All published articles of this journal are available on ScienceDirect.

Evaluation of Knowledge, Attitudes and Oral Health-related Nutritional Performance of Diabetic Patients Referred to the Diabetes Research Center in Isfahan-Iran, 2016
Abstract
Background:
Type II diabetes is a chronic disease, with an ever-increasing incidence, concomitant with an increase in the number of the elderly. It is one of the conditions that can affect the orodental health. In general, the diabetes-related oral problems include dental caries, xerostomia, oral candidiasis, periodontal diseases and consumption of inappropriate foodstuff.
Objective:
The aim of this study was to evaluate knowledge, attitudes and oral health-related nutritional performance of diabetic patients referred to the diabetes center research in Isfahan-Iran, 2016.
Methods:
In the present cross-sectional study, 362 diabetic subjects (142 females and 220 males) referred to the Research Center for Endocrine Glands and Metabolism in Isfahan, were evaluated after being selected by simple random sampling technique. The frequency distribution of demographic data (gender, marital status, occupation, affliction with orodental diseases, disease history, and use of medications and supplements) were evaluated. The relationships of the variables above and the knowledge, attitude and performance scores of the subjects were evaluated. Data were analyzed with independent t-test, Pearson’s correlation coefficient and Spearmen’s correlation coefficient.
Results:
There were no significant relationships between orodental diseases and the mean scores of knowledge, attitudes and performance of the subjects. The mean scores of knowledge, attitudes and performance of the subjects were 33.8 ± 11.2, 53.311.01 and 53.7 ± 6.9 out of 100, respectively.
Conclusion:
The oral-health related nutritional knowledge of diabetic subjects was poor. Programs should be prepared to improve the knowledge and oral health-related nutritional performance of diabetic patients.
1. INTRODUCTION
Type II diabetes mellitus is a chronic disease in which the body is unable to use and store glycogen, and glucose returns to blood stream instead of being converted into energy, resulting in various symptoms and signs [1]. This type of diabetes mostly affects individuals over 40 years of age, who are obese and have a family history of diabetes. However, unfortunately, it should be pointed out that currently, the number of younger individuals who are affected is on the increase due to life style [2].
The incidence of type II diabetes mellitus is constantly increasing and the number of the elderly in the community in increasing concomitant with it [3]. The elderly population is at risk for diabetes, resulting in concerns for physicians in relation to the provision of health services in the elderly with diabetes. Based on the 2014 statistics in Iran, the number of diabetic patients in age range of 20-79 years has been estimated at 4.5 million people [4]. Hyperglycemia might lead to dehydration, cognitive and visual disturbances and functional compromise [5].
Diabetes is one of the diseases that might affect the orodental health. This effect is so prominent that even dentists can play an important role in the diagnosis of diabetes. This condition has been one of the most common causes of mortality in the recent years. Therefore, patients with diabetes should be several times more active in taking care of their teeth and gingival tissues [6].
The diagnosis of diabetes in medicine is made through general tests and in dentistry using oral signs such as gingivitis, periodontitis, fungal infections and a delay in the healing of oral ulcers. Therefore, dentists can play an important role in the diagnosis of diabetes and referral of patients to treatment centers [7].
Subjects with diabetes run a higher risk for periodontal diseases compared to healthy individuals [8]. In addition, these patients have a higher rate of dental caries and xerostomia. Periodontal diseases consist of gingival and tooth-supporting bone infections [9]. The best protection against periodontal diseases is proper control of diabetes. In this context, the majority of complications, including gingival diseases, are prevented by proper control of diabetes [10].
One of the complications of diabetes is an increase in vascular thickness, which might increase the risk of gingival disease [11]. On the other hand, bacteria grow well on sugary substances and poor control of diabetes might contribute to bacterial growth and initiation of gingival disease. In addition, xerostomia is one of the most common complications of diabetes, facilitating bacterial proliferation through a decrease in salivary flow [12].
Generally, the diabetes-related problems in the oral cavity include dental caries, oral candidiasis, xerostomia [13], periodontal diseases and consumption of inappropriate foodstuff [14].
