All published articles of this journal are available on ScienceDirect.

Dentition Status and Treatment Needs Among Orphans in Riyadh City, Saudi Arabia: A Cross-sectional Descriptive Study
Authors Info & Affiliations
Abstract
Background:
Oral health affects the general health and quality of life of an individual. It has been well documented that the absence of family support influences the general and oral health of children. Factors that lead to the development of a disease are likely to have their roots in a complex chain of environmental events that may have begun years before the disease occurs. The purpose of this study was to examine the prevalence of dental caries and assess treatment needs of the orphans of Riyadh City, Saudi Arabia
Methods:
This cross-sectional study included 238 orphaned children aged 6 to 18 years. Clinical examination was conducted by two doctors, and oral findings were recorded according to the World Health Organization (WHO) oral health assessment form (1997). The data collected was analyzed using SPSS 21.0.
Results:
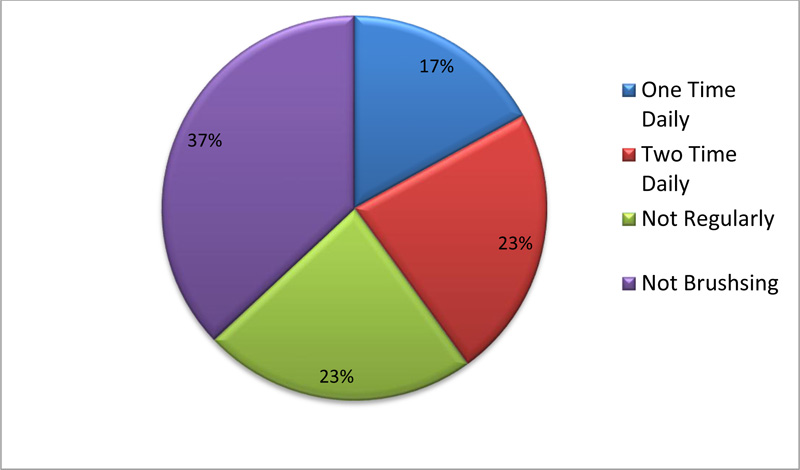
Results revealed that 37% of the participants reported that they do not brush their teeth, 23%of the participants reported that they do not brush regularly, 17% of the participants reported that they brush one time daily, and 23% of the participants reported that they brush twice daily. The prevalence of dental caries among the participants was 96.6%. When examining treatment needs among study participants, 7.6% might need preventive caries arresting care, 49.6% might need fissure sealant applications, 51.3% might need at least one surface filling, 13.1% might need two or more surface filling, 2.5% might need crown for any reason, 0.4% of participants might need veneer or laminate, 0.2% of participants might need pulp care and restoration, and 8.1% might need extraction.
Conclusion:
Results of our study indicate that orphan children have low utilization of preventive and therapeutic oral health services. Urgent attention is required to plan a comprehensive dental health-care program to improve their oral health status.
1. INTRODUCTION
Parents are the primary caretakers of a child. They take care of their children by protecting them from hazards and teach them honesty, courtesy, respect, generosity, and love. Unfortunately, there are many children underprivileged from their parents’ care either one of them or both of them. The United Nations International Children’s Fund and global partners define an orphan as a child under 18 years of age who has lost one or both parents for any cause of death. By this definition, due to wars, natural disasters, infections, and other causes, there are nearly 140 million orphans living in the world today [1, 2] . According to the Ministry of Labor and Social Development in Saudi Arabia, in 2015, there were 1145 orphans in Riyadh, a region of Saudi Arabia [3].
Oral health is an important contributor to overall health and well-being [4,5] . According to the new definition of oral health that was announced by the World Dental Federation, and over 200 national dental organizations, includingthe American Dental Association, “The oral health is multi-faceted and includes the ability to speak, smile, smell, taste, touch, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort, or disease of the craniofacial complex [6,7]. A gloobal review of oral health showed that 90% of schoolchildren worldwide experienced caries [8,9].
