All published articles of this journal are available on ScienceDirect.

Rotary Instrument in Non-Surgical Treatment of Chronic Periodontal Disease: Clinic Randomized Study
Authors Info & Affiliations
Abstract
Objective:
The aim of this study is to compare the efficacy of rotary instruments vs hand scalers in non-surgical periodontal therapy, studying the variation of periodontal health indexes.
Materials and Methods:
Forty patients (age between 30 and 70 years) with advanced chronic periodontitis, that were recruited for the study, were divided into two groups; control group and test group. Control patients were treated with hand scalers while test group patients were treated with rotary instruments. Periodontal indexes were evaluated at baseline and after 3 months.
Results:
Nonsignificant differences were found at 12 weeks follow up for all the parameters between test and control groups.
Conclusions:
Within their limits, the results indicate that different instruments can be effective in removing calculus and endotoxins. This requisite is mandatory for a proper periodontal healing.
The reasons for clinicians to use diamond-coated instruments are related to a faster procedure, and the clinical evidence of a smooth root surface. The clinicians’ ability remains one of the most important variables that could affect periodontal therapy.
1. INTRODUCTION
Periodontal disease is a chronic inflammatory infection that leads to the destruction of the teeth supporting tissues, with a progressive loss of connective tissue attachment and bone resorption [1].
The pathogenesis of periodontal disease is characterized by a complex relationship between microorganisms in dental biofilm (plaque) and the host immuno-inflammatory response [2]. This response may be influenced by genetic factors, environmental and / or acquired conditions, such as smoking and systemic diseases [3, 4].
The periodontal disease is also described as a modifying factor of systemic health and its clinical relevance can exert an impact on the quality of life in the form of emotional, social and functional aspects, as well as being relevant in acute processes [5, 6].
Bacterial plaque and calculus are recognized as the etiological agents of the periodontal disease that along with a rough tooth surface can facilitate bacterial adhesion to the tooth and the root [7-9].
For this reason, the aim of periodontal therapy is the reduction of a specific sub-gingival gram-negative anaerobic organism by the removal of calculus, plaque and contaminated root cementum [10, 11].
Periodontal therapy can be broadly classified as surgical and non-surgical. Non-surgical therapy is nowadays executed with hand scalers and ultrasonic scalers.
Ultrasonic scalers have become more widely used in recent years because they are easy and fast to use, when compared to hand scaler, but SEM evaluation reported a difficulty to achieve a smooth and calculus free surface [12, 13]. However, hand scalers are unable to decontaminate root surfaces properly when the periodontal pockets are more than 4 mm deep [14].
To overcome these difficulties, associated with hand instrumentation and ultrasonic scalers, rotary instrument was introduced in periodontal treatment for scaling and root planning [15, 16].
The aim of the present investigation is to compare the efficacy of rotary instruments compared to hand scalers in non-surgical periodontal therapy.
2. MATERIALS AND METHODS
2.1. Study Population and Methodology
All the patients were recruited from the Department of Periodontology of the University of Naples Federico II. The ethical committee approved the study protocol and all participating patients signed an informed consent at the beginning of the study.
2.2. Selection of Subjects
40 patients (age between 30 and 70 years) with a diagnosis of advanced chronic periodontitis were selected for the study [17, 18].
The inclusion criteria for patient selection were:
- Adults between 18 and 70 years;
- Patients with at least 20 teeth;
-
Patients with at least 5 sites with:
- Probing depth (PD) ≥ 5mm;
- Clinical attachment level (CAL) ≥ 3;
The exclusion criteria were:
- Patients undergoing periodontal treatment during the last 2 years;
- Patients using antibiotics for 6 months prior to treatment;
- Patients with any systemic disease;
- Patients using medicated mouthwashes;
- Pregnancy;
- Smokers (≥10/die).
2.3. Study Design
Forty patients with generalized advanced chronic periodontitis, who fulfilled all the prerequisites, were recruited for the present study. Patients underwent a screening examination, which included full mouth probing (six sites for every tooth), and an intraoral radiographic examination. All subjects were enrolled in a hygiene program two weeks prior to the treatment. They received professional supra-gingival tooth cleaning with ultrasonic scalers (supra-gingival ultrasonic tip) and oral hygiene instructions (baseline) [19, 20] (Fig. 1).

Patients were randomly divided into two groups; control group and test group. Control patients were treated with hand scalers while test group patients were treated with rotary instruments.
2.4. Randomization of the Study
Examiner (A) conducted the screening test and the final recruitment. The 40 patients were randomly assigned to the groups using random tables. The second examiner (B) kept the randomization list, and the patients were given sealed envelopes indicating the treatment modality. Examiner (C) opened those envelopes and performed the therapy. Examiner (A), who was unaware of the treatment received, performed the recording of all clinical parameters. Finally, examiner (B) compiled the data received from examiner (A) according to the randomization list. At all-time points, the outcome of research was assessed blindly.
