All published articles of this journal are available on ScienceDirect.

Passive Periodontal Sensation Threshold of Upper Molars in Patients with Myofascial Pain
Authors Info & Affiliations
Abstract
Background and Objective:
The relationship between periodontal sensation and Myofascial Pain (MP) is not yet fully clarified. The aim of this study was to test the null hypothesis that there is no difference in the periodontal sensation threshold between subjects with MP and subjects with no Temporomandibular Disorders (TMD).
Methods:
Participants have clinically assessed in accordance with the Research Diagnostic Criteria for Temporomandibular Disorders version 1.0 guidelines and assigned to the MP group (mean age 54.8 ± 14.8 years; 1 male and 11 females) or the control group (mean age: 63.9 ± 13.2 years; 1 male and 15 females). The Passive Periodontal Sensation Threshold (PPST) was evaluated using impulsive mechanical stimulation on the occlusal surface parallel to the tooth axis of the maxillary first molar, if present. The difference in the mean PPST between the MP group and the control group was evaluated using the Student t-test after checking for homoscedasticity.
Results:
The mean PPST value was 1050.1 ± 480.3 mN in the MP group and 712.3 ± 288.5 mN in the control group. A significant difference was observed between these mean PPST values (p = 0.045).
Conclusion:
There was a significant difference in PPST between the MP group and the control group. Although the etiology of the change of PPST is still unknown, the higher PPST value observed in MP patients suggests that future study on occlusal dysesthesia or occlusal sensation-related pathosis is warranted.
1. INTRODUCTION
Tactile sensation in the teeth plays an important role in maintaining a sound stomatognathic system, and the properties of this function have been studied extensively [1-3]. It has been reported that some patients who suffer from Temporomandibular Disorders (TMD) experience uncomfortable occlusal sensations [4]. Clark et al., defined occlusal dysesthesia as a “persistent uncomfortable sense of maximum intercuspation after all pulpal, periodontal, muscle and Temporomandibular Joint (TMJ) pathologies have been ruled out and a physically obvious bite discrepancy cannot be observed” [5].
Sensory inputs from the muscle spindles of the jaw-closing muscles, periodontal receptors, and sensory receptors in the TMJ have been reported to have a possible relationship with occlusal dysesthesia [6]. One study found that patients with Myofascial Pain (MP) or TMJ pain showed a significantly higher threshold for occlusal thickness discrimination than that exhibited by a control group [7]. Another study found a significant relationship between MP and occlusal thickness discrimination [8]. However, the relationship between periodontal sensation and MP has not yet been fully clarified.
In human studies, a psychophysical approach has been adopted in this field because of the difficulty in recording signals directly from nerve fibers or sensory receptors in humans [9]. To achieve higher objectivity, recording of the Passive Periodontal Sensation Threshold (PPST) is considered to be an appropriate modality for the evaluation of periodontal sensation. PPST can be recorded using standardized mechanical stimulation methods [2]. For example, air-operated stimulating devices, pneumatic stimulating devices, and strain gauges have been used to evaluate PPST [9]. However, most of these devices adopted anterior teeth as the target for the evaluation, most likely because of the size and structure of the stimulation system. Komiyama et al. investigated the intraoral tactile detection threshold using the Semmes-Weinstein monofilament test [10], which is used for quantifying the sensitivity to light punctuate mechanical stimulation on the skin or mucosa [11]. The monofilaments were cut to half their length for use in the oral cavity. This short monofilament technique is an excellent method, as it does not require any special equipment. However, as it requires a lengthy application for each tooth, it seemed inappropriate to apply this method to a TMD patient in pain. Therefore, evaluation of PPST in the molar teeth of TMD patients has been difficult. Recently, Morimoto et al., described a new apparatus to evaluate PPST using a computer-regulated impulsive force with a short measuring time according to the staircase method [12], which offers the potential to be applied to the molar teeth of TMD patients.
