBCT scans were assessed in this study; 200 of the subjects (52.1%) were female and 184 (47.9%) were male (Table 1). The patients mean age was 36.8±13.9 years and within a range of 10 to 75 years. Of the subjects, 131 (34.1%) were under 30 years of age, 174 (45.3%) were from 30 to 49 years old and 79 (20.6%) were 50 years and older. A total of 81 IFs, (21.1%) were discovered from the 384 maxilla and mandible CBCT scans.
| Gender | No. | % | Average age(year) | Standard deviation | Max. age(year) | Min. age(year) |
|---|---|---|---|---|---|---|
| Male | 184 | 47.9 | 44 | 11.2 | 75 | 13 |
| Female | 200 | 52.1 | 29.6 | 9.5 | 49 | 10 |
| Total | 384 | 100 | 36.8 | 13.9 | 75 | 10 |
The primary indications for CBCT scans in our study were implant and bone evaluation for implant (n = 228) and third molar surgery (n = 47). The least common CBCT indications were vertical root fracture and missing tooth. The indication for CBCT referral from the subjects is shown in Table 2.
| Indication for CBCT | No. |
|---|---|
| Implant/bone evaluation for implant | 228 |
| Trauma | 26 |
| Oral and maxillofacial lesion | 15 |
| Impaction localization | 21 |
| Third molar surgery | 47 |
| Orthodontic root resorption | 8 |
| Supernumerary tooth | 12 |
| Missing tooth | 7 |
| Vertical root fracture | 5 |
| Evaluation of graft | 15 |
| Total | 384 |
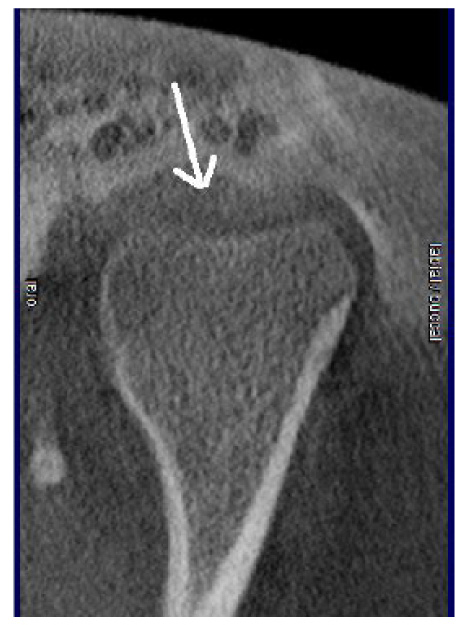
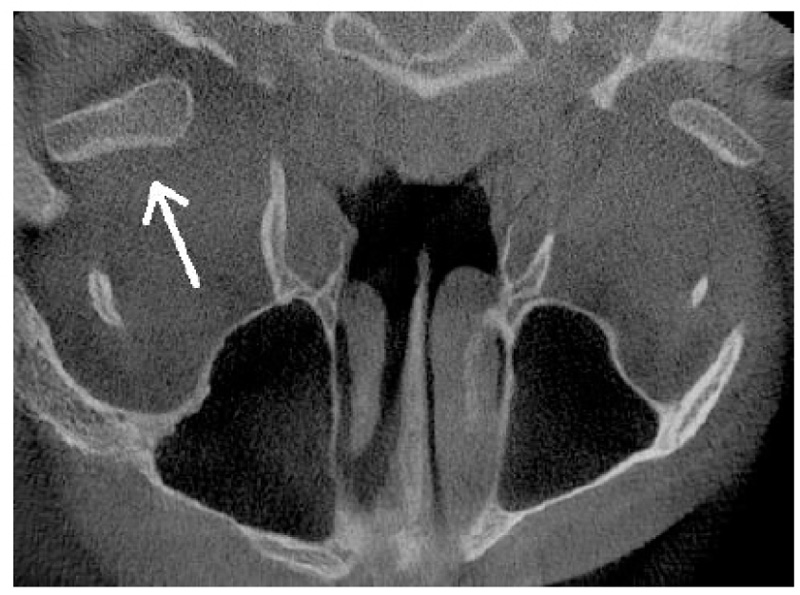
The number of IFs in TMJ including its related structures are shown in percentages in Table 3. The highest frequency (40.74%) was related to flattening and erosion of condyle and articular eminence (Fig. (1), followed by soft tissue calcification (30.86%), osteophytes (12.34%) (Fig. (2) , subchondral pseudo cyst (8.46%), condylar hypoplasia (3.75%), bifid condyle (2.64%) (Fig. (3) , and condylar hyperplasia (1.23%) (Fig. (4 ). Osteoarthritis was not observed in any of the subjects.
