All published articles of this journal are available on ScienceDirect.

Prevalence of Early Childhood Caries in Children Aged 1 to 5 Years in the City of Quito, Ecuador
Authors Info & Affiliations
Abstract
Background:
Early childhood caries is an aggressive pathology that can destroy the teeth in a short time, reaching the proximal surfaces, causing discomfort, pain and affecting the dental pulp, causing premature loss of deciduous teeth.
Objective:
The purpose of this research is to determine the prevalence of early childhood caries in children aged 1 to 5 years of the Metropolitan District of Quito.
Materials and Methods:
This is a cross-sectional study including a sample of 557 children attending child care centers in Quito, Ecuador, between May and July 2018. The sample was evaluated clinically registering the data in a simplified dental file containing the odontogram and the result of decayed, lost and sealed teeth, according to the dmft index, as well as data such as age and gender. Data were tabulated and analyzed statistically by independent t-test.
Results:
The prevalence of early childhood caries was found to be 59.61%. Children affected by early childhood caries presented a mean age of 2.83 years, the ones suffered the most from this pathology were those of 2 years (35.54%), followed by those of 3 years (34.94%) and 4 years (22.5%). Boys presented more early childhood caries (53.92%) in relation to the girls (46.08%).
Conclusion:
The early childhood caries presented a prevalence of 59.61% and a general dmft index of medium level of severity according to the classification of the World Health Organization, in children from 1 to 5 years of age in Quito, Ecuador.
1. INTRODUCTION
Oral health is an integral part of general health and is essential for a good quality of life. It is important that individuals have a good oral health condition that allows them to speak, chew, taste, smile and live without pain or discomfort. Since caries and periodontal disease are the most prevalent pathologies, the presence of caries from early infancy can cause damage to the teeth in the first three years of life, affecting the deciduous dentition and, in the future, permanent dentition [1, 2].
Caries is a biofilm (plaque)-induced acid demineralization of enamel or dentin, mediated by saliva [3]. The disease of Early Childhood Caries (ECC) is characterized by the presence of 1 or more decayed (noncavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger. In children younger than 3 years of age, any sign of smooth-surface caries is indicative of Severe Early Childhood Caries (S-ECC) [3]. From ages 3 through 5, 1 or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score of ≥4 (age 3), ≥5 (age 4), or ≥6 (age 5) surfaces constitutes S-ECC [3].
The presence of caries in children causes a series of sequels, such as infections, aesthetic problems, feeding difficulties, language alterations and the appearance of malocclusions and bad oral habits, as well as medical, emotional and financial repercussions. Factors such as low socioeconomic level and low levels of schooling, poor eating and hygienic habits, medical history, among other factors specific for each individual, can determine the susceptibility to the development of the disease [4].
Early childhood caries is an aggressive and very rapid growth pathology that can destroy the teeth in a short time. It can extend to the proximal surfaces, which can cause discomfort, pain and even affect the dental pulp, causing premature loss of deciduous teeth. For the child's parents, this destruction or an early loss of teeth is not a major concern, usually because they do not know about it. Therefore, they generally do not take the necessary steps to avoid it; consequently, it is not treated in time, causing a high degree of damage to the affected parts. It may even produce various disorders within the baby's oral cavity [5].
This type of caries can be detected with various levels of complexity, from incipient caries, which can be treated satisfactorily, until reaching the caries known as early childhood caries, which is mainly associated with the habit of using a bottle and the lack of adequate hygiene, producing a total or partial deficiency of the dental structures of children. Preliminary studies have shown that there is a relationship between early childhood caries and the intake of additional foods in breast milk at an early stage in an infant's life [5].
Despite the decline in the incidence of dental caries in children in Western countries, early childhood caries continues to be a major problem in developed and developing countries [6]. The prevalence of this type of caries varies greatly, depending on factors such as race, culture and ethnic origin; socioeconomic status, lifestyle, food standard and oral hygiene practices, as well as several characteristic factors different from one region to another. Previous research indicates that, in most developed countries, the prevalence rate of early childhood caries is from 1 to 12% [7]. In less developed countries and among disadvantaged groups in developed countries, prevalence has been reported to be as high as 70%, which is considered to be more prevalent in low socioeconomic groups [8].