In the present study, we measured PPST in TMD patients using the apparatus reported by Morimoto et al., following further miniaturization of the sensor head [12]. The aim of this study was to test the null hypothesis that there is no difference in the periodontal sensation threshold between patients who have and do not have MP.
2.. MATERIALS AND METHODS
2.1. Subjects
The present study was conducted from August 2014 to March 2015 in the TMD Clinic of the Clinical Division of Removable Prosthodontics and the Clinical Division of Preventive Dentistry at Okayama University Hospital. The participants were recruited from sequential patients who visited the Clinical Division of Preventive Dentistry seeking periodic oral health examinations, and the TMD clinic seeking treatment. Inclusion criteria were painless jaw opening to more than 30 mm interincisal distance and having a maxillary molar which fulfilled the following target tooth criteria: 1) at least one occlusal tooth contact point with an antagonistic tooth but without premature occlusal tooth contact; 2) no periodontal pocket greater than 3 mm; 3) no mobility exceeding the normal range; 4) no pulpal disease, periodontal disease or periapical periodontitis; and 5) not incorporated in a fixed denture prosthesis. The maxillary first molar was selected as the first choice. When the first molar was missing, the most posterior molar that fulfilled the above conditions was adopted. Subject exclusion criteria were as follows: 1) taking an antianxiety agent of benzodiazepine derivation; and 2) not obtaining informed consent.
After all, participants underwent clinical assessment in accordance with the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) version 1.0 guidelines to assign the axis I diagnosis of MP [13], two subject groups, the Myofascial Pain group (MP group) and the control group, were used in this study. The MP group consisted of 12 patients who were diagnosed with myofascial pain in the jaw closing and opening muscles (mean age: 54.8 ± 14.8 years; 1 male and 11 females); seven with unilateral MP and five with bilateral MP. The mean duration of pain in the MP group was 4.5 ± 3.4 months. The control group consisted of 16 patients asymptomatic for TMD (mean age: 63.9 ± 13.2 years; 1 male and 15 females).
All subjects received an explanation of the nature and purpose of the study, and all provided their written informed consent to participate in the study. The study protocol was approved by the Ethics Committee of Okayama University (No. 2084).
2.2. PPST Measuring Equipment
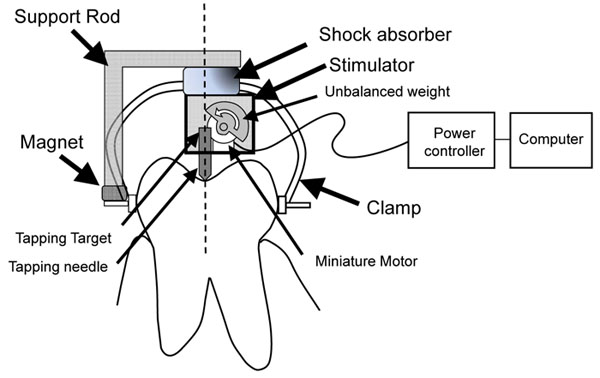
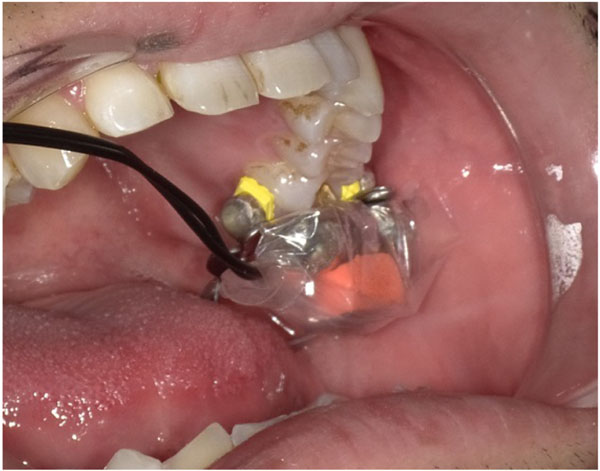
PPST was evaluated using impulsive mechanical stimulation exerted on the occlusal surface parallel to the tooth axis. Fig. (1a) shows a schematic diagram of the PPST measuring system used in this study. The stimulator consisted of a miniature motor with an unbalanced weight that hammered the tapping target. The outer size of the stimulator was 25 x 5 x 15 mm, and the weight was 2.9 g. The outer size was smaller than the stimulator reported by Morimoto et al., [12]. Before installing the stimulator, a tooth clamp (2AS Rubber Dam Clamp, Hu-Friedy Mfg Co., LLC, Chicago, IL, USA) was attached to the target tooth without touching the gingiva. The stimulator and support rod were then attached to the clamp via a magnet as shown in Fig. (1b). The