In relation to the oral health-related nutritional performance, two basic considerations should be taken into account. The first is the fact that unfortunately in the course of care and treatment of diabetes, the patients' orodental health and nutritional performance draw inadequate attention. The second is the fact that in recent decades the nutrition pattern of the majority of societies have changed and unhealthy nutrition behaviors have increased significantly due to changes in life styles, and in some cases such patients consume inappropriate foodstuff for diabetes since they have no other choice, which exacerbates orodental diseases in diabetic patients [15]. Very limited studies available at present on the role of knowledge and nutritional performance in diabetic patients; however, in a cross-sectional study by Seyyed Moallemi et al., the mean knowledge scores of university students in relation to carcinogenicity of various food items and the role of nutrition in oral health were 31.2 ± 7 (of 48) and 4.7 ± 1.5 (of 8), respectively. The mean score of oral health-related performance of university students was 15.44 ± 4.3 (of 32), with no significant difference between the students of two universities [16].
Therefore, it is necessary to evaluate knowledge and orodental health-related nutritional performance in diabetic patients. The present study was undertaken to evaluate knowledge and oral health-related nutritional performance of diabetic patients referred to the Research Center for Endocrine Glands and Metabolism in Isfahan so that it would be possible to determine weak and strong points of diabetic patients in the community and the related factors to finally prioritize educational subject matters for promotion of knowledge and performance of such patients.
2. MATERIALS AND METHODS
2.1. Sample Collection
In the present cross-sectional study, the subjects were selected from diabetic patients referred to the Research Center for Endocrine Glands and Metabolism in Isfahan from January 2016 to September 2016, based on inclusion and exclusion criteria. The sample size was estimated at 362 subjects using the formula used to estimate sample sizes for prevalence studies, which showed below [17]. The inclusion criteria consisted of affliction with type II diabetes mellitus, ability to read and write, and an interest in participating in the study; the exclusion criteria consisted of affliction with other systemic conditions and provision of no responses to the questions on the questionnaire. Then questionnaires were completed on demographic data and on nutrition and knowledge through interviews. The protocol of the present study was approved by the Ethics Committee of Isfahan University of Medical Sciences. All the subjects signed informed consent forms after they were given adequate written and oral information about the aims of the study and the procedural steps.
 |
2.2. Data Collection
The questionnaires on demographic data (age, gender, marital status, use of tobacco, disease history, medical history, educational level, occupation, use of supplements and medications) and nutrition were completed for all the subjects. The questionnaire consisted of 2 sections as follows:
A: Oral health-related nutritional knowledge: 1) Knowledge about cariogenic foodstuff: A list was prepared of 24 foodstuff in terms of their sources and the frequencies of their use in the community as snacks or main meals so that knowledge about their cariogenicity could be evaluated using the three choices of “highly cariogenic”, “not cariogenic” and “I do not know”. 2) Knowledge about the role of nutrition in oral health: A total of 8 questions were related in this section to the students knowledge about the role of nutrition in oral health, using three options of “correct”, “incorrect”, “I do not know”. In order to analyze data, each correct response was given a score of “1” and each wrong response and “I do not know” were given a score of zero. Finally, the total score of the questions (from zero to 8) was calculated and then the total mean was calculated.
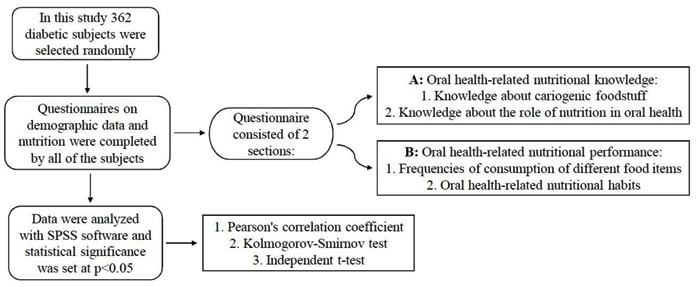
B: Oral health-related nutritional performance: 1) The frequencies of consumption of different food items: To evaluate food intake the frequencies of the use of 16 different food items were evaluated. The frequency distributions (percentages) were calculated for data analysis. 2) Oral health-related nutritional habits: A total of 8 questions were used, with choices of “always”, “mostly”, “sometimes”, “seldom” and “never” to evaluate oral health-related nutritional habits. This section was prepared with the use of questionnaires available, on nutrition and an article on nutrition and oral health (Fig. 1).