In Europe, epidemiological studies have shown significant percentages of pre-school children affected by early childhood caries, confirming the widespread prevalence of the disease, dispersing randomly in the population, disproportionately affecting disadvantaged families [6]. The prevalence of early childhood caries ranged from 2.1% to 7% in Sweden, 19% in Italy and 36% in Greece [9].
A high prevalence has been reported in some Asian countries, such as Palestine (76%) and the United Arab Emirates (74.1%) [10, 11]. In other countries of the continent, an inconsistent prevalence of early childhood caries was found: in India (51.9%) and in Israel (64.7%) [12]. In addition, the research by Ismail and Sohn [13] found a prevalence of 85.5% in Chinese children in rural areas [6].
In the United States, prevalence was estimated to range between 3% to 6%, which is consistent with the prevalence in other Western countries, noting that the highest prevalence is found in the age group of 3 to 4 years and boys are significantly more affected than girls, aged between 8 months and 7 years [6, 14].
In the case of Latin America, the literature review found that in countries such as Mexico [15], the dmft index in children aged 2 to 4 y ears is between 2.4 and 4.3 years, with a tendency to increase with age, when older children registered an increase in the dmft index. This behavior was also reflected in Chile in the year 2010 [16], with a dmft index of 0.54 in children under 2 years of age which was dramatically higher in 4 years old children with 2.32. Ecuador has no exception regarding this reality, as the Ministry of Public Health in a National Epidemiological Study of Oral Health reported 6-years old children to have 79.4% of dmft (decayed, missing and filled deciduous) [17].
In Ecuador, there is not much research reported to study the phenomenon of early childhood caries. In the early childhood caries in Quito, only two studies were reported: Narváez and López studied the relationship between social determinants and the presence of caries in children between 1 and 5 years of age, and found a prevalence of 60.93 [18]. Likewise, in a study carried out in 2009, but published in 2017, Valarezo and Mariño analyzed the prevalence of early caries in children aged 1 to 4 years, and found a prevalence of 51.9% and a dmft index of 2.5 [19].
In general, these authors recommend that, due to the high prevalence in Quito, Ecuador, more research has been conducted in the area. This is why, this study is based on early childhood caries in children aged 1 to 5 years of the Metropolitan District of Quito, Ecuador, in order to determine the prevalence of caries and the dmft index.
2. MATERIALS AND METHODS
The present study is descriptive and cross-sectional with an aim to determine the prevalence of early childhood caries among preschool children attending the Metropolitan District of Quito, which consists of 141 nurseries, located in the north, central and south regions of the city of Quito, from May to July 2018. The study was approved by the Ethics Committee in Human Research of the Ingá Faculty.
The sample size calculation for the proportion confidence interval of 95% with an error of 5% for the expected proportion of 70% {8} required 323 individuals with a loss of 402 subjects.. For the proportion confidence interval of 99%, the sample should be of 557 subjects, in this way, we decided to use this number for increasing confiability of the results of prevalence of early childhood caries in Ecuadorian preschool children.
The study population corresponded to 6244 children, aged from 1 to 5 years, who attended the child care centers of the Metropolitan District of Quito, where 557 children were randomly selected and a clinical evaluation was performed using the dmft index, considering the variables, age and gender.
Among the inclusion criteria were considered: children from 1 to 5 years of age who attended the child care centers of the Metropolitan District of Quito, with informed consent signed by parents or legal guardians; children who allowed clinical examination to be performed; and who were present at the daycare center on the day of diagnosis. Exclusion criteria were: children with systemic diseases, syndromes or infectious diseases and use of orthodontic or orthopedic appliances.
The clinical examination of each child was carried out in a classroom with natural and front light, to avoid children from getting nervous, using only a dental mirror and a tongue depressor as support instruments, which were discarded after each use, in order to prevent the transmission of bacteria among children, as well as the necessary equipment to avoid any kind of contamination such as sterile gloves and face masks. During the clinical examination, each child was seated comfortably on an ordinary chair and examined by a sole examiner using a tongue depressor.