measuring equipment was installed so the tapping needle contacted the occlusal surface at the central fovea, and the axis was adjusted to be parallel to the tooth axis. The tapping force featured 30 intensities ranging from 68 mN to 2720 mN, and was regulated by a voltage controlled by a computer program to generate upward and downward sequences according to the staircase method (described in the experimental section). The impulsive force was calibrated using an acceleration pickup (NP-2106, Ono Sokki Co., Ltd, Yokohama, Japan). A randomized interval from 2 to 3 s was automatically generated by the computer between stimulations to avoid the anticipation effect.
For infection prevention, the tooth clamp was sterilized for each subject and the measuring equipment was covered with a disposable sleeve.
3. EXPERIMENTAL
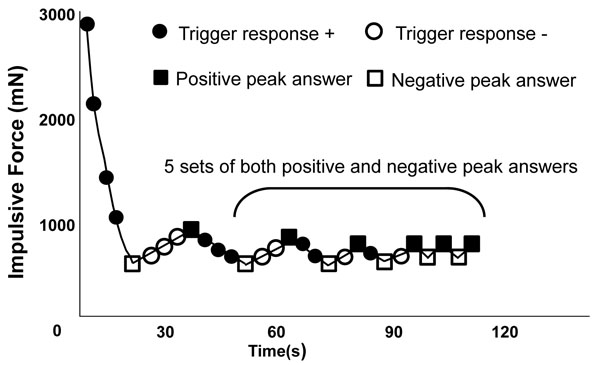
The experimental procedure took place for each subject from 9 a.m to noon in the clinic. The subject was instructed to hold the trigger switch and to turn the trigger on as soon as the impulsive stimulus was felt on the test tooth. The subject wore noise-canceling headphones playing pink noise to block any ambient noise and possible subtle noise generated by the measuring system. The subjects were instructed to sit in an upright position in a dental chair during the test procedure. Fig. (2) shows a typical trigger response to the sequential mechanical stimulation. The trigger response for the first impulsive force was regarded as a positive response, and the strength of the next impulsive force applied was one step lower according to a downward sequence. The downward sequence was automatically repeated with decreasing strength until the subject did not make a trigger response, which was recorded as a negative peak answer. By recording the negative peak answer, the sequence was turned into an upward sequence. The stimulation procedure was then automatically repeated with increasing strength until the subject made a trigger response, which was considered to be a positive peak answer. By detecting the positive peak answer, the stimulation was turned into a downward sequence again. The upward and downward sequences were repeated alternately until six sets of negative and positive peak answers were recorded.
The PPST for the tooth was calculated as the mean of the last five sets of peak values. The representative PPST value for a subject was calculated as the mean value of the measured periodontal sensation threshold for the left and right target teeth when target teeth on both sides were available. For subjects with a unilateral target tooth, the PPST value of that tooth was used as the representative PPST value of the subject.
3.1. Statistics
Differences in the mean PPST between the MP group and the control group were evaluated using the Student t-test after checking for homoscedasticity. The significance of the relationship between PPST and the age of the subjects in the two groups was evaluated using Pearson’s correlation coefficient. In the MP group, the significance of the relationship between the duration of pain and PPST was evaluated using Pearson’s correlation coefficient. A significance level of 0.05 was adopted for all statistical tests, and two-sided tests were applied. Data analysis was performed using IBM SPSS Statistics for Windows, version 19 (IBM Corp., Armonk, NY, USA).
