All published articles of this journal are available on ScienceDirect.

Evaluation of Fracture Resistance and Sites of Failure of Different Dowel Core Restorations: An In-Vitro Study
Abstract
Background:
Dowel Cores are often required in endodontically treated tooth to aid retention and resistance for a final prosthetic crown. Studies concerning the role of post-core systems on the fracture resistance with different dowel material remain controversial.
Aim:
This experimental study aimed to investigate the fracture resistance strength and failure mode of 3 dowel systems (glass fiber, indirect resin, and prefabricated metal with resin core).
Methods:
Twenty-one extracted human maxillary central incisors were first endodontically treated and then separated into 3 equal groups randomly;1st group consisted of glass fiber dowel, 2nd group consisted of indirect resin dowel, and 3rd group consisted of the prefabricated metal dowel. All specimens were restored with resin core and indirect resin crown. A testing force was applied with a universal testing machine (at 135 o angle) at 3 mm from the incisal edge of crown and forces were measured. Statistical tests were done using One-way ANOVA and Chi-square Test.
Results:
There was no significant difference (P-value >0.05) of the fracture resistance among glass fiber dowel, indirect resin dowel and pre-fabricated dowel with indirect resin crown. The prefabricated metal dowel had maximum fracture resistance (566 ±157.771 N) followed by Glass fiber dowel (541.047 ±199.571 N) and indirect resin dowel and post (444.550 ±139.788 N).
Conclusion:
Glass fiber dowel, indirect resin dowel and prefabricated metal dowel with resin core and indirect resin crown systems showed statistically insignificant fracture strength values and mode of failure.
1. INTRODUCTION
Endodontic/ root canal treated teeth lose considerable structure of tooth from caries, restorations, and cavity preparation for endodontic treatment [1]. After endodontic treatment, the tooth becomes brittle because of structural change in the dentin and collagen cross-linking which may lead to fracture or tooth and/or root [2].
Dowel/ post and cores are often needed in endodontically treated tooth to provide retention and resistance form for final crown, and finally to restore the form and function of the tooth. Hence, the restoration of endodontically treated teeth with posts and direct resin conserves the remaining tooth structure [3, 4]. The coronal restorations are done to replace structure loss, to restore coronal morphology and functions, to provide the strength for the restoration/tooth complex to with stand functional stress [5].
There are 2 types of dowels according to the materials made from; metallic and non-metallic dowels used in clinical dentistry. Other types of dowel systems are available to restore the tooth structures, such as prefabricated or custom cast, parallel or tapered, and active or passive [6]. Prefabricated metal dowels are popular due to their low cost, convenient, and simplicity [7]. But the disadvantages of such systems are poor retention of the dowel, fracture of dowel and root, and chance of corrosion when used different materials [8, 9]. Besides, when the root canal is curved, it is difficult to obtain optimal adaptation. Therefore, in this situation, a custom/ indirect resin dowel build-up method might be the preferred option [10].
The custom cast dowel has the advantage of good fit and retention, precise marginal integrity, ideal contacts, and reproduction of anatomic morphology [11, 12]. But these dowels are less aesthetic compared to fiber post [13]. The non-metallic dowels are esthetic, flexibility than metal dowels and presence of the same modulus of elasticity as dentin. Hence, they help in the force distribution more evenly in the root preventing root fractures [6]. Various fiber dowels also are available including carbon, quartz, glass and silicon dowels.
With recent advances in different forms of indirect resin materials, the study on the properties of these materials as dowel and crown material will be beneficial to overcome shortcomings of conventional dowel core materials and system. Central Incisors (CIs) for the important part of dental esthetics [14-16]. This experimental study was to investigate the fracture resistance strength of CIs and failure mode for each dowel system (glass fiber, indirect resin, and prefabricated metal with resin core).
2. METHODS
2.1. Specimen Preparation
Ethical clearance (IRB number 6.11E) for this study was obtained from the Institutional Review Board, Institute of Medicine, Tribhuvan University and this in vitro study was conducted from 2011-2012. This report followed the protocol established by the modified CONSORT Statement for reporting pre-clinical In vitro studies on dental materials [17]. Twenty-one central incisors (CIs) meeting the criteria were collected from the patients who were undergoing extraction (i.e. for complete denture prosthesis, orthodontic purpose, trauma, etc.) according to the convenient sampling as shown in Table 1. CIs were selected as they are most prone to trauma in the anterior region. At first, CIs were disinfected with 10% formalin for 1 week and then immersed in 5.25% sodium hypochlorite (NaOCl) solution to remove soft tissues and debris. Calculus on teeth was then removed with ultrasonic scalers and subsequently stored in distilled water. The maximum Bucco-Lingual (B-L) and Mesio-Distal dimensions (M-D) of all these teeth were measured as the Cemento-Enamel Junction (CEJ).