The data were collected exclusively by one researcher, in order not to misrepresent the results obtained during the diagnosis; therefore, no inter-examiner calibration was found necessary. This evaluator had previously been calibrated. The clinical examination and evaluation were carried out by a university professor specialized in pediatric dentistry, who was used to perform this type of evaluation routinely.
The clinical history was elaborated in two parts. In the first one, the data collected from the clinical examination of the children of the sample, containing informative data, such as the file number, date, name of the day care center, age and gender were collected.
The second part contained the simplified dental sheet, the odontogram and the account of decayed, missing and filled teeth, according to the dmft index, adopted by Gruebbel [20] for the deciduous dentition, which takes into account only the deciduous decayed, missing and filled teeth, considering only the 20 deciduous teeth. The exceptions of the dmft index were the teeth extracted in children by orthodontic treatments or lost by accidents, as well as crowns restored by fractures, excluding the teeth extracted previously, and including only the extractions indicated by caries exclusively.
The data recorded were tabulated in the Excel program, to perform statistical analysis with the aid of the SPSS program, with a confidence level of 95% and a significance of 5%.
3. RESULTS
The descriptive analysis of the 557 patients distinguished by the nominal qualitative variable gender with two levels of classification (female, male), the quantitative variable age between 1 and 5 years and the diagnostic variable according to the dmft index. Of the 557 children who participated in the study, 59.61% had caries representing 332 children and 40.39% had no caries, according to the dmft index.
Table 1 shows the mean dmft index for children with early childhood caries, showing that the total dmft is 1.28 and 1.21 for the girls and boys, respectively; for D (decayed), it0.98 and 1.00, for M (missing), 0.03 and 0.04, and for F (filled), 0.27 and 0.17. Girls had a total dmft index slightly greater than boys (Table 1). The highest percentage of patients with early childhood caries was of males, representing 53.92% in relation to the females, being 46.08% (Table 1).
| Gender | Decayed | Missing | Filled | Total |
|---|---|---|---|---|
| Females | 0.98 | 0.03 | 0.27 | 1.28 |
| Males | 1.00 | 0.04 | 0.17 | 1.21 |
| Gender | Patients | % | ||
| Females | 153 | 46.08% | ||
| Males | 179 | 53.92% | ||
| Total | 332 | 100.00% | ||
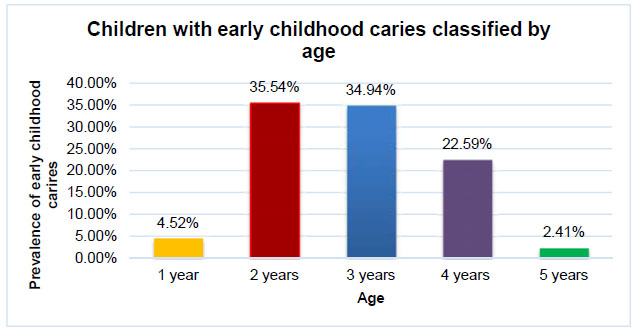
In Fig. (1), each bar represents the percentage of children classified by age group, where the children of 2 (35.54%), 3 (34.94%) and 4 (22.59%) years of age represent the highest number of subjects with caries, the lowest proportion of children with caries are with 5 years (2.41%) and 1 year of age (4.52%).