2.3. Statistic Analysis
In order to analyze data, after aligning the questions a score of zero was assigned to a completely incorrect performance, with a score of 4 to a completely correct performance. Then the total score of these 8 questions (from zero to 32) and the total mean score were calculated. Data were analyzed with IBM-SPSS for windows version 20.0 (SPSS Inc., Chicago, IL) and statistical significance was set at P<0.05. Kolmogorov-Smirnov test was used to evaluate normal distribution of data before selecting any statistical test for quantitative variables. Independent t-test was used to compare smoking, affliction with orodental diseases, use of supplements and medications, occupation and marital status as normal quantitative variables. Pearson's correlation coefficient was used to determine the linear correlation between quantitative variables (knowledge, attitude and performance scores), and Spearman’s coefficient was used to determine the correlation between quantitative variables (knowledge, attitude and performance scores) and educational levels.
3. RESULTS
After excluding un-responded questionnaires or those with incomplete responses the following data were collected. 362 subjects included in the study, which 142 (39.2%) were female and 220 (60.8%) were male. The subjects had an age range of 30-63 years, with a mean age of 46.6 ± 4.2 years. Other demographic charactristics are presented in Table 1. Of all the subjects, only 62 (17.1%) were smokers and 292 (80.7%) exhibited orodental diseases. Apart from diabetes, 274 (75.7%) of the subjects had a history of cardiovascular, hepatic and renal diseases. The mean knowledge, attitude and performance scores of the subjects were 33.8 ± 11.2, 53.3 ± 11.01 and 53.7 ± 6.9 out of 100, respectively.There was an inverse relationship between the subjects' age and attitude scores (P = 0.03, r = -0.112); however, there were no significant relationships between knowledge and performance scores and age (P > 0.05). There were no significant relationships between the mean knowledge (33.3 ± 11.3), attitude (54.1 ± 10.7) and performance (53.5 ± 6.9) scores and gender (P > 0.05). There were no significant differences in the mean knowledge (33.8 ± 11.2), attitude (33.9 ± 11.01) and performance (53.5 ± 7.3) scores between single and married subjects (P > 0.05). There were no significant relationships between the mean knowledge (34.1 ± 11.1), attitude (52.9 ± 10.9) and performance (53.8 ± 7.02) scores and the subjects’ orodental diseases (P > 0.05). There were no significant relationships between the mean knowledge and performance scores and the subjects’ occupation (P > 0.05); however, the mean attitude scores of the employees (56.04 ± 11.8) were significantly higher (P = 0.03). There were no significant relationships between the mean knowledge (33.7 ± 11.1), attitude (53.1 ± 10.8) and performance (53.9 ± 6.9) scores and use of supplements and medications (P > 0.05). There were no significant relationships between the mean knowledge (34.3 ± 12.5), attitude (52.5 ± 10.6) and performance (53.9 ± 6.5) scores and smoking (P > 0.05). Evaluation of the frequency distributions of the use of different food items (in percentages) by the patients showed that the most frequently consumed food items were soft drinks, jam, fried chicken, cheese puffs, sweetened tea and natural fruit juices, and the least frequently consumed food items were milk, fruits, sugar-free chewing gums, bitter tea and nuts, respectively (Table 2).