The gender distribution of IF in the TMJ area and related structures are shown in Table 4. Fisher exact test showed no significant difference between genders in flattening and erosion of condyle and articular eminence, osteophytes, and soft tissue calcification (p> 0.05). In addition, the Chi-square test showed that other IFs of TMJ joint and its related structures were not significantly different between sexes (p> 0.05).


| Categories | % of IF | No. of IF |
|---|---|---|
| Subchondral Pseudo cyst | 8.46 | 7 |
| Flattening and erosion of condyle and articular eminence | 40.74 | 33 |
| Osteophytes | 12.34 | 10 |
| Osteoarthrosis | 0 | 0 |
| Condylar hyperplasia | 1.23 | 1 |
| Condylar hypoplasia | 3.73 | 3 |
| Bifid condylar | 2.46 | 2 |
| Soft tissue calcification | 30.86 | 25 |
| Total | 100 | 81 |
Chi-square test showed a significant difference (p<0.001) between individuals of different age groups in frequency of flattening and erosion of condyle, articular eminence and soft tissue calcification Table 5. Chi-square test with the likelihood ratio did also show that the frequency of subchondral pseudo cyst (p= 0.04) and osteophyte (p= 0.002) was significantly different between different age groups, but not the frequency of condylar hyperplasia, condylar hypoplasia and bifid condyle (p> 0.05). IFs of TMJ region were mostly seen in over 30 years old. The only IFs seen in under 30 years old were flattening and erosion of condyle and articular eminence. The most frequent IF seen in over 30 years was flattening and erosion of condyle and articular eminence and soft tissue calcification. The prevalence of flattening and erosion of condyle and articular eminence was remarkably high in the over 50 year age group.
| Incidental finding | Female | Male | P-value | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Subchondral pseudo cyst | 3 | 3.70 | 4 | 4.94 | 0.45 |
| Flattening and erosion of condyle and articular eminence | 18 | 22.22 | 15 | 18.52 | 0.77 |
| Osteophytes | 3 | 3.70 | 7 | 8.64 | 0.14 |
| Condylar hyperplasia | 0 | 0.00 | 1 | 1.23 | 0.48 |
| Condylar hypoplasia | 1 | 1.23 | 2 | 2.47 | 0.47 |
| Bifid condylar | 0 | 0.00 | 2 | 2.47 | 0.23 |
| Soft tissue calcification | 13 | 16.05 | 12 | 14.81 | 0.99 |
4. DISCUSSION
In this study, 81 incidental findings in the TMJ region were documented. The most frequently IFs seen in the TMJ region, with flattening and erosion of condyle and articular eminence (40.74%).
| Incidental findings | Under 30 years | 30-49 years | 50 years or older | - | |||
|---|---|---|---|---|---|---|---|
| % | No. | % | No. | % | No. | p-value | |
| Subchondral pseudo cyst | 0.00 | 0 | 4.94 | 4 | 3.70 | 3 | 0.04 |
| Flattening and erosion ofcondyle and articular eminence | 2.47 | 2 | 11.11 | 9 | 27.16 | 22 | <0.001 |
| Osteophytes | 0.00 | 0 | 4.94 | 4 | 7.41 | 6 | 0.002 |
| Condylar hyperplasia | 0.00 | 0 | 1.23 | 1 | 0 | 0 | 0.45 |
| Condylar hypoplasia | 00.0 | 0 | 1.23 | 1 | 2.47 | 2 | 0.13 |
| Bifid condylar | 0.00 | 0 | 1.23 | 1 | 1.23 | 1 | 0.37 |
| Soft tissue calcification | 0.00 | 0 | 9.88 | 8 | 21.01 | 17 | <0.001 |
Different studies showed different results on the frequency of TMJ IFs. This difference may have been due to the superior reliability and greater accuracy of CBCT for analyzing the TMJ region because of the absence of superimposition of anatomical structures. In particular, panoramic imaging and conventional tomography may yield disappointing results [9]. In 2018 the study review of Rai et al, of 1500 patients, IFs were found in 89% of the subjects and the least IFs(0.4%)were related to the TMJ region [10]. However, in previous studies, findings in the TMJ region were recorded from 2.6% to 26.5% [11, 12]. In our study, the occurrence of IFs in the TMJ region was 21% (81 out of 384 subjects) with some patients having more than one IFs with the most IF being the flattening and erosion of condyle and articular eminence, similar to those reported by Nakata et al. (2006) [13] and Price et al. (2012) [14]. In the study by Çaglayan et al, in 2012, the highest rate of IFs in TMJ region was flattening and erosion of condyle and articular eminence (4.8%), followed by osteophyte (3.4%) and bifid condyle (2.9%) [15]. In a study done by Cha JY et al. (2007), IFs in the TMJ region were the second common finding (3.4%) [16]. In 2012, Allareddy et al. reported osteoarthritis as the most commonly IFs in the TMJ region [17] in contrast to the findings of this study, no osteoarthritis was observed in any of the subjects.