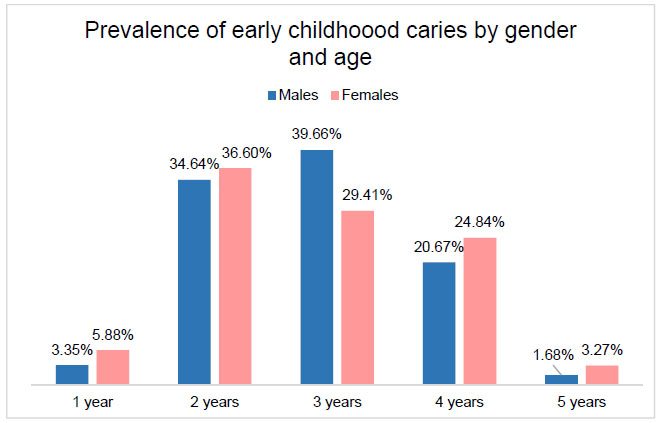
The prevalence of early childhood caries by gender and age Fig. (2) shows that 3-year-old male children have the highest caries value with 39.66% in relation to females (29.41%). When compared to the other ages, girls presented the highest percentage, at 2 years (36.60%), 4 years (24.84%), 1 year (5.88%) and 5 years (3.27%) of age.
Table 2 shows the mean and standard deviation, as well as the range for the only quantitative variable in the study, in which children with early childhood caries have a mean of 2.83 ± 0.91 years.
The Student's t-test was performed with a 5% significance to determine the difference between the mean of patients with early childhood caries and those who did not have caries according to age and gender. For age, the value of p was less than 0.05, therefore there is a relationship between patients with caries and age (Table 2). As the value of p is greater than 0.05, it has been concluded that there is no relation between the patients with caries and the gender (Table 2).
| Variable | N | Minimum | Maximum | σ | p-value |
|---|---|---|---|---|---|
| Age in years | 332 | 1 | 5 | 2.83 ± 0.91 | 0.000* |
| Gender | N | σ | p-value | ||
| Males | 298 | 1.40 ± 0.491 | 0.812 | ||
| Females | 259 | 1.41 ± 0.493 | |||
4. DISCUSSION
Early childhood caries, a dental disease in deciduous teeth, is considered infectious and transmissible, which can cause serious long-term consequences, such as otitis media, orthodontic problems, speech disorders, deleterious oral habits in children and possible psychosocial problems. This pathology is characterized by a single decomposition pattern that begins with the main deciduous incisors followed by deciduous molars in order of eruption [21].
The present study found that of the 557 children, 59.61% had early childhood caries (332 children). In Ecuador, there are no official records of early childhood caries from the Ministry of Public Health, they only offer epidemiological data on children under 15 years of age, where 6-year-old children reporting an average of 79.4% of missing, decayed and filled teeth [17], while the World Health Organization affirms that children of school age present 60 to 90% of dental caries. Therefore, the results of this study are relevant to highlight the prevalence of this disease in Ecuador.
The results of this research are in agreement with the study by Valarezo e Mariño [19] that evaluated the prevalence of early caries in four daycare centers in the Quito-Ecuador population in 420 infants aged 1-4 years in 2009. In this study, it was reported that 51.90% of children had early childhood caries.
Compared with other countries, there is a trend of high prevalence of early caries, similar to Peru that is 62.3% [22], in Mexico 59.5% [23], in Argentina 87.5%, [24]in Colombia is 83%, [25] in Uruguay 74% [26], in China, 47% [27], and in India, 41.9% [12].
However, in countries such as Chile, it is 20.3%, England and Sweden have between 1% and 17% prevalence rates, [28] in Germany 10% [29], in the USA and in Brazil, it is approximately 20% [30]. The low prevalence of dental caries in developed countries is due to the implementation of intervention programs, which should be considered in developing countries also. Increased fluoride consumption was the most likely cause of reduced dental caries in most industrialized countries [31].
The results indicated that the general dmft index is 1.21 for boys and 1.28 for girls. According to the level of severity reported by the World Health Organization, it is at low-risk level (1.20-2.60). These rates are less than those published by Valarezo and Mariño [19], where the rate is 2.50. A lsothe study by Chavarria et al. [25], evaluated the prevalence of carious lesions in 589 children of 32 and 52 months in the city of Villacencio-Colombia, identifying a dmft index of 2.0.