The following manual instruments were used in this study:
- Gracey SG 7-8 (Hu-Friedy Mfg. Co., LLC Chicago, IL - USA);
- Gracey SG11/12 (Hu-Friedy Mfg. Co., LLC Chicago, IL - USA);
- Gracey SG13/14 (Hu-Friedy Mfg. Co., LLC Chicago, IL - USA);
- Periodontal Probe North Carolina (Hu-Friedy Mfg. Co., LLC Chicago, IL - USA).
The following mechanical rotating instruments were used:
- Diamond bur 740 with40 µm graining (Red) (Perio-Set, Intensiv SA, Montagnola, CH);
- Diamond bur 715 with 15µm graining (Yellow) (Perio-Set, Intensiv SA, Montagnola, CH).
The instrumentation was done under local anesthesia. The curettes were sharpened at the operator's request, no restrictions regarding the duration of the therapy were set in any group. The burs were used according to the manufacturer’s instructions, with diamond bur 740 first, and then with diamond bur 715, using right angle hand piece, at rotation speeds of 6000 rpm, under water-cooling (Fig. 2).
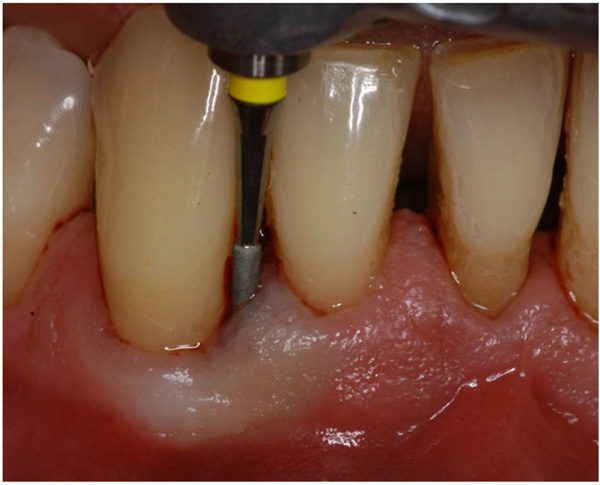
During the surface treatment, attention was paid to maintaining uniform pressure.
After the treatment, follow-up was performed at 12 weeks, and oral hygiene instructions were repeated (Fig. 3).

The clinical periodontal indexes recorded were the Periodontal Depth (PD), the gingival Recession (REC), the Full Mouth Plaque Score (FMPS) and Full Mouth Bleeding Score (FMBS).
2.5. Statistical Analysis
The statistical analysis was performed using NCSS-PASS (Number Cruncher Statistical System) software. F-Fisher’s test was carried out to verify the age distribution between the two groups, while Chi-square was performed to evaluate the gender distribution. The clinical indexes REC and CAL are expressed in mm, while FMPS and FMBS are expressed in percentage. All indexes were executed using mean values and standard deviations. Kolmogorov-Smirnov test was performed to evaluate the distribution of defects among the groups considering the PD, CAL and REC indexes. The intra-group comparative analysis was performed using a paired t-test, while for the inter-group, comparative analysis was done using an unpaired t-test. The frequency distribution of results, considering the pocket depth reduction and the clinical attachment level was evaluated using Mantel-Haenszel test. For all tests, a p-value of 0.05 is considered as statistically significative.
3. RESULTS
The baseline data are reported in Table 1; there were no significant differences for all the parameters between the test group and control group.
| - | CAL | PD | REC | FMPS | FMBS |
|---|---|---|---|---|---|
| Test group | 8 ± 1.17 | 4.74 ± 1.10 | 3.26 ± 0.87 | 21.16 ± 11.94 | 84 ± 0.37 |
| Control group | 8.05 ± 1.45 | 4.63 ± 1.50 | 3.42 ± 0.84 | 16.84 ± 3.66 | 79 ± 0.42 |
| P-value | 0.978 | 0.889 | 0.577 | 0.552 | 0.789 |
Table 2 shows periodontal indexes respectively of test and control group at 12 weeks follow-up. There were no significant differences for all the parameters between the test group and control group.
| - | CAL | PD | REC | FMPS | FMBS |
|---|---|---|---|---|---|
| Test group | 7.05 ± 1.33 | 2.95 ± 1.18 | 4.1 ± 0.60 | 12.53 ± 8.83 | 34 ± 0.30 |
| Control group | 7.27 ± 1.52 | 3.47 ± 1.58 | 3.8 ± 0.67 | 10.74 ± 2.83 | 31 ± 0.23 |
| P-value | 0.169 | 0.127 | 0.762 | 0.209 | 0.342 |
Table 3 shows a comparison between the 3 months follow-up indexes and the baseline of the test group; A significant reduction of PD, CAL, REC, FMPS and FMBS values is shown.