The level of oral diseases in the community is influenced by the environment, individual’s lifestyles, behaviors, and socioeconomic factors [10]. Despite improvements in oral health with newer technology and materials, the global problem persists. Oral disease is particularly more prevalent among underprivileged groups, and orphans are considered a high-risk group [11, 12]. According to the Social Affairs Ministry of Saudi Arabia, there are 12,000 orphans among a population of 28 million [3]. The orphans represent 3% of the total population of children in Saudi Arabia. Although orphans contribute to 2% of the world’s population, studies regarding their oral health status are scarce. To the fullest of our knowledge, there has been no previous study addressing the issue of oral health of orphans in Riyadh, Saudi Arabia. This study aimed to assess the prevalence of dental caries in orphaned children in Riyadh, Saudi Arabia. Our study will provide insight regarding dental health in orphans, which is a significant issue, so that the government and the private sector can be aware of this issue and so that programs addressing this issue can be developed.
2. MATERIALS AND METHODS
A descriptive cross-sectional study was conducted to assess the prevalence of dental caries and to assess the treatment need among orphans in Riyadh, Saudi Arabia. This study was approved by the ethical committee of Riyadh Elm University (IRB approval: FIRP/2018/156).Approval was taken from Insan Orphanages center (Fig. 1). By considering the prevalence rate of dental caries to be 90%, the sample size required was 238 at 95% confidence level and 5% confidence interval. Participants were randomly selected and a total of 238 orphans were included, divided as 177 (74%) male orphans and 61(26%) female orphans. We included orphans aged 6 to 18 years and orphans who were willing to participate and cooperate.
There were three interns. The interns were trained by the principal researcher to fill the form that was the World Health Organization oral health assessment form (1997) [13,14]. A clinical examination was conducted on all 238 participants. All examinations were carried out in a well-lit room. Instruments used in examinations weredisposable dental examination kit,which consisted of a dental examination mirror Kerr model PE9401, Anhui, China, double-ended probe (examination/perio WHO-type 3.5, 5.5, 8.5 & 11.5mm) Kerr model PE9401, Anhui, China, tweezers Kerr model PE9401, Anhui, China, masks Kerr model PE9401, Anhui, China, bib Kerr model PE9401, Anhui, China, tissue wipe Kerr model PE9401, Anhui, China, cotton rolls Kerr model PE9401, Anhui, China, and a biodegradable tray Kerr model PE9401, Anhui, China, with disposable gloves, Sanita, Riyadh, Saudi Arabia. A structured questionnaire that was originally written in English was translated in Arabic and distributed in both English and Arabic (Fig. 2). The respondents were asked questions on basic knowledge, such as frequency of brushing, technique of brushing, and methods and aid used for cleaning oral cavity. We added a question about the use of miswak as a method for taking care of oral health. Miswak is a traditional chewing stick prepared from the roots, twigs, or stem of Salvadora persica tree and has been used in the country as a natural method for tooth cleaning. A number of scientific studies have demonstrated that miswak (Salvadora persica) possesses antibacterial, anti-fungal, anti-viral, anti-cariogenic, and anti-plaque properties [15]. The Simplified Oral Hygiene Index (OHI-S) by Greene and Vermillion [16] was used and included a debris index, calculus index, plaque index, and gingival index. Each of these indexes is based on numerical determinations representing the amount of debris or calculus found on the preselected tooth surfaces. The examination was performed by using the Disposable Examination Kit.
2.1. Statistical Analysis
The data were analyzed using SPSS version 21. Mean and standard deviations were calculated to express the mean Decayed Missing Filled Surface DMFS values. The chi-squared test was used to assess associations between treatment needs and various risk factors including lifestyle and social support, oral hygiene practice, utilization of a toothbrush, a toothpaste, and dental floss, and frequency of visits to dentists. Specific statistical testswere used including (Spearman’s rho, Mann-Whitney U) .A p < 0.05 was considered statistically significant.
3. RESULTS
The age range of the study participants was 6 to 18 years, with a mean age ± standard deviation of 13.98±2.45 years. The majority (93.6%) of the participants were 10 years and above. The gender distribution of the study participants was 177 male participants and 61 female participants.