4. RESULTS
Clinical parameters and demographic characteristics of study subjects in the MP group are shown in Table 1. Detailed information about the subjects in the control group is shown in Table 2. Among the MP group subjects, bilateral muscle tenderness was observed in five subjects, and single-side muscle tenderness was reported in seven subjects. The mean evaluation time of PPST in the MP group, from the first stimulation to the end of the staircase method, was 1.8 ± 0.5 min for the right side and 2.0 ± 0.7 min for the left side. The mean evaluation time of PPST in the control group was 2.1 ± 0.6 min for the right side and 1.9 ± 0.5 min for the left side. The mean PPST value was 1050.1 ± 480.3 mN in the MP group and 712.3 ± 288.5 mN in the control group. A significant difference was observed between these mean PPST values (p = 0.045).
| Subject No. | Age | Sex | PPST (mN) | Subjected Teeth | Time Spent for PPST Evaluation (Min) | Muscle Pain With Palpation | Duration of Pain (Months) | Unassisted Jaw Opening Without Pain (Incisal Overlap Added) (mm) | |
|---|---|---|---|---|---|---|---|---|---|
| Right Side | Left Side | ||||||||
| 1 | 31 | F | 1258.0 | 16, 26 | 1.1 | 2.2 | Bil.MM | 14 | 37 |
| 2 | 36 | F | 1229.1 | 16, 26 | 1.2 | 1.6 | Bil.MM, Bil.DM | 4 | 47 |
| 3 | 44 | M | 1703.4 | 16, 26 | 2.4 | 2.4 | Bil.MM, Bil.TM, Bil. MPM, Bil.DM | 5 | 43 |
| 4 | 47 | F | 724.2 | 16, 26 | 1.7 | 1.9 | R.TM | 3 | 37 |
| 5 | 47 | F | 1465.4 | 16, 26 | 1.7 | 1.7 | Bil.MM, Bil.DM | 3 | 36 |
| 6 | 51 | F | 774.3 | 16, 26 | 1.9 | 2.1 | Bil.MM, L.TM, L.MPM | 7 | 40 |
| 7 | 53 | F | 1658.5 | 16, 26 | 1.5 | 1.4 | L.MM, L.MPM, L. DM | 7 | 41 |
| 8 | 64 | F | 563.0 | 16, 26 | 2.4 | 1.8 | L.DM, L.SM | 1 | 47 |
| 9 | 66 | F | 1268.2 | 16, 26 | 1.8 | 1.5 | L.MM | 3 | 32 |
| 10 | 70 | F | 343.4 | 16, 25 | 2.9 | 3.7 | R.MM, R.MPM | 2 | 32 |
| 11 | 72 | F | 354.4 | 15, 25 | 1.7 | 2.1 | R.MM | 2 | 39 |
| 12 | 77 | F | 1229.7 | 16, 26 | 1.5 | 1.0 | L.MM | 3 | 33 |
| Mean (S.D.) | 54.8 (14.8) | - | 1050.1 (480.3) | - | 1.8 (0.5) | 2.0 (0.7) | - | 4.5 (3.4) |
38.7 (5.2) |
| Subject No. | Age | Sex | PPST (mN) | Subjected Teeth | Time Spent for PPST Evaluation (min) | |