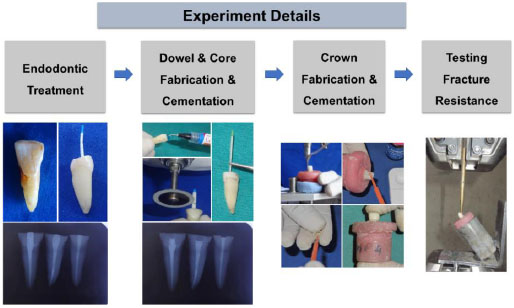
Then, a line was drawn 4 mm from CEJ (M-D and B-L) parallel at CEJ and perpendicular to the long axis of the root and the crown of each tooth was cut with a diamond disk with continuous water irrigation. The study detail is shown in Fig. (1).
| Selection Criteria | |
|---|---|
| Inclusion criteria | - Teeth selected were within these variables; length of each root:13 ± 2 mm and mesiodistal width at cervix: 7 ± 0.4 mm. |
| Exclusion criteria | - absence of root-surface caries, visible fracture lines, abrasions and abfractions, crown fractures and previous restorations. - Internal root resorption/ obstruction in the root canal. |
2.2. Endodontic Treatment
Access cavity preparation was performed, and apical patency was maintained using a size #10 K-file (Dentsply-Maillefer, Ballaigues, Switzerland). Then, the working length was made 1 mm short from the apical foramen. The root canals were instrumented using rotary Pro Taper files S1, S2, F1, F2, F3) (Dentsply, Maillefer, Ballaigues, Switzerland). The canals were irrigated with 2% NaOCl and 17% Ethylene-Diamine-Tetraacetic Acid (EDTA) (Glyde, Maillefer, Dentsply, Ballaigues, Switzerland), and dried with paper points (Protaper Paper points, Maillefer, Dentsply, Ballaigues, Switzerland). The canals were filled with gutta-percha (Protaper Gutta-percha points, Maillefer, Dentsply, Ballaigues, Switzerland) and endodontic sealer (AH Plus; Dentsply DeTrey, Konstanz, Germany) with the lateral condensation and vertical condensation. Then, sealed with a filling material (ORAFIL-G- Prevest Dent Pro) and radiographs were taken, and the specimens were kept for 1 week in deionized water at room temperature. After 1 week, specimens were polished with sandpaper (600-grit) until the specimen was 2 mm short from the CEJ and dowel preparation was done.
The specimens were separated into 3 groups randomly to receive different types of dowel materials: glass fiber dowel (n = 7), indirect resin dowel (n = 7), and prefabricated metal dowel (n=7) (Fig. 2) and dowel preparation was done according to the manufacturer’s recommendations.
2.2.1. Group 1: Glass Fiber Dowel
Dowel space preparation. Gutta-percha was removed predrilling with a drill (Largo drill, Ref. A0009 no. 2. EasyPOST TM Precision Drill REF C 0601-3) with a depth of 11 mm which was confirmed from a silicone stopper on the drill. Dowels were tried in the tooth to check their fit in the canal.
2.2.1.1. Dowel Core Preparation
The dowel spaces were cleaned and conditioned with EDTA for 1 min and 36% phosphoric acid for 15 sec. They were rinsed with NaOCl, cleaned with 70% alcohol, and dried with paper points. Then, 1 drop of adhesive (Prime & Bond NT, Dentsply Sirona, Milford DE, USA) and bonding agent (Self-Cure Activator, Dentsply Sirona, Milford DE, USA) were mixed well for 2 seconds with a small brush tip. The mixture of adhesive/activator was applied to dowel preparation on all surfaces properly and kept for 20 seconds and air-dried with air syringe followed by dry paper points. Air entrapment was avoided while applications. Dual cured resin cement (CalibraTM, Dentsply Sirona, Milford DE, USA) base and catalyst pastes were mixed for 20 sec on a mixing pad by taking an equal amount mixed. Mixed cement was applied on the surface of dowel and into the dowel preparation with Lentulo Spiral, and dowel was sealed immediately. Excess cement was wiped, and dowel was stabilized with finger pressure until set. Cemented dowels were cured for 20 seconds using light-cured. Then, the cemented dowel was cut to a length of 3 mm incisal to the labial preparation.

2.2.2. Group 2: Indirect Resin Dowel
Dowel space preparation. Gutta-percha was removed predrilling with a special penetration drill, Ref. A0009 no. 2. Precision Drill REF C 0601-3 was used for dowel space preparation to a depth of 11 mm using a silicone stopper on the drill for standardization of dowel length and diameter.