4. DISCUSSION
Based on the results of the present study, there were no significant relationships between the mean knowledge, attitude and performance scores of the subjects and their orodental diseases. The knowledge of patients with type II diabetes was deemed weak in terms of mean knowledge scores; on the other hand, the mean performance and attitude scores were moderate in terms of the role of nutrition in oral health. The present study showed that the mean performance and attitude scores of the subjects were moderate in terms of the role of nutrition in oral diseases, considering the consumption of food items by the patients. The mean scores of the patients consumption of food items such as French fries, cheese puffs, industrial fruit juices, soft drinks and sweetened tea indicated a low level of knowledge on nutritional-related oral diseases, which might be attributed to the fact that the majority of individuals believe that natural food items are thoroughly healthy. On the other hand, the direct relationship between the educational level and knowledge, attitude and performance scores of the patients might indicate the fact that the choice of food items can have a great effect on oral health. Neamatollahi et al., showed the effect of education on health-related knowledge [18].
| Variable | No (n=362) | Percentage (%) |
|---|---|---|
| Gender | ||
| Female | 142 | 39.2 |
| Male | 220 | 60.8 |
| Total | 362 | 100 |
| Marital status | ||
| Single | 97 | 26.8 |
| Married | 265 | 73.2 |
| Total | 362 | 100 |
| Educational level | ||
| Some high school education | 160 | 44.2 |
| High school graduate | 101 | 27.9 |
| University/college | 101 | 27.9 |
| Total | 362 | 100 |
| Occupation | ||
| Self-employed | 185 | 51.1 |
| Employee | 177 | 48.9 |
| Food Item | Seldom or Never | 1-3 Times a Month | 1-3 Times a Week | More than 5 Times a Month | 1-2 Times a Day | 3-4 Times a Day | More than 5 Times a Day |
|---|---|---|---|---|---|---|---|
| Nuts | 18.2% | 34.9% | 22.9% | 15.5% | 3.3% | 2.2% | 3% |
| French fries and cheese puffs | 31.2% | 21.8% | 21.3% | 16.9% | 1.9% | 3.6% | 3.3% |
| Jam | 24.3% | 25.4% | 17.1% | 17.4% | 8.6% | 1.7% | 5.5% |
| Honey | 21% | 19.1% | 20.7% | 20.4% | 9.4% | 7.7% | 1.7% |
| Fresh vegetables | 10.7% | 20.4% | 26% | 21% | 9.1% | 6.4% | 6.4% |
| Industrial fruit juice | 16.3% | 22.7% | 21.8% | 20.2% | 7.7% | 4.7% | 6.6% |
| Natural fruit juice | 29.3% | 19.6% | 15.7% | 18% | 6.9% | 5.5% | 5% |
| Soft drink | 33.4% | 35.6% | 10.8% | 10.2% | 5.6% | 2.2% | 2.2% |
| Sugar-free tea | 27.6% | 24.6% | 20.7% | 13.3% | 6.6% | 2.8% | 4.4% |
| Sweetened tea | 24.3% | 20.7% | 21.5% | 18% | 8.8% | 3.9% | 2.8% |
| Fresh fruits | 16.6% | 22.9% | 20.4% | 19.1% | 11.6% | 6.6% | 2.8% |
| Milk | 15.8% | 19.1% | 19.6% | 19.9% | 14.6% | 7.7% | 3.3% |
| Cheese | 11.9% | 17.1% | 23.2% | 22.4% | 8.3% | 9.9% | 7.2% |
| Pastry, cakes and biscuits | 17.1% | 25.1% | 15.2% | 17.4% | 13.3% | 5.5% | 6.4% |
| Conventional chewing gum | 23.5% | 23.5% | 16.9% | 14.4% | 12.7% | 5.1% | 3.9% |
| Sugar-free chewing gum | 36.7% | 19.6% | 10.8% | 10.8% | 10.2% | 3.9% | 8% |
Recent studies have shown the important role of nutrition in health and prevention of non-communicable diseases such as metabolic syndrome, cardiac diseases and orodental diseases given the diversity of food items. The majority of studies have shown that the diversity of food items is affected by nutritional culture [19].
Studies have shown a direct relationship between diabetes and oral diseases. Therefore consumption of food items that have a role in disorders of blood glucose levels might income the risk of oral diseases [15]. For this reason, the present study showed that the use of food items (which may have played a role in) exacerbating the condition, with a mean knowledge score 33.6.