|---|---|---|---|---|---|---|
| Right Side | Left Side | |||||
| 1 | 30 | F | 574.6 | 16, 26 | 1.9 | 2.6 |
| 2 | 39 | F | 380.8 | 16, 26 | 2.7 | 2.0 |
| 3 | 58 | F | 520.2 | 14, 26 | 2.7 | 2.7 |
| 4 | 59 | F | 455.6 | 16, 26 | 1.5 | 2.5 |
| 5 | 62 | F | 600.1 | 16, 26 | 1.8 | 1.8 |
| 6 | 63 | F | 531.3 | 16, 26 | 2.9 | 2.7 |
| 7 | 64 | F | 856.8 | 16, 26 | 1.5 | 1.9 |
| 8 | 67 | F | 581.4 | 16, 25 | 1.7 | 1.8 |
| 9 | 67 | M | 597.0 | 16, 26 | 2.6 | 1.9 |
| 10 | 68 | F | 396.1 | 16, 26 | 3.7 | 1.7 |
| 11 | 68 | F | 1251.2 | 17, 26 | 1.5 | 1.5 |
| 12 | 71 | F | 945.2 | 16, 25 | 1.8 | 1.7 |
| 13 | 72 | F | 746.3 | 16, 26 | 2.0 | 1.2 |
| 14 | 76 | F | 1394.0 | 16, 25 | 1.4 | 1.0 |
| 15 | 77 | F | 787.1 | 16, 26 | 2.4 | 1.7 |
| 16 | 81 | F | 778.6 | 16, 26 | 2.4 | 1.5 |
| Mean (S.D.) | 63.9 (13.2) | 712.3 (288.5) | - | 2.1 (0.6) | 1.9 (0.5) | |
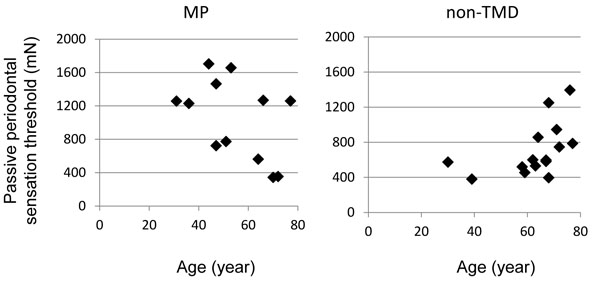
The relationship between measured PPST values for both groups and the age of the subjects is shown in Fig. (3). In the control group, PPST seemed to be related to the age of the subject, but this relationship was not statistically significant (r = 0.44, p = 0.052). No statistically significant relationship was observed in the MP group (r = 0.46 p = 0.13).
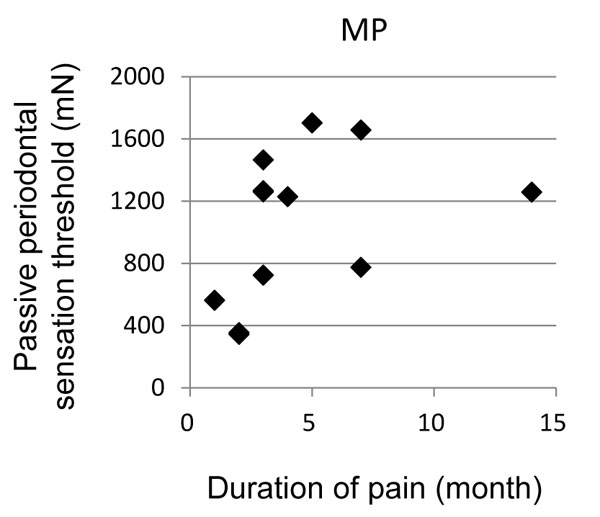
The relationship between the duration of pain and PPST in the MP group is shown in Fig. (4) PPST in the MP group had a tendency to increase with the duration of pain, but this relationship was not statistically significant (r = 0.40, p = 0.20).
5. DISCUSSION
Numerical evaluation of periodontal sensation could be of great importance in the analysis and observation of occlusion-related clinical problems. In the present study, significantly higher PPST values were observed in the MP group than in the control group. Previous studies have adopted a technique involving biting on metal blocks or metal strips to evaluate occlusal sensation in relation to myofascial pain [7, 8]. However, these evaluation methods may include sensational inputs from the muscle spindles of masticatory muscles or the mechanical receptors of the temporomandibular joint [7].