2.2.2.1. Dowel Core Preparation
For fabrication of indirect resin dowel, silicone putty index of the easy post was made and cut half to pack the indirect resin (Ceramage, Shofu Dental GmbH Ratingen, Germany). The pattern obtained was trimmed and adjusted in the individual canals. For customization of dowel above the canal, silicone index was made from fiber dowel to obtain the diameter like other groups. Cementation and treatment of dowel space and dowel were done in a manner like the fiber dowel. After cementation, the dowel was cut to a length of approx. 3 mm incisal to the labial preparation. Cores were made in a similar as in group1.
2.2.3. Group 3: Prefabricated Metal Dowel
2.2.3.1. Dowel Space Preparation
Special penetration drills 0212, 0213, 02014 were used for gutta-percha removal and dowel space preparation. Silicone stopper was used to ensure the drill up to 11 mm.
2.2.3.2. Dowel Core Preparation
For dowel cementation of UNIMETRIC 215 T dowel (titanium alloy) (no. 310; Maillefer Instruments) procedures like group 1 were used. Cores are made in a similar as in group 1. Tooth preparation was done on all the specimens with a resin core. A line was marked 3 mm below the incisal edge of the specimens on the palatal surface of each specimen (0.5 mm deep and 0.5 mm wide) with a round bur.
2.3. Crown Fabrication
Crowns were fabricated in all the specimens of 3 groups from indirect resin (Ceramage, Shofu Dental GmbH Ratingen, Germany) of 1 mm thickness and height 2 mm. The margins were finished using a finishing kit. All indirect resin crowns were cemented in a specimen using dual-cure resin cement. Etching and bonding were done following manufacturer instructions. Cementations were done with dual-cure resin cement (CalibraTM, Dentsply Sirona, Milford DE, USA). The specimens for the experiments had different dowel with resin core and indirect resin crown with the dimensions of the dowel and cores from the mesial aspect were: lengths of the dowel = 9 mm, length of the core = 5 mm, length of final restoration = 7 mm, and width of the dowel = 1 mm.
2.4. Measurement of Fracture Resistance
Alveolar bone and periodontal ligament simulation. The root surface of each specimen was dipped 2 mm below the CEJ into melted wax to produce a 0.2 to 0.3 mm layer of wax. This layer of wax is considered to simulate the average thickness of the periodontal ligament. Specimens were embedded in autopolymerizing acrylic resin (Orthoresin, Dentsply Sirona, Milford DE, USA) with silicone cylinder matrix, vertically with the help of a surveyor to a depth of 1 mm apical from the CEJ. After the first signs of polymerization, the specimen was removed from the resin blocks by moving rods in an upward direction, and the wax spacer was removed from the root surfaces. Light body silicon impression material (ExpressTM XT Light body, 3M ESPE Seefeld, Germany) was injected into acrylic resin molds, and the specimen was reinserted. All specimens were stored at 37ºC for 24 hours.
Specimens were subjected to static loading in a universal testing machine (Shimadzu AG-100kNIC). Each specimen was placed in a special jig at an angle of 45◦ to the B-L axis so that loading probe could be positioned over predesigned indentation [18] on the lingual aspect of the buildup 3 mm from the incisal edge. A 45◦ was selected as this angle was taken as the normal angle between upper and lower central incisors. The specimen was subjected to force with a crosshead speed of 2 mm/min and subjected to load on a universal testing machine (Shimadzu AG-100kNIC). The load was applied until fracture of any part of the root, dowel, core or crown occurred. Fracture resistances point was monitored graphically in a screen of a universal testing machine.
2.5. Analysis of Failure Mode
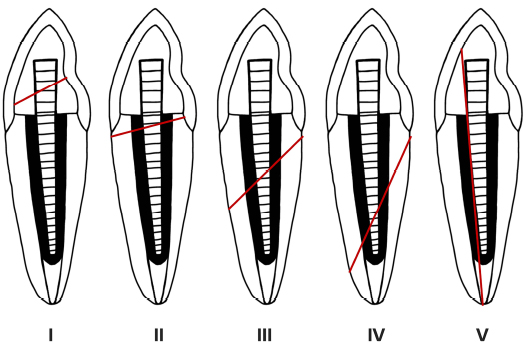
The failure mode was examined in each specimen from the visual examination, photographs and intraoral periapical radiographs according to the site of the failure. Then, they were classified using a classification system given by Zhi-Yue and Yu-Xing [19] as shown in Fig. (3) [20].