Results revealed that 37% of the participants reported that they do not brush their teeth, 23% of the participants reported that they do not brush regularly,17% of the participants reported that they brush one time daily and 23% of the participants reported that they brush twice daily (Fig. 3), which indicate that the participants were highly susceptible to dental caries.
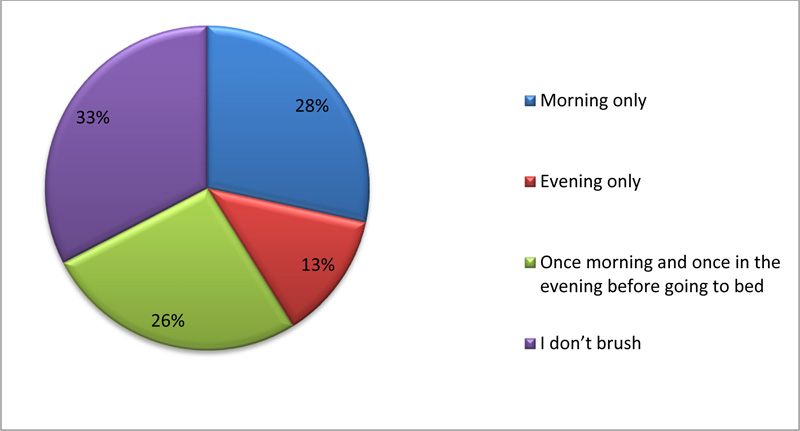
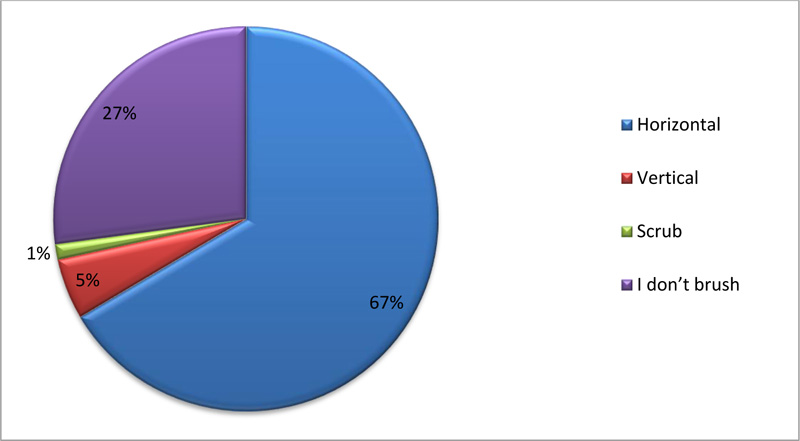
When evaluating the time at which participants brush their teeth, 28% of the participants used to brush their teeth only at morning, 13% of the participants used to brush their teeth only at night and 26% of the participants used to brush their teeth both morning and night (Fig. 4). While examining the technique of brushing, 67% of the participants would brush their teeth in the horizontal direction , 5% of the participants would brush their teeth in a vertical motion and 1%of the participants would brush their teeth in a scrub motion (Fig. 5).
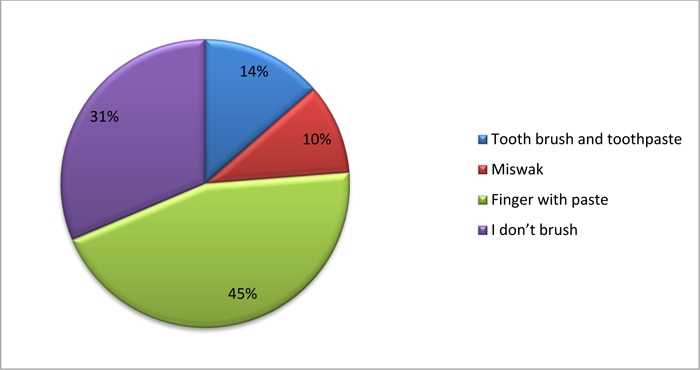
While examining the tools used by orphans for brushing their teeth,14% of the participants reported to brush their teeth using a toothpaste with a brush, 10% of the participants reported to use miswak and 45% of the participants reported to use their finger with toothpaste.