In our study, soft tissue calcification was the second most common finding in the TMJ region. In 2016, a study by Barghanet al. reported soft tissue calcification (29.71%) as the most common observed finding in TMJ region [18].
The prevalence of condylar bone changes in orthognathic surgery patients has been reported to be 55% by transpharyngeal radiographs [ 19 ] and 35.7% by CT [ 20 ]. Miloglu et al. [ 21 ] found the frequency of bifid mandibular condyle in a Turkish patient population to be 0.3% by panoramic radiography.
In the present study, the incidental findings of TMJ and its related structures were not significantly different between the two sexes (p> 0.05), but another study found that women were 2.58 times more likely to be found with osteoarthritis in TMJ scan studies [11].
Here, IFs of the TMJ region were mostly seen in over 30 years old and the prevalence of flattening and erosion of condyle and articular eminence was remarkably high in the over 50 age group. Patients aged 40-49 were also found in another study to have the highest percentage of reported IFs, in contrast to patients aged 20-29 [22]. The prevalence of flattening and erosion of condyle and articular eminence soft tissue calcification, subchondral pseudo cyst and osteophyte have been significantly varied between different age groups.
The reason for the reported low rate of TMJ erosion changes in orthodontic patients’studies [12] could be sampling bias as most samples were from young patients. Our study and those of others have shown that the TMJ changes increases with age [23]. Several studies have also shown that TMJ degenerative changes are higher among women [11, 24].
This study clearly showed variation IFs in the TMJ region. Several radiographic methods are used to assess the TMJ, an area that is difficult to be imaged due to factors like the superimposition of adjacent structures and morphological variations. This variability in the TMJ may be important can be an indicator of various TMJ diseases. Calcifications are one of these IFs and may be asymptomatic but common in TMJ images. Although most of the calcifications require no treatment, some findings including erosion of condyle and articular eminence, osteophytes, condylar hyperplasia, condylar hypoplasia can further mimic signs and symptoms of TMJ disorders.
The initial detection of morphological changes of the TMJ is often difficult to identify because an initial clinical diagnosis is routinely based on suspicion, rather than any visual degenerative signs. Evaluating the TMJ area in the CBCT scans taken for another reason could early detect changes in the TMJ region. Osseous changes are best visualized in tomography for analyzing the TMJ region because of the absence of superimposition of anatomical structures
Taken together, IFs in the TMJ area may present no clinical symptoms or functional impairment which require medical intervention, however, some IFs may influence the treatment plan. Diagnosis and early treatment of such pathological lesions and injuries, in the TMJ region, can reduce the treatment time and cost. Our results hence reinforce the need for dental professionals to be aware of the IFs and variations in normal anatomy.
One limitation of our study is that the process is limited to two maxillofacial radiologists. The maximum age of the females was much less than the males because we used CBCTs scans within a specified timespan. We recommend that further studies be carried out on a larger sample and on genders in the same age deviation, and more radiologists perform the analysis. The other limitation was the categories of incidental findings could be misleading when comparing to previous studies in the literature and would lead to either overestimation or underestimation of the findings. Standardization of anatomical classification of these regions will be helpful for comparison purposes in future CBCT studies.
CONCLUSION
While examining CBCT images, it is vital to check for evidence of IFs in the TMJ region. The findings of this study highlight the value of interpretation and thorough examination of all areas visualized on CBCT scans even those beyond the region of interest.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval for the retrospective review was obtained from the Ethical Committee of Isfahan University of Medical Sciences, Faculty of Dentistry, Iran.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
All patients participated on a voluntary basis and gave their informed consent.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [F.G], upon reasonable request.
FUNDING
This project was supported by Isfahan University of Medical Sciences, Isfahan, Iran.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