The percentage of the use of food items such as French fries, cheese puffs, jam, soft drinks, sweetened tea, pastry, cakes and biscuits was higher than other food items, confirming the results of a study by Hosseyni Esfahani et al., in which an increase in the consumption of French fries, biscuits, chewing gum, different kinds of industrial sweet drinks and pastry that resulted in an increase in consumption of sugar and a decrease in consumption of fruits and vegetables [20]. However, nutritional guidelines recommended the consumption of at least four units of fruits and 5 units of vegetable, which contribute to both the general and oral health [21].
Given the mean performance score of the patients and the frequency of consumption of milk and sugar-free tea, milk might be considered a proper alternative for cariogenic drinks [16]. The preventive effect of cheese on dental caries has been shown in human experimental and interventional studies. Milk contains calcium, phosphorus and casein, which inhibit caries and promote oral health.
Food items that promote salivation, including nuts, cheese and sugar-free chewing gum, are considered protective factors against dental caries [22]. There was no significant relationship between the knowledge and performance score of the subjects and their occupation; however, the mean attitude score of employees was significantly higher. It appears employed subjects exhibit a higher level of readiness to promote their knowledge through correct education due to a high level of social contacts. Another study reported a significant relationship between occupation and knowledge [23].
In a study, Ajami et al., showed a significant relationship between oral health-related knowledge and educational level (P = 0.004); in this context, physicians exhibited the highest knowledge level and those with associate degrees exhibited the least [24]. There was an inverse relationship between the patients’ age and attitude scores (P = 0.03, r = -0.112); however, there was no significant relationship between the patients’ age and knowledge and performance scores, indicating the fact that health beliefs are affected by various factors. The present study showed that the highest level of knowledge and good attitudes were exhibited by married, employed subjects, indicating the fact that after the subjects begin their joint life subsequent to marriage, they make attempts to increase their knowledge in all the fields, including in the field of health and prevention of oral and dental diseases [24].
In a study Eldarrat evaluated diabetic subjects at an age range of 17-78 years, reporting that patients with diabetes lead a low level of knowledge about the increased risk of orodental diseases compared to other subjects. In this context,attempts should be made in dental and medical fields in order to increase the patients knowledge [25]. In another study, Marshal et al., showed that consumption of calcium and folate in subjects with sound teeth, who were obliged to observe orodental health, was higher [26]. Also, Smiciklas-Wright et al., showed that inadequate intake of vitamins A, C and B6 might lead to auditory, immune, cardiovascular and oral health-related disorders [27]. A study by Allen et al., on the attitudes of diabetic patients in relation to the effect of diabetes on the quality of life showed that knowledge about the increased risk of periodontal diseases in the diabetic group was low, especially compared to their knowledge about other complications of diabetic. This study showed that diabetes had a moderate effect on the quality of life and dissatisfaction with nutritional status. In addition, this study showed that diabetic patients had limited knowledge about the effect of the oral health on the body’s general health. Less than half of the subjects had referred to a dental office in the previous year and less than one-third of the subjects who had referred to a dentist during the previous 5-year period had more knowledge about the risk of dental diseases. The oral health-related quality of life did not exhibit unfavorable effects in the presence of diabetes, with effects on the selection of food items and their satisfaction [28].
One of the strong points of the present study was the large sample size. The chief limitation of the present study was its cross-sectional design; such designs prevent determination of a cause-and-effect relationship. Therefore, it is necessary to evaluate the possible cause-and-effect relationship. It is recommended that cohort and prospective studies be carried out to determine cause-and-effect relationships.
CONCLUSION
The diabetic subjects in the present study exhibited a low level of oral health-related knowledge of nutrition. It is recommended that programs be prepared to promote knowledge and oral health-related performance of diabetic patients.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Ethical Committee of Isfahan, University of Medical Science. This clinical trials code is (IRCT) IRCT2016012626209N1.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008 (http://www.wma.net/en/20activities/10ethics/10helsinki/).
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patients for publication of this study.
AVAILABILITY OF DATA AND MATERIAL
The data sets analyzed during the current study are available from the corresponding author on request.
FUNDING
Funds of this project paid with Isfahan University of Medical Sciences, Isfahan, Iran.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors thank the participants for taking part in this study.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publishers Website along with the published article.