Study results show that the prevalence of dental caries among participants was 96.6% for debris index, calculus index, plaque index, and gingival index. The median score was one. The scoring criteria are listed in Table 1. Spearman’s Rho showed a statistically significant positive correlation between debris index, calculus index, plaque index, and gingival index (p=0.000) .
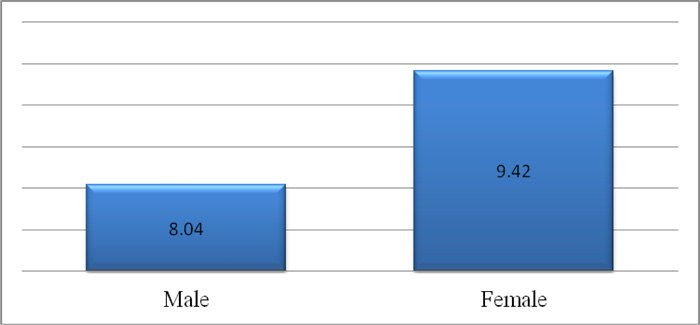
The mean ± standard deviation DMFS of the participants was 8.40±4.19 (range: 0-18). The mean ±standard deviation DMFS of female participants (9.42±3.20) was higher than that of male participants (8.04±4.44) (Fig. 6). Furthermore, the Mann-Whitney U test showed that this difference was statistically significant (p=0.008). Spearman’s Rho showed a statistically significant positive correlation between DMFS and age (rho=0.216, p=0.001), suggesting that DMFS increased with age.
| Index | Median Score | Scoring Criteria |
| Debris | Score 1 | Soft debris covering not more than 1/3rd of the exposed tooth surface or presence of extrinsic stains without other debris regardless of surface area covered |
| Calculus | Score 1 | Supragingival calculus covering not more than 1/3rd of the exposed tooth surface |
| Plaque | Score 1 | A film of plaque adhering to the free gingival margin and the adjacent area of the tooth. The plaque may be recognized only by running a probe across the tooth surface |
| Gingival | Score 1 | Mild inflammation, slight change in color & edema, but no bleeding on probing |
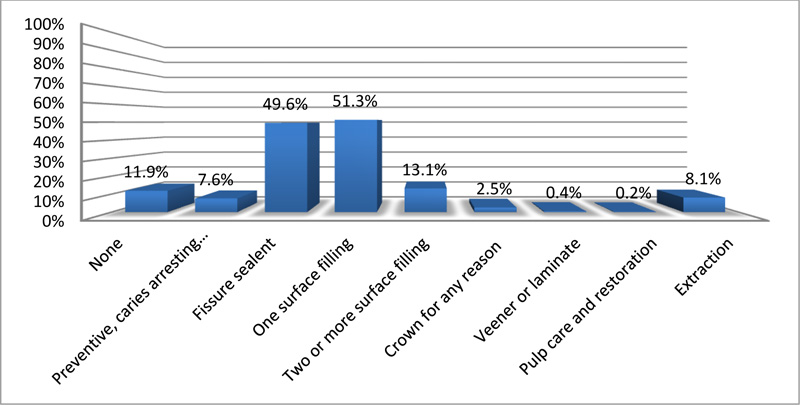
When examining treatment needs among study participants, 7.6% needed preventive caries arresting care, 49.6% needed fissure sealant applications, 51.3% needed at least one surface filling, 13.1% needed two or more surface filling, 2.5% needed crown for any reason, 0.4% needed veneer or laminate, 0.2% needed pulp care and restoration and 8.1% of participants needed extraction (Fig. 7).
4. DISCUSSION
Nowadays,, parents face many difficulties in controlling their children from consuming candies and beverages that effect their oral health. In contrast for those whose don’t have their parents with them, there is no one to make sure of children’s oral health, resulting in increased consumption of candies and beverages which cause more caries as reported in a study by Caneppele TM, Jeronymo RD [17] , in their study that done on one hundred standardized dentin slabs obtained from bovine incisor roots which study effect beverage on teeth, result shows increase of erosion on roots dentin which mean more caries which show why we have high consideration about consumption of beverages, candies, sweet etc.