It has been suggested that jaw muscle receptors may contribute to mandibular kinesthesia [14]. Morimoto and Kawamura also suggested that muscle spindles in the jaw-closing muscles may be responsible for the discrimination of interdental thickness [15]. TMJ receptors have been reported to play an important role in positional and sensorial discrimination [16-18]. Jacobs et al., reported that the threshold for the interocclusal
detection of small objects, such as strips, may be dependent on the activity of periodontal mechanoreceptors [9].
According to these previous reports, it would be reasonable to infer that the sensory receptors in the periodontium are extremely sensitive.
Although sensory receptors in the periodontium and intradental receptors have been reported to play a role in detecting occlusal contact, Linden et al., found no significant differences in the sensory threshold for mechanical stimulation between teeth with vital pulp tissue and pulpected teeth [19]. Therefore, mechanical stimulation for each tooth is thought to be mainly perceived by the sensory receptors in the periodontium.
In the present study, an impulsive force in the form of occlusal tapping was used as the source of mechanical stimulation. As the measuring equipment used in this study was small and lightweight (2.9 g), it can be assumed that the equipment would not affect the sensational inputs from the muscle spindles of masticatory muscles or the mechanical receptors of the temporomandibular joint. Therefore, differences in the observed threshold were caused not by the differences in these related mechanoreceptors, but by the periodontal receptors.
Oki et al. reported that mechanical loading increased the periodontal sensation threshold [20], and previous studies suggested that sustained low-level masticatory muscle activity might play an important role in the etiology of temporomandibular disorders [21-24]. Considering the results of these previous studies, it could be inferred that sustained mechanical loading affects periodontal sensation. However, the etiology of myofascial pain is still controversial, and several mechanisms for the development of such pain have been proposed [25]. One study proposed a concept of Persistent Orofacial Muscle Pain (POMP), with the hypothesis that the induction of POMP involves the interplay between a peripheral nociceptive source in muscle, a faulty central nervous system component, and decreased coping ability. From the results of this study, POMP itself or the above-mentioned induction factors of POMP could affect periodontal sensation. Kleim et al., reported that neural plasticity took place at 2 to 9 months after finger trauma [26], suggesting that time course could be regarded as an important aspect of the clinical phenomena in relation to neural plasticity. In the present study, the duration of pain was recorded in relation to PPST. Although a slight trend was noted, no significant relationship was observed between the duration of pain and PPST. Further investigation of this relationship could yield additional information about this important aspect of occlusal dysesthesia.
As a limitation of the present study, the following three items are conceivable. First, subjects with severe limitation of jaw opening were excluded from this study. Although the size of the outer shell of our equipment was improved to be much smaller than the one reported by Morimoto et al. [12], subjects in the MP group with a maximal pain-free jaw opening of less than 30 mm were excluded from the study. Because the PPST of patients with severe MP would be of great interest, this limitation needs to be overcome in future studies. Second, the number of subjects in this study was small. Sample size in the present study was estimated with reference to our past research [12]. This sample size was appropriate for comparing PPST between the MP group and the control group; however, it seemed to be insufficient for evaluating the relationship of PPST with age and duration of pain. Third, although the age of the two groups was matched as far as possible, they could not be completely matched. Further investigations should be designed taking these three limitations into consideration.
CONCLUSION
The results of the present study reveal that there was a significant difference in PPST between the MP group and the control group. Further investigation of PPST may further clarify the properties and etiology of occlusal dysesthesia.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Ethics Committee of Okayama University (No. 2084).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all individual participants included in the study.
CONFLICT OF INTEREST
No conflict of interest is disclosed. This work was supported by a Grant-in-Aid for Scientific Research (B) from the Japan Society for the Promotion of Science (24390433).
ACKNOWLEDGEMENTS
We thank Helen Jeays, BDSc AE, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.