| - | CAL | PD | REC | FMPS | FMBS |
|---|---|---|---|---|---|
| Baseline | 8 ± 1.17 | 4.74 ± 1.10 | 3.26 ± 0.87 | 21.16 ± 11.94 | 84 ± 0.37 |
| 3 months | 7.05 ± 1.33 | 2.95 ± 1.18 | 4.1 ± 0.60 | 12.53 ± 8.83 | 34 ± 0.30 |
| P-value | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 |
Table 4 shows a comparison between the 3 months follow-up indexes and baseline of the control group. After 12 weeks, a statistically significant difference for PD, CAL, REC, FMPS and FMBS values, was evident.
| - | CAL | PD | REC | FMPS | FMBS |
|---|---|---|---|---|---|
| Baseline | 8.05 ± 1.45 | 4.63 ± 1.50 | 3.42 ± 0.84 | 16.84 ± 3.66 | 79 ± 0.42 |
| 3 months | 7.27 ± 1.52 | 3.47 ± 1.58 | 3.8 ± 0.67 | 10.74 ± 2.83 | 31 ± 0.23 |
| P-value | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 | ≤ 0.05 |
4. DISCUSSION
The aim of the present investigation is to compare the efficacy of rotary instruments to hand scalers in non-surgical periodontal therapy.
The purpose of this study is linked to the common opinion that mechanical instruments are easier to use, while hand-scaling technique is more difficult to be learned, properly executed and requires more time to be performed. If rotary instruments have the same or a better effectiveness, it could be a valid alternative to curettes in periodontal therapy.
Mengel et al., reported that the mechanical rotating instruments produced a homogeneous surface, when compared to the manual instruments, however, the SEM images revealed the presence of a marked smear layer [21].
Parma-Benfenati et al., in an earlier study, attested that the curette was the most suitable instrument for producing a smooth and clean root surface, while Mamoru Kishida et al., reported the opposite, but underlined the use of mechanical rotating instrument to be faster than curettes [7, 22].
Our clinical experience confirms that the use of mechanical rotating instruments is faster than manual instrumentation resulting in a shorter periodontal treatment. Schwarz JP et al., concluded that there are no significant differences related to the level of cleanliness achieved by hand versus rotary instrumentation, except that some residual bacterial deposits could be identified, in small lesions (10 μm) on the roots, more often on surfaces instrumented by the Gracey curettes [23].
Dahiya et al., showed how the use of rotary instruments in chronic periodontal disease treatment gives comparable results with the traditional approach of scaling and root planning [16].
Schlageter et al., used mechanical rotating instruments in open flap debridement and concentrated his attention on surfaces smoothness proving that curettes as well as very fine rotating diamonds created the smoothest root surfaces [24]. Dibart et al., run an in vivo study on hopeless teeth, and then evaluated in vitro the effect on the teeth surfaces, showing how the rotating instrumentation was more effective in removing debris and plaque than the conventional Gracey curettes [25].
The present study, according to the literature studies reported, shows that there are no significant differences between manual and mechanical rotating instruments.
CONCLUSION
The presence of small bacteria-contaminated resorption lacunae in root planed areas may prevent complete elimination of periodontal pathogens from treated surfaces [26].
These conditions could affect the bacterial eradication unless being more “aggressive” on the root cementum removal [23]. The extra-fine diamond finisher bur (with 15-pm graining) can be recommended when treating inaccessible sites. However, these instruments remove more dental substance and form a thicker smear layer [21].
In conclusion, achieving an environment free surface from noxious substances is probably the most important prerequisite for periodontal healing, and this result could be reached with different instruments [24]. These two kinds of therapy seem to produce a general improvement of clinical indexes with no significant differences; however, the clinician ability remains one of the most important variables that could effect periodontal treatment [27].
The often-cited reasons for clinicians to use diamond-coated instruments are related to a shorter time-consuming therapy and provide a smoother root surface than hand instruments even when used by less-skilled clinicians [27]. Any bias, such as clinician ability, that could affect periodontal therapy could be reduced using an easier instrumentation system. Next studies should investigate clinical characteristics of these two instrumentations, in particular, which treatment could be more effective in clinical conditions where the access is more prohibitive. Further clinical and histological investigations are needed to fully evaluate microscopic effects of mechanical rotatory instruments.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was analyzed and approved by the Ethics Committee of Department of Periodontology of the University of Naples Federico II.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
All patients gave informed consent.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
All individuals listed as authors have contributed substantially to the design, performance, analysis, and reporting of the work. No others contributors to the articles that the authors accredited.