Previous studies have suggested that children with a moderate risk of early caries may require the reestablishment of progressive and cavitated lesions, whereas lesions of proximal white spots and enamel should be treated by preventive techniques, controlling the progression of the dental condition [28]. The findings of the present study show that there is a decrease in the prevention of early childhood caries, which is due to the fact that neither parents, who are responsible for educating them nor the public health system of the country are supporting to eliminate the disease [32, 33]. The diet, fluoride exposure and socioeconomic status were not evaluated or compared in the present study. However, it is known that, unfortunately, the children evaluated did not have exposure to fluoride, and their socioeconomic status was also low. Parents were young and had almost no knowledge about tooth decay, therefore, the future objective of the university where the study was conducted is to educate parents.
During the comparison of the results, it was found that the largest number of infants affected by early caries was of males, being 53.92%, compared to the girls, 46.08%, although there was no relationship between gender and prevalence of dental caries. Similar results were found in previous studies [19, 33, 34].
It is important to note that, although there was no relationship between early caries and gender, dmft was higher in girls (1.28) than in boys (1.21). This indicates a greater involvement of deciduous teeth with an indication of missing and filled teeth in girls. These findings agree with other studies [35], which described the prevalence of caries in daycare centers in Cartagena, and found that girls had dmft of 2.94 ± 3.28 and boys had dmft of 2.50 ± 3.55.
The authors state that the differences in caries rates between the girls and the boys are partially explained by the age limit of the study groups where the eruption of some types of caries occurs. In addition, the girls present a sequence of events of the dental eruption in younger ages in relation to boys, thereby the teeth of the girls have a longer time of exposure to the risk of caries; however, the age factor contributes only partially to the explanation of the variance in caries behavior [36].
The mean age of children affected by early childhood caries is 2.83 ± 0.91 years, and children of 2, 3 and 4 years of age have the highest percentage of caries with 35.54%, 34.94% and 22.59% respectively, those with a lower risk of caries are 1 and 5 years old children . Age, in this study, was a factor related to early childhood caries, the literature corroborates these findings [23]. This association is due to the fact that older childrenconsume sugary foods as compared to younger infants (1 year) and the older the child's age, the greater the risk of caries, because children are more exposed to several determinants and an additional dental eruption [37].
The highest incidence of caries occurred in the present study in children of 2 and 3 years of age, contrary to the literature [6, 14]. This can probably be explained by the fact that younger children up to 3 years of age breastfeed more or take more bottles, and brush their teeth less, and have less motor coordination. From age 3, motor coordination improves, they rely less on the bottle and breastfeed, and are able to express themselves better. In this way, they are able to express pain better, and when they present caries, they complain of pain and make their parents seek dental treatment, thus reducing the prevalence of caries.
The age at which early childhood caries occurs is of great importance, since children with this disease in the first years of life are prone to experience this situation when their permanent teeth erupt [38], and therefore, corrective and preventive measures are necessary to prevent the spread of this disease, such as educating the population to maintain adequate oral hygiene, non-cariogenic foods, and encouraging them and their family members as promoters within the community. In addition, it is necessary to continue studies of caries prevalence in early childhood, to keep a record of this pathology and the consequences on the oral health of infants, to instill the importance of deciduous dentition in parents and also the sequelae of dental caries in the long term.
CONCLUSION
The prevalence of early childhood caries in children attended in the Metropolitan District of Quito, corresponds to 59.61% of the sample analyzed.
The general dmft index of early childhood caries in children from 1 to 5 years of age in the Metropolitan District of Quito shows a medium level of severity according to the classification of the World Health Organization, with girls presenting a higher level of risk than the boys.
Children more affected by early childhood caries are those of 2 years, followed by 3 and 4 years, stating that the age of the children is related to the pathology studied.
Boys presented more early childhood caries than girls; however, the statistical test did not establish a significant relationship between gender and early childhood caries.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee in Human Research of the Ingá Faculty (Code Number: 9159/2).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013 (http://www.wma.net/ en/20activities/10ethics/10helsinki/)?
CONSENT FOR PUBLICATION
Informed consent was signed by parents or legal guardians.
AVAILABILITY OF DATA AND MATERIALS
The data sets analyzed during the current study are available from the corresponding author (Dr. Karina M. S. Freitas) on request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