3. RESULTS
3.1. Results of Fracture Resistance
Table 2 shows the descriptive statistics of the fracture resistance of 3 dowel groups; glass fiber dowel, indirect resin dowel and pre-fabricated dowel with indirect resin crown. It showed that the prefabricated dowel had maximum fracture resistance (566 ±157.77 N) followed by glass fiber dowel (541.05 ±199.57 N) and indirect resin dowel and post (444.55 ±139.79 N).
The box plot diagram of the fracture strength is shown in Fig. (4). Glass fiber dowel group showed the maximum range and the prefabricated dowel group showed the least range.
| - | n | Mean ±SD | Std. Error | 95% CI for Mean | Min | Max | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Glass fiber dowel | 7 | 541.05 ±199.57 | 75.43 | 356.47 | 725.62 | 275.78 | 783.25 |
| Indirect resin dowel and post | 7 | 444.55 ±139.79 | 52.83 | 315.27 | 573.83 | 176.90 | 617.03 |
| Pre-fabricated metal dowel | 7 | 566.48 ±157.77 | 59.63 | 420.56 | 712.39 | 225.21 | 697.84 |
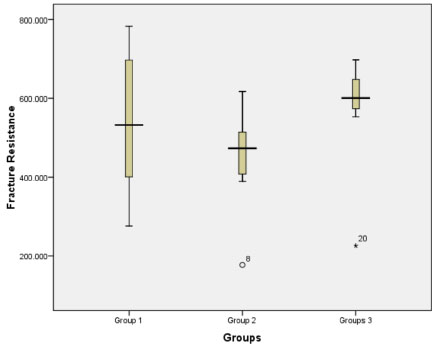
Table 3 shows the multiple comparisons of the fracture resistance among 3 dowel groups. It showed that there was no significant difference (P-value > 0.05) of the fracture resistance among glass fiber dowel, indirect resin dowel and pre-fabricated dowel with indirect resin crown.
| Multiple Comparison of fracture strength | P-value |
| Group 1 vs Group 2 | 0.57 |
| Group 2 vs Group 3 | 0.41 |
| Group 1 vs Group 3 | 0.96 |
3.2. Results of Fracture Resistance
It showed that there were no differences in the mode of failure between, glass fiber dowel indirect dowel and prefabricated metal dowel groups (Table 4). Fracture in the crown, core, and/ or cervical third of the root (mode I) was predominant in all groups. In addition, the site of failure was found within type I and type II in all groups. From Chi square test showed that there was no significant difference (P value = 0.112) for the failure mode among glass fiber dowel, indirect resin dowel and pre-fabricated dowel with indirect resin crown.
| Failure Mode | 1 | 2 | 3 | 4 | 5 | P-value |
|---|---|---|---|---|---|---|
| Glass fiber dowel | 6 | 1 | 0 | 0 | 0 | 0.112 |
| Indirect resin dowel and core | 4 | 3 | 0 | 0 | 0 | |
| Prefabricated metal dowel | 5 | 2 | 0 | 0 | 0 | |
| Total | 15 | 6 | 0 | 0 | 0 | - |
Table 5 showed that there was a weak positive no significant correlation between fracture resistance and 3 dowel types.
4. DISCUSSION
Central incisors form a major esthetic component but are most commonly prone to traumatic injury [15, 21-23]. The evaluation of the fracture resistance of the incisors and failure mode of a dowel and core system is important for the improvement of their performance. Varieties of dowel core systems are available for the build-up and stabilization of endodontically treated teeth. The durability of dowel core restoration depends on the fit between dowel, the residual dentine of root canal, and the bond between the core and dowel material enabling to transfer stresses under functional loading. Some studies were done to compare the mechanical properties of different dowel core systems, but the results were contradictory and were limited to specific dowel [20, 24-27]. As a result, there were confusions in the literature regarding how dowel core material affects the resistance performance of restored teeth [28]. Hence, our study was conducted to evaluate the fracture resistance and mode of failure of different dowel materials. Fiber-reinforced, indirect resin and prefabricated metal dowels were used. All specimens were restored with a complete coverage crown before testing to simulate the clinical situation.