In Saudi Arabia, although there are many epidemiological studies on oral health in children, limited studies have examined oral health in orphan children in Saudi Arabia. The main purpose of this study was to identify the dentition status and treatment needs among orphaned children of Riyadh City, Saudi Arabia.
The present study included 238 orphans among them 93.6% were ≥ 10 years of age.
The mean record of DMFS was 8.40±4.19.Previously, Alsadhan [18,19] reported that the DMFS value ofmale schoolchildren aged 12-14 years was 7.20 ± 3.89. Our results showed that the DMFS value of male orphans was 8.04±4.44 which is higher than the that shown in Alsadhan study which seems realistic due to loss of their parents. The caries prevalence in our study participants was 96.6%, which is higher when compared to a previous study conducted by Aldosari [20], which reported that caries prevalence among intermediate schoolchildren was 92.3%.
Regarding brushing teeth,37% of the participants reported that they do not brush their teeth and 23% of participants reported that they do not brush their teeth regularly. This may be explained by the fact that since the participants lost their parents,they neversaw their parents brushing their teeth while the participant was of preschool age. Ozbek [21] compared the tooth brushing habit between children and their parents and the result showed significant association in the frequency of tooth brushing between the parents and their children. If their parents brushed their teeth once a day, children were more likely to brush their teeth ≥1 time a day.
The majority of the participants needed preventive care followed by fissure sealant, one surface filling, two surface filling, pulp therapy, malocclusion correction, and extractions. Out of 238 participants, only 3.4% showed good oral health care. These figures were compared with a study by Khare et al. [22], where 26.2% of the participants required one surface filling which was lower than our study being 51.3%.18.3% required two or more surface fillings which was higher than the result achieved in our study being 13.1%.8.1% of the partipants in our study had teeth requiring extraction,compared to 5.2% reported in the study by Khare et al study. Finally, acidic environment that result from eating high sugar content food and drinks that mainly found in sweets, beverages, etc. can effect even restoration, study done by poggio, violo, mirando [23] focused on effect of beverage on some types of restoration, in their study they used thirty specimens of each esthetic restorative material., their results shows the effect of acidic environment on restorations (Needs to be rephrased).
5. LIMITATION
In our research, there are limitations; firstthe data collected for habits and practices may be limited. Secondly, there were some difficulties faced in achieving a balance between the number of male and female orphans due to refusal from some females to participate which influenced the result of the research. Third, the data on oral health knowledge, attitudes, and practices of orphan children with regard to consumption of sugary foods and drinks are very scarce. Due to this fact, and a comparison with a non-orphan population consider one of the limitation in our study, this research can used as reference in future researches.
CONCLUSION
Death or absence of one or both parents can lead to bad oral health of children. Thus, orphaned children are vulnerable and are potentially at an increased risk for poor health. This study shows that there is a great need for implementing preventive measures among orphaned children living under special circumstances. This research is the first study of its kind conducted in Saudi Arabia and there were no prior study conducted in Saudi Arabia. It has been observed that the oral health of orphans was poor and this community has low utilization of preventive or therapeutic oral health services. Prevention programs targeting dental caries such as sealant programs and fluoride programs should be started soon as possible for this population. In the future, orphans should be considered a priority group when formulating plans for oral health care.
LIST OF ABBREVIATION
| DMFS | = = Decayed Missing Filled Surface |
AUTHOR’S CONTRIBUTIONS
TO and BS and AS performed the examination on the children, KA and did the research design, AA and made the structured questionnaire construction in English and translated to Arabic. RD performed the data analysis, AA and TO were major contributors in writing the manuscript. All authors read and approved on the final manuscript
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethical Committee of Riyadh Elm University, Saudi Arabia (IRB approval: FIRP/2018/156).
HUMAN AND ANIMAL RIGHTS
No animals were used in this study. All humans research procedures followed were in accordance with the guidelines of the Declaration of Helsinki of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
Informed consent approval letter was given by Ensan, the Charity Committee for Orphans Care
AVAILABILITY OF DATA AND MATERIAL
The data that support the findings of this study are available from the corresponding author, [A.A], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank all the head of Ensan the Charity Committee for Orphans Care, caretakers of orphanages and all the children who participated in the study. for their cooperation.