| Pearson Correlation | ||
|---|---|---|
| - | Groups | Fracture Resistance |
| Groups | 1 | 0.063 |
| Fracture Resistance | 0.063 | 1 |
| Sig. (2-tailed) | .785 | .785 |
In our study, it showed that there was no significant difference (P-value >0.05) of the fracture resistance among glass fiber dowel, indirect resin dowel and pre-fabricated dowel with indirect resin crown. This agrees with other studies [29, 30]. Raygot et al. [29] found no statistically significant differences in fracture resistance values between the groups (cast post-and-core, carbon fiber-reinforced composite post or prefabricated stainless steel post systems) and Hu et al. [30] also found no statistically significant differences in fracture resistance values between the groups (cast dowels and cores, carbon-fiber dowels with resin-composite cores, and ceramic dowels with resin-composite cores). Another similar study was done by Öztürk et al. [31] which compared the fracture resistance and fracture mode of endodontically treated thin-walled teeth which restored with different post systems: only composite resin, cast post, glass-fiber post, and I-TFC post. There were significant differences in the fracture resistance of teeth among the groups. They found that the highest fracture resistance was recorded for cast post, followed by the glass-fiber, ITFC post, and composite resin. In addition, Pruthi et al. [32] found that double tapered posts showed better fracture resistance than parallel and tapered posts.
Regarding the mode of failure in our study, the majority of the failures were a post or core fracture (I) and root fracture in cervical third (II) as shown in Fig. (4) and Table 4. This is like the results found by other studies [33, 34]. Yaman et al. [33] evaluated the stress distribution in a maxillary central incisor restored with various dowel-core applications using a finite element method and found that core material was of greater importance than dowel material or size. In another study, the stress distribution was around the neck of the metal implant near the cervical area [34]. Similarly, in another study done by Akkayan and Gulmez [24], they compared the fracture resistance and mode of fracture of quartz fiber, glass fiber, titanium, and zirconia dowels and found that quartz and glass fiber groups fractured favorably (fractures able to be repaired). Catastrophic fractures were observed in the titanium and zirconia groups. Another study reported similar fracture resistance of anterior teeth restored with carbon fiber composite dowel-composite cores and metallic dowels-composite cores [35]. Also, they found 50% of failures of the metallic dowels involved root fractures, whereas no root fractures were found with the carbon fiber composite dowels. Two other studies found that the dowel-core and crown system with metallic dowel was more resistant to fracture than the carbon fiber composite dowel system [20, 36].
In our study, it was seen that there is a large variability in the fracture loads for each of the three groups of test specimens and we found that the prefabricated dowel had maximum fracture resistance (566 ±157.77 N) followed by glass fiber dowel (541.05 ±199.57 N) and indirect resin dowel and post (444.55 ±139.79 N). This might be because of the high strengths of metallic posts and low strengths of indirect resin posts.
It was found that the average maximal bite force in the central incisors region to be 140 N [37]. Regarding gender, males have higher maximal bite force (146.17 to 175.14 N) than females (93.88 to 112.57 N) [38, 39]. Hence, the force exerted on the specimens in our study was >444 N which is much higher than the biting forces from various studies. This indicates that the fracture strength of all 3 dowel core systems is acceptable. The advantages, disadvantages, and indications of different dowel systems used in this study are shown in Table 6.
| Dowel Systems | Glass Fiber Dowel | Indirect Resin Dowel | Prefabricated Metal Dowel |
|---|---|---|---|
| Advantages | • Esthetic • Moderate fracture resistance • Removability |
• Moderate esthetic • Better fitting |
• High strength • Maximum fracture resistance • Removability |
| Disadvantages | • Mostly radiopaque | • Least indirect resin dowel and post | • Least esthetic • Radiopaque |
| Indications | • Indicated when high esthetic is required | • Useful teeth without loss of tooth structure | • Useful for grossly decayed teeth and high strength is required |
Regarding limitations, this study only pertains to in vitro fracture resistance and mode of failure of the glass-fiber, indirect resin, and metal dowels. Prosthodontic structures do not break because of a single, intense episode of stress application, but rather as the end effect of many comparatively small loadings on the entire tooth-supporting tissues-restoration complex. This study lacks specimen fatiguing, aging, thermal and mechanical cyclic loading that are interesting features when analyzing endodontically treated teeth. Finally, only the single loading point and angle were tested in this study. Further study can be done considering multiple angles in various angles.
CONCLUSION
Following conclusions can be drawn:
- All studied dowel (glass fiber, indirect resin and prefabricated metal dowel with resin core) showed much higher fracture resistance than normal biting force.
- There was no difference in the fracture resistance of glass fiber, indirect resin and prefabricated metal dowel with a resin core.
- Glass fiber dowel, indirect resin dowel, and prefabricated metal dowel showed predominantly similar fracture mode (core and crown fracture) indicating that there is less influence of dowel materials on fracture mode.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of Institutional Review Board, Institute of Medicine, Tribhuvan University (Code # 6.11E).
HUMAN AND ANIMAL RIGHTS
No animals/humans were involved in studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available from the corresponding author (M.G) upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Thanks to People’s dental College for the materials support for this study.